Download presentation
Presentation is loading. Please wait.

2
Hyperglycemia Management in the Hospital Tools to Make the Journey Safer & More Comfortable Bruce W. Bode, MD, FACE Atlanta Diabetes Associates Member of the SIG of GHA for Diabetes

3
Objectives l Understand the need for protocols for managing hyperglycemia and diabetes in the hospital l Present what the Georgia Hospital Association (GHA) has done to date and what tools we are using to accomplish this task l Discuss what tools are in development to make this journey easier
 has done to date and what tools we are using to accomplish this task l Discuss what tools are in development to make this journey easier")
4
GHA Special Interest Group for Diabetes l Formed in 2003 with the mission to monitor, evaluate and enhance diabetes care in the state of Georgia l Team composed of over 50 medical specialists with interest in diabetes care in the hospital l Team members are MDs, RNs, RDs, PharmDs, Administrators, Insurance Reps, etc

6
Key Elements of Inpatient Orders l Conforms with the current guidelines (AACE) l Simple and user friendly l Identifies patients needing initiation or modification of insulin therapy l Addresses the administration requirements for insulin infusion and the unique nutritional requirements l Addresses consultation/educational needs for patients
 l Simple and user friendly l Identifies patients needing initiation or modification of insulin therapy l Addresses the administration requirements for insulin infusion and the unique nutritional requirements l Addresses consultation/educational needs for patients")
7
The Increasing Rate of Diabetes Among Hospitalized Patients 48% Available at: http://www.cdc.gov/diabetes/statistics/dmany/fig1.htm. Accessed June 15, 2004.

8
Hyperglycemia in Hospitalized Patients l Hyperglycemia (>200 mg/dL x 2) occurred in 38% of hospitalized patients –26% had known history of diabetes –12% had no history of diabetes l Newly discovered hyperglycemia was associated with: –Longer hospital stays – higher admission rates to intensive care units –Less chance to be discharged to home (required more transitional or nursing home care) Umpierrez GE, et al. J Clin Endocrinol Metab. 2002;87:978–982.

9
Hospital Costs Account for Majority of Total Costs of Diabetes Hogan P, et al. Diabetes Care. 2003;26:917 – 932. Per Capita Healthcare Expenditures (2002) DiabetesWithout diabetes
 DiabetesWithout diabetes.")
10
Benefits of Improved Glucose Control in the Hospital l Aggressive insulin treatment improves –ICU outcomes –Outcomes post-MI –Cardiac surgery outcomes

11
Hospital Target Blood Glucose (mg/dL) l 80 – 110 in ICU patients l 80 – 140 in other Surgical and Medical Patients l 70 – 100 in Pregnancy Bode et al Endocrine Practice July 2004
 l 80 – 110 in ICU patients l 80 – 140 in other Surgical and Medical Patients l 70 – 100 in Pregnancy Bode et al Endocrine Practice July 2004")
12
Conclusion All hospital patients should have normal glucose

13
Insulin The agent we have to control glucose only most powerful

14
Methods For Managing Hospitalized Persons with Diabetes l Continuous Variable Rate IV Insulin Drip Major Surgery, NPO, Unstable, MI, DKA, Hyperglycemia, Steroids, Gastroparesis, Delivery, etc l Basal / Bolus Therapy (MDI) when eating
 when eating")
15
Threshold blood glucose in mg/dL for starting IV insulin infusion l Peri-operative care:> 140 l ICU care: > 110 - 140 * l Non-surgical illness:> 140 - 180 * * l Pregnancy> 100 * Van den Berghes study supports 110; Finneys study supports 145 * * If drip indication is failure of SQ therapy, use 180 ; if indication is specific condition ( DM 1/ NPO, MI, etc ), use 140
, use 140")
16
The Ideal IV Insulin Protocol l Easily ordered (signature only) l Effective (Gets to goal quickly) l Safe (Minimal risk of hypoglycemia) l Easily implemented l Able to be used hospital wide
 l Effective (Gets to goal quickly) l Safe (Minimal risk of hypoglycemia) l Easily implemented l Able to be used hospital wide")
17
Essentials of a good IV Insulin Algorithm l Easily implemented by nursing staff l Able to seek BG range via: - Hourly BG monitoring - Adjusts to the insulin sensitivity of the patient

18
Various Protocols Exist l DIGAMI (studied in acute MI setting) l van den Berghe (studied in critical care setting) l Portland Protocol (used in surgical setting) l Markovitz (studied in postoperative heart surgery patients) l Yale Protocol (studied in medical intensive care setting)
 l van den Berghe (studied in critical care setting) l Portland Protocol (used in surgical setting) l Markovitz (studied in postoperative heart surgery patients) l Yale Protocol (studied in medical intensive care setting)")
19
1. Start Portland protocol during surgery and continue through 7 AM of the third POD. Patients who are not receiving enteral nutrition on the third POD should remain on this protocol until receiving at least 50% of a full liquid or soft American Diabetes Association diet. 2. For patients with previously undiagnosed DM who have hyperglycemia, start Portland protocol if blood glucose is greater than 200 mg/dL. Consult endocrinologist on POD 2 for DM workup and follow-up orders. 3. Start infusion by pump piggyback to maintenance intravenous line as shown in Appendix Table 1. 4. Test blood glucose level by finger stick method or arterial line drop sample. Frequency of blood glucose testing is as follows: a. When blood glucose level greater than 200 mg/dL, check every 30 minutes. b. When blood glucose level is less than 200 mg/dL, check every hour. c. When titrating vasopressors, (eg, epinephrine) check every 30 minutes. d. When blood glucose level is 100 to 150 mg/dL with less than 15 mg/dL change and insulin rate remains unchanged for 4 hours (stable infusion rate), then you may test every 2 hours. e. You may stop testing every 2 hours on POD 3 (see items 1 and 8). f. At night on telemetry unit, test every 2 hours if blood glucose level is 150 to 200 mg/dL; test every 4 hours if blood glucose level is less than 150 mg/dL and stable infusion rate exists. 5. Insulin titration according to blood glucose level is performed as follows a. When blood glucose level is less than 50 mg/dL, stop insulin and give 25 mL 50% dextrose in water. Recheck blood glucose level in 30 minutes. When blood glucose level is greater than 75 mg/dL, restart with rate 50% of previous rate. b. When blood glucose level is 50 to 75 mg/dL, stop insulin. Recheck blood glucose level in 30 minutes; if previous blood glucose level was greater than 100 then give 25 mL 50% dextrose in water. When blood glucose level is greater than 75 mg/dL, restart with rate 50% of previous rate. c. When blood glucose level is 75 to 100 mg/dL and less than 10 mg/dL lower than last test, decrease rate by 0.5 U/h. If blood glucose level is more than 10 mg/Dl lower than last test, decrease rate by 50%. If blood glucose level is the same or greater than last test, maintain same rate. d. When blood glucose level is 101 to 150 mg/dL, maintain rate. e. When blood glucose level is 151 to 200 mg/dL and 20 mg/dL lower than last test, maintain rate. Otherwise increase rate by 0.5 U/h. f. When blood glucose level is greater than 200 mg/dL and at least 30 mg/dL lower than last test, maintain rate. If blood glucose level is less than 30 mg/dL lower than last test (or is higher than last test), increase rate by 1 U/h and, if greater than 240 mg/dL, administer intravenous bolus of regular insulin per initial intravenous insulin bolus dosage scale (see item 3). Recheck blood glucose level in 30 minutes. g. If blood glucose level is greater than 200 mg/dL and has not decreased after three consecutive increases in insulin, then double insulin rate. h. If blood glucose level is greater than 300 mg/dL for four consecutive readings, call physician for additional intravenous bolus orders. 6. American Diabetes Association 1800-kcal diabetic diet starts with any intake by mouth. 7. Postmeal subcutaneous Humalog insulin supplement is given in addition to insulin infusion when oral intake has advanced beyond clear liquids. a. If patient eats 50% or less of servings on breakfast, lunch, or dinner tray, then give 3 units of Humalog insulin subcutaneously immediately after that meal. b. If patient eats more than 50% of servings on breakfast, lunch, or supper tray, then give 6 units of Humalog insulin subcutaneously immediately after that meal. 8. On third POD, restart preadmission glycemic control medication unless patient is not tolerating enteral nutrition and is still receiving an insulin drip. Portland Protocol Furnary et al J Thorac Cardiovasc Surg 2003;123:1007-21
 check every 30 minutes. d. When blood glucose level is 100 to 150 mg/dL with less than 15 mg/dL change and insulin rate remains unchanged for 4 hours (stable infusion rate), then you may test every 2 hours. e. You may stop testing every 2 hours on POD 3 (see items 1 and 8). f. At night on telemetry unit, test every 2 hours if blood glucose level is 150 to 200 mg/dL; test every 4 hours if blood glucose level is less than 150 mg/dL and stable infusion rate exists. 5. Insulin titration according to blood glucose level is performed as follows a. When blood glucose level is less than 50 mg/dL, stop insulin and give 25 mL 50% dextrose in water. Recheck blood glucose level in 30 minutes. When blood glucose level is greater than 75 mg/dL, restart with rate 50% of previous rate. b. When blood glucose level is 50 to 75 mg/dL, stop insulin. Recheck blood glucose level in 30 minutes; if previous blood glucose level was greater than 100 then give 25 mL 50% dextrose in water. When blood glucose level is greater than 75 mg/dL, restart with rate 50% of previous rate. c. When blood glucose level is 75 to 100 mg/dL and less than 10 mg/dL lower than last test, decrease rate by 0.5 U/h. If blood glucose level is more than 10 mg/Dl lower than last test, decrease rate by 50%. If blood glucose level is the same or greater than last test, maintain same rate. d. When blood glucose level is 101 to 150 mg/dL, maintain rate. e. When blood glucose level is 151 to 200 mg/dL and 20 mg/dL lower than last test, maintain rate. Otherwise increase rate by 0.5 U/h. f. When blood glucose level is greater than 200 mg/dL and at least 30 mg/dL lower than last test, maintain rate. If blood glucose level is less than 30 mg/dL lower than last test (or is higher than last test), increase rate by 1 U/h and, if greater than 240 mg/dL, administer intravenous bolus of regular insulin per initial intravenous insulin bolus dosage scale (see item 3). Recheck blood glucose level in 30 minutes. g. If blood glucose level is greater than 200 mg/dL and has not decreased after three consecutive increases in insulin, then double insulin rate. h. If blood glucose level is greater than 300 mg/dL for four consecutive readings, call physician for additional intravenous bolus orders. 6. American Diabetes Association 1800-kcal diabetic diet starts with any intake by mouth. 7. Postmeal subcutaneous Humalog insulin supplement is given in addition to insulin infusion when oral intake has advanced beyond clear liquids. a. If patient eats 50% or less of servings on breakfast, lunch, or dinner tray, then give 3 units of Humalog insulin subcutaneously immediately after that meal. b. If patient eats more than 50% of servings on breakfast, lunch, or supper tray, then give 6 units of Humalog insulin subcutaneously immediately after that meal. 8. On third POD, restart preadmission glycemic control medication unless patient is not tolerating enteral nutrition and is still receiving an insulin drip. Portland Protocol Furnary et al J Thorac Cardiovasc Surg 2003;123:")
20
Leuven Protocol. Arterial BG q 1-2 hours, then q 4 hours if stable. If BG >220 give 4 units/hr. If BG >110 mg/dl give 2 units/hr.. If F/U BG in 1-2 hours >140 mg/dl Increase insulin 1-2 units/hr.. If F/U BG in 1-2 hours 121-140 mg/dl increase insulin 0.5-1 unit/hr.. If F/U BG 110-120 mg/dl increase insulin 0.1-0.15 units/hr.. If BG 81-110 mg/dl then do not change.. If BG decreases >50% decrease insulin 50%.. If BG 61-80 mg/dl decrease insulin reduced as dictated by previous BG level.. Repeat BG in one hour.. If B 41-60 mg/dl discontinue insulin.. If BG >40 mg/dl give 10 Gm glucose IV. Repeat q 1 hr until BG 81-110 mg/dl.. If BGT decreases >20% in 81-110 mg/dl range decrease insulin 20%.. If patient transferred from ICU and insulin <2 units/hr, DC insulin.. If patient transferred from ICU and insulin >2 units/hr get endocrine consult. Requires ICU nurses trained in protocol and study physician

21
A System for the Maintenance of Overnight Euglycemia and the Calculation of Basal Insulin Requirements in Insulin-Dependent Diabetics NEIL H. WHITE, M.D., DONALD SKOR, M.D., JULIO V. SANTIAGO, M.D.; Saint Louis, Missouri Ann Int Med 1982 ;97:210-214 Practical Closed Loop Insulin Delivery Slope = 0.02 = Multiplier 0 1 2 3 4 5 6 0100200300400 Glucose (mg/dl) Insulin Rate (U/hr) INSPIRATION FOR GLUCOMMANDER
 Insulin Rate (U/hr) INSPIRATION FOR GLUCOMMANDER.")
22
Continuous Variable Rate IV Insulin Drip l Mix Drip with 125 units Regular Insulin into 250 cc NS (0.5 U/cc) or 1 U/cc l Starting Rate Units / hour = (BG – 60) x 0.02 where BG is current Blood Glucose and 0.02 is the multiplier l Check glucose every hour and adjust drip l Adjust Multiplier to keep in desired glucose target range (80 to 110 in ICU; 100 to 140 on floor)
 or 1 U/cc l Starting Rate Units / hour = (BG – 60) x 0.02 where BG is current Blood Glucose and 0.02 is the multiplier l Check glucose every hour and adjust drip l Adjust Multiplier to keep in desired glucose target range (80 to 110 in ICU; 100 to 140 on floor)")
23
Continuous Variable Rate IV Insulin Drip l Adjust Multiplier (initially 0.02) to obtain glucose in target range 100 to 140 mg/dL If BG > 140 mg/dL and has not decreased by 15% in the last hour, increase by 0.01 If BG < 100 mg/dL, decrease by 0.01 If BG 100 to 140 mg/dL, no change in Multiplier l If BG is < 80 mg/dL, Give D50 cc = (100 – BG) x 0.4 l Give continuous rate of Glucose in IVFs l Once eating, continue drip till 2 hours post SQ insulin
 to obtain glucose in target range 100 to 140 mg/dL If BG > 140 mg/dL and has not decreased by 15% in the last hour, increase by 0.01 If BG < 100 mg/dL, decrease by 0.01 If BG 100 to 140 mg/dL, no change in Multiplier l If BG is < 80 mg/dL, Give D50 cc = (100 – BG) x 0.4 l Give continuous rate of Glucose in IVFs l Once eating, continue drip till 2 hours post SQ insulin")
29
Solution - Glucommander l Computer directed insulin infusion –Complexity is moved to the computer –Standardization is achieved Davidson et al, Diabetes Care 28(10): 2418-2423, 2005
: , 2005")
30
Glucommander History l 1982 Paul Davidson develops protocols for intravenous insulin l 1984 Dennis Steed writes Glucommander program based on Davidsons protocols l Used in multiple hospitals throughout US –Approximately 130 Davidson et al, Diabetes Care 28(10): 2418-2423, 2005
: , 2005")
31
Glucommander History l Version 1 – prototype, never used l Version 2 – 1984, ran infusion pump l Version 3 – 1985, new multiplier adjustment algorithm l Version 4 – 1992, double entry of BG, nurse runs infuser Davidson et al, Diabetes Care 28(10): 2418-2423, 2005
: , 2005")
32
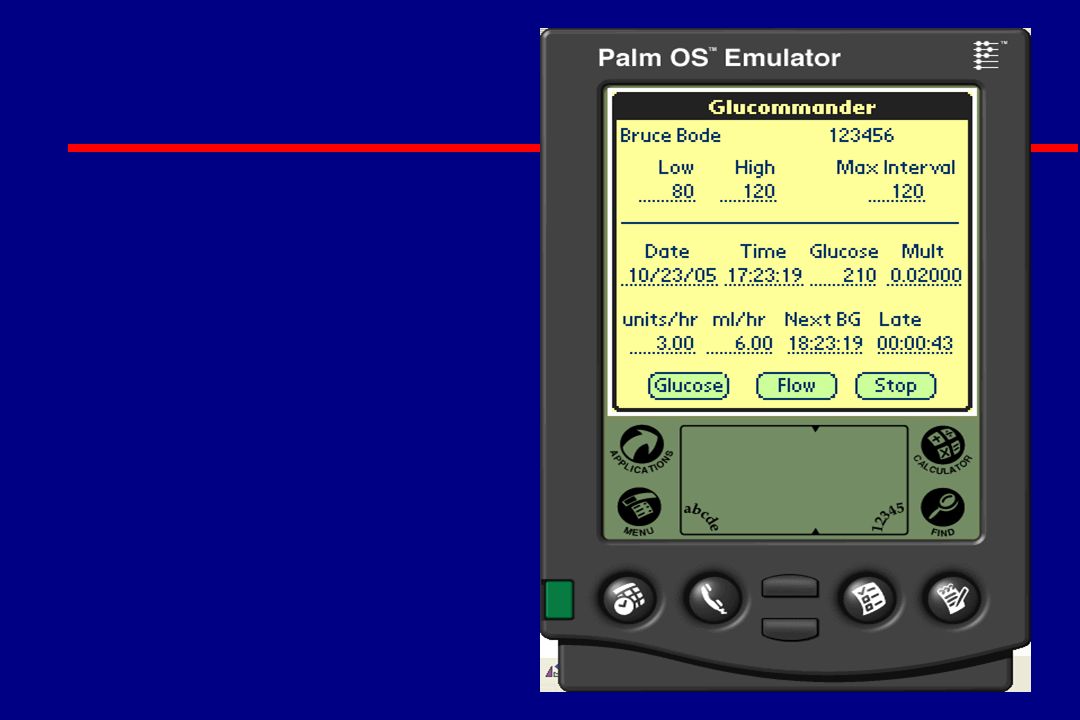
Glucommander Algorithm l Insulin (u/hr) = multiplier x (BG – 60) l Blood glucose checked periodically –Variable interval based on BG stability –Typically hourly l Multiplier adjusted to seek target range Davidson et al, Diabetes Care 28(10): 2418-2423, 2005
 = multiplier x (BG – 60) l Blood glucose checked periodically –Variable interval based on BG stability –Typically hourly l Multiplier adjusted to seek target range Davidson et al, Diabetes Care 28(10): , 2005")
33
Glucommander Principles Insulin Units / Hour Glucose mg / dl Davidson et al, Diabetes Care 28(10): 2418-2423, 2005
: , 2005")
34
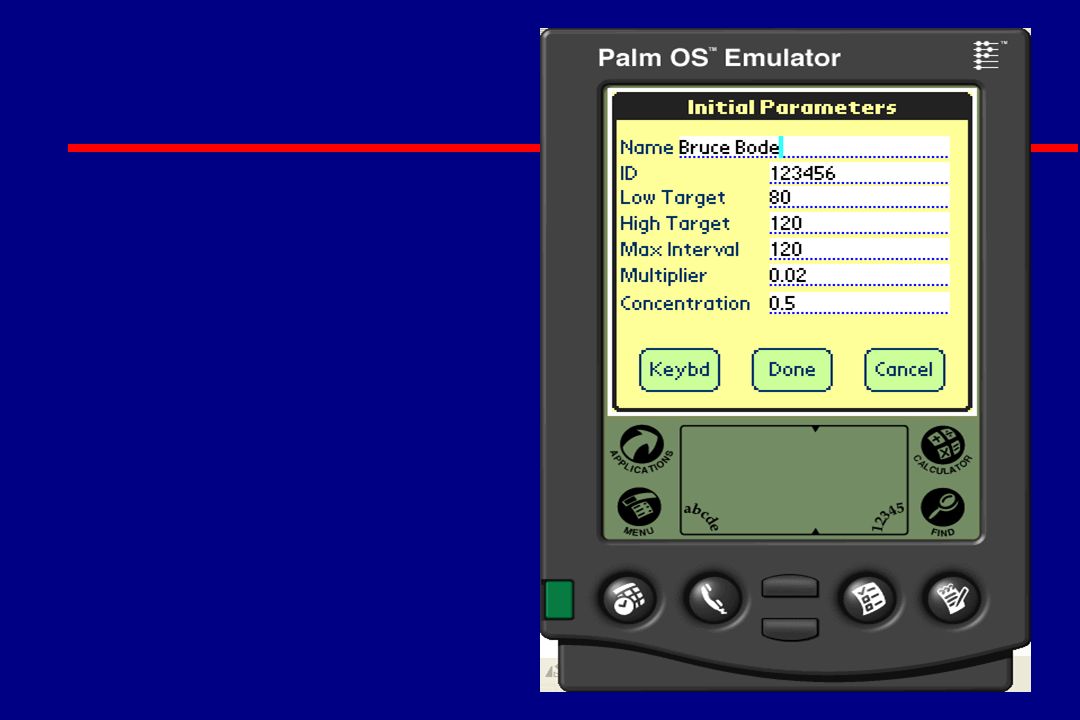
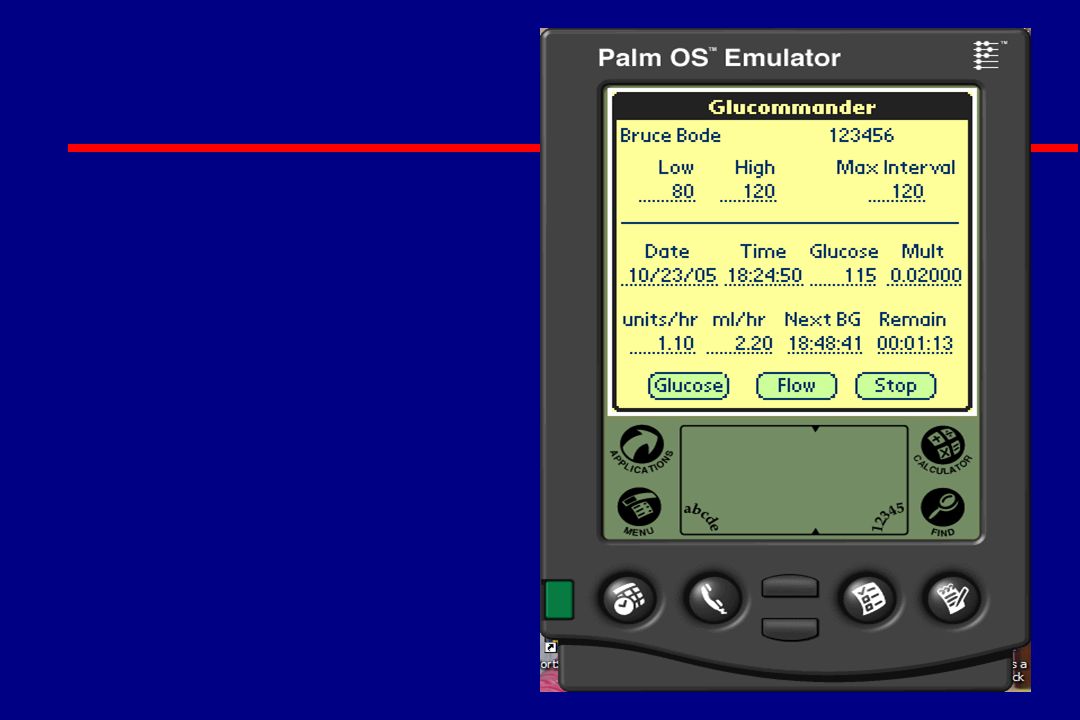
Physician View – Writing orders l High Target Glucose l Low Target Glucose l Multiplier l Maximum interval l Insulin concentration

35
Glucommander Setttings– Default ICU l High Target Glucose: 110 mg/dL l Low Target Glucose: 80 mg/dL l Multiplier: 0.02 l Maximum interval: 120 minutes l Insulin concentration: 0.5 units per ml

36
Glucommander Setttings– Default Floor l High Target Glucose: 120 mg/dL l Low Target Glucose: 100 mg/dL l Multiplier: 0.02 l Maximum interval: 120 minutes l Insulin concentration: 0.5 units per ml

37
Glucommander Setttings– Default OB Floor l High Target Glucose: 100 mg/dL l Low Target Glucose: 70 mg/dL l Multiplier: 0.04 l Maximum interval: 120 minutes l Insulin concentration: 0.5 units per ml

38
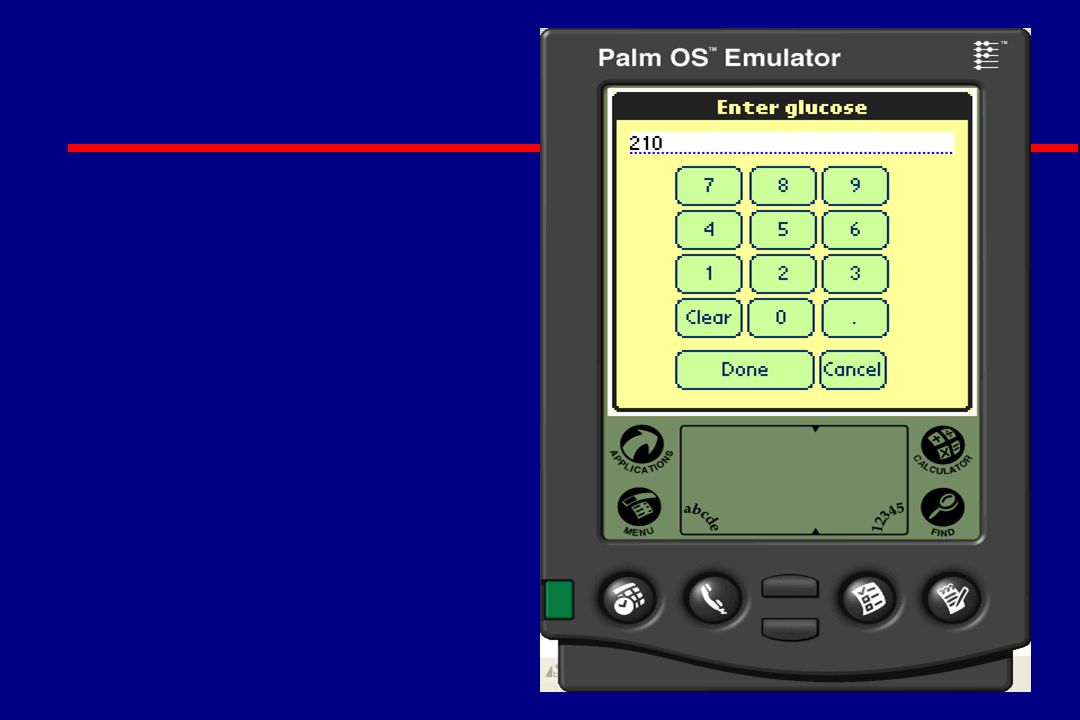
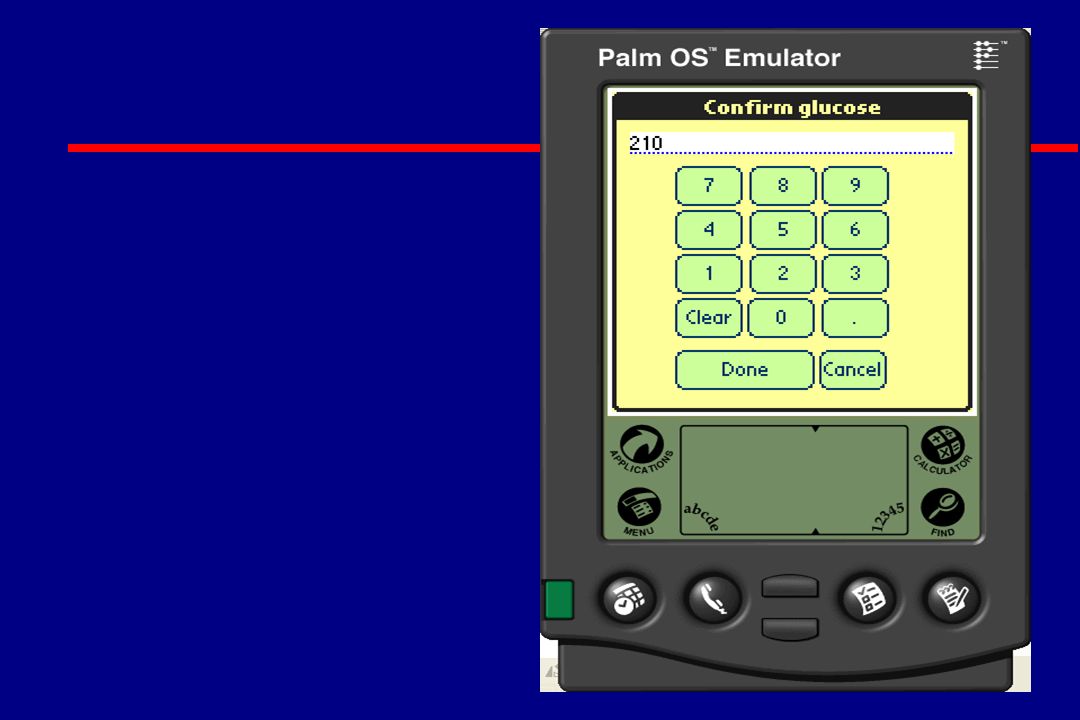
Nurse View of Glucommander l Computer periodically alarms l Check blood glucose l Enter glucose into computer l Set insulin drip to rate from computer l Eliminates calls to the physician

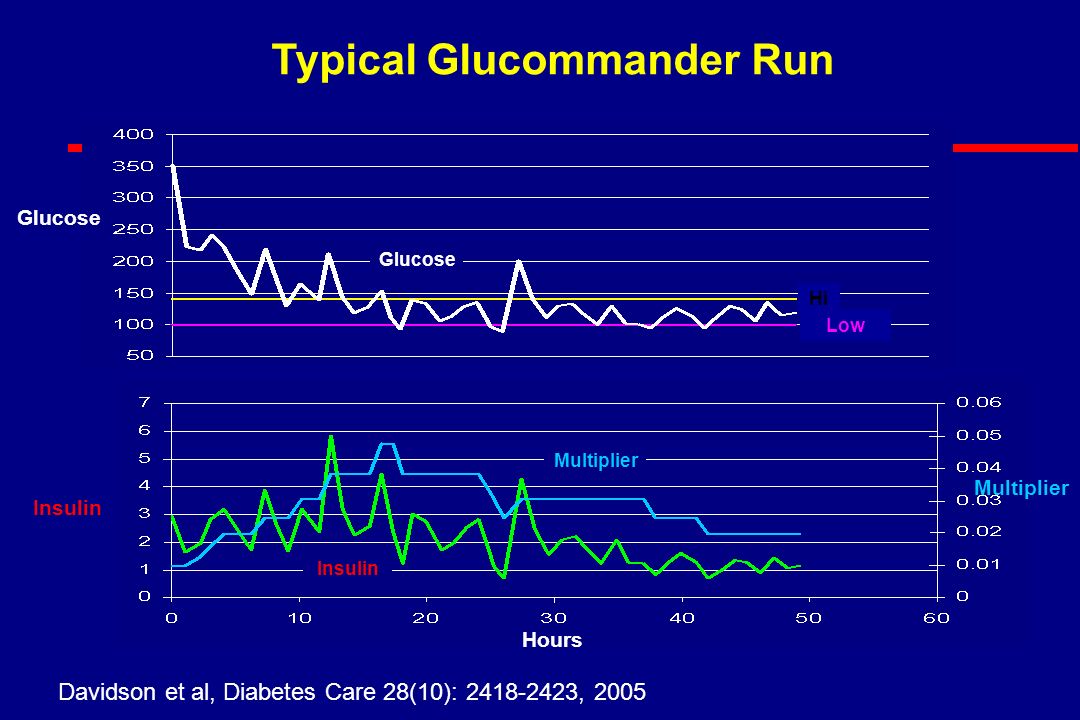
59
Hours Glucose Multiplier Insulin Glucose Typical Glucommander Run Hi Low Davidson et al, Diabetes Care 28(10): 2418-2423, 2005
: , 2005")
60
Database l Collected all uses of Glucommander 1984- 1998 l 5803 runs l 120618 timed glucose / insulin pairs Davidson et al, Diabetes Care 28(10): 2418-2423, 2005
: , 2005")
61
Average and Standard Deviation of of All Runs Davidson et al, Diabetes Care 28(10): 2418-2423, 2005
: , 2005")
62
Treating to Target Range

63
Conformity of Blood Glucose to Glucommander Target

64
Low Range (v4)
")
65
How has the Glucommander been used? l Treatment of ketoacidosis l Hyperosmolar non-ketotic state l Perioperative glucose management l Labor and delivery l Myocardial infarction l Critically ill patients in ICU l Hyperalimentation l Gastroparesis with intractable nausea and vomiting l Estimating a patients insulin sensitivity –A guide for dosing insulin Estimating total insulin dose, correction factor, CHO/Ins Davidson et al, Diabetes Care 28(10): 2418-2423, 2005
: ,")
66
Transition from Glucommander to Subcutaneous Insulin l 24-hour insulin requirement –Multiplier X 1000 = TDD l Give one-half TDD as basal (Glargine) –Multiplier X 500 = BI l Give rapid acting insulin based on CHO consumed –0.5 / multiplier = CIR (Gms CHO / unit) or –30 X multiplier = units / CHO exchange l Monitor BG a.c. t.i.d., h.s., and 3 am l Correct all BG > 140 mg/dL –(BG - 100) / (1.7 / multiplier)
 / (1.7 / multiplier).")
67
Computerized Hospital Insulin Infusion Project (CHIIP) l Quality improvement Initiative –Initially based on current Glucommander –Multiple hospitals –Common outcomes database –Track response to algorithm changes –Publish progress reports
 l Quality improvement Initiative –Initially based on current Glucommander –Multiple hospitals –Common outcomes database –Track response to algorithm changes –Publish progress reports")
68
Computerized Hospital Insulin Infusion Project (CHIIP) l Currently exploring funding –Grants Government Industry –Membership fees
 l Currently exploring funding –Grants Government Industry –Membership fees")
69
1 Center Experience with Glucommander over a 1 year period (2004 to 2005) l East Carolina University – 750 bed hospital with 7 ICUs l Glucommander initiated in all ICU patients with BG >140 mg/dL l 7 FTEs hired to implement the program l Average BG went from 167 to 126 mg/dl l LOS decreased in ICU by 1 day; in Hospital by 0.3 days l No central line infections l Net savings to hospital 2 million dollars (470% Return on Investment) Personal Communication with Chris Newton, MD FACE
 l East Carolina University – 750 bed hospital with 7 ICUs l Glucommander initiated in all ICU patients with BG >140 mg/dL l 7 FTEs hired to implement the program l Average BG went from 167 to 126 mg/dl l LOS decreased in ICU by 1 day; in Hospital by 0.3 days l No central line infections l Net savings to hospital 2 million dollars (470% Return on Investment) Personal Communication with Chris Newton, MD FACE")
70
Current Status Of Glucommander l Being studied in 8 hospitals vs Hirsh et al drip l Discussions are on going with several groups to bring the device to all interested hospitals l Available for research purposes via www.glucommander.com

72
Converting to SC insulin l If More than 0.5 u/hr IV insulin required with normal BG, start long-acting insulin (glargine) Exception: if no prior DM and normal A1C, may not need SC insulin Exception: if no prior DM and normal A1C, may not need SC insulin l Must start SC insulin at least 1 to 2 hours before stopping IV insulin l Some centers start long-acting insulin on initiation of IV insulin or the night before stopping the drip
 Exception: if no prior DM and normal A1C, may not need SC insulin Exception: if no prior DM and normal A1C, may not need SC insulin l Must start SC insulin at least 1 to 2 hours before stopping IV insulin l Some centers start long-acting insulin on initiation of IV insulin or the night before stopping the drip")
73
Intravenous Insulin Infusion Under Basal Conditions Correlates Well With Subsequent Subcutaneous Insulin Requirement Hawkins et al. Endocr Pract. 1995;1:385–389. Units IV Units SQ Total Intravenous vs. Subcutaneous 24-hour Insulin Requirements, units 275 250 225 200 175 150 125 100 75 50 25 0 2752502252001751501251007550250

74
The Physiological Insulin Profile Adapted from Polonsky, et al. 1988. 10 20 30 Insulin (mU/l) 0 40 50 60 70 Short-lived, rapidly generated prandial insulin peaks Low, steady, basal insulin profile Normal free insulin levels from genuine data (mean) 060009001200150018002100240003000600 BreakfastLunchDinner
 Short-lived, rapidly generated prandial insulin peaks Low, steady, basal insulin profile Normal free insulin levels from genuine data (mean) BreakfastLunchDinner.")
75
4:0016:0020:0024:004:00 BreakfastLunchDinner 8:00 12:008:00 Time Glargine or Detemir Lispro Lispro Lispro Aspart, Aspart, Aspart, or Plasma insulin Basal/Bolus Treatment Program with Rapid-acting and Long-acting Analogs Glulisine Glulisine Glulisine

76
Initiating SC Basal Bolus l Starting total dose = 0.5 x wgt. in kg Wt. is 100 kg; 0.5 x 100 = 50 units l Basal dose (glargine) = 50% of starting dose at HS 0.5 x 50 = 25 units at HS l Bolus doses (aspart / lispro) = 50% of starting dose 0.5 x 50 = 25 divided by 3 = ~8 units pc (tid) l Correction bolus = (BG - 100)/ CF, where CF = 1700/total daily dose; CF = 30
 = 50% of starting dose at HS 0.5 x 50 = 25 units at HS l Bolus doses (aspart / lispro) = 50% of starting dose 0.5 x 50 = 25 divided by 3 = ~8 units pc (tid) l Correction bolus = (BG - 100)/ CF, where CF = 1700/total daily dose; CF = 30.")
79
Protocol for Treatment of Hypoglycemia l Any BG <80 mg/dl: D50 = (100-BG) x 0.4 ml IV l Recheck in 15 minutes and retreat if needed l If eating, may use 15 gm of rapid CHO (prefer glucose tablets) (prefer glucose tablets) l Do Not Hold Insulin When BG Normal
 x 0.4 ml IV l Recheck in 15 minutes and retreat if needed l If eating, may use 15 gm of rapid CHO (prefer glucose tablets) (prefer glucose tablets) l Do Not Hold Insulin When BG Normal")
83
Hospital Diabetes Plan What Can We Do For Patients Admitted To Hospital? l Pathway Protocols For All Hyperglycemia and Diabetes Patients l Finger Stick BG ac qid on ALL Admissions with BG >140 mg/dL or history of DM or high risk (ICU, Cardiac, Vascular, CVA, etc) l Check All Steroid Treated Patients l Diagnose Diabetes FBG >126 mg/dl Any BG >200 mg/dl
 l Check All Steroid Treated Patients l Diagnose Diabetes FBG >126 mg/dl Any BG >200 mg/dl.")
84
Hospital Diabetes Plan What Can We Do For Patients Admitted To Hospital? l Document Diagnosis in Chart Hyperglycemia Is Diabetes Until Proven Bring to All Physicians Attention Note on Problem List and Face Sheet l Check Hemoglobin A1C in all hyperglycemic patients l Hold Metformin; Hold TZD with CHF l Start Insulin in All Hospitalized Patients with BG >140 mg/dl

85
l Treat Any Patient With BG >140 mg/dl With Insulin –Treat Any BG >140 mg/dl with Rapid-acting Insulin (BG-100) / (3000 / wt kg) or 1700 / total daily insulin –Treat Any Recurrent BG >180 mg/dl with IV Insulin if failing SC therapy or >110 to 140 mg/dl if NPO, acute MI, perioperative, ICU, or >100 mg/dl if pregnant l If More than 0.5 u/hr IV Insulin Required with Normal BG Start Long Acting Insulin Hospital Diabetes Plan Protocol for Insulin in Hospitalized Patient
 / (3000 / wt kg) or 1700 / total daily insulin –Treat Any Recurrent BG >180 mg/dl with IV Insulin if failing SC therapy or >110 to 140 mg/dl if NPO, acute MI, perioperative, ICU, or >100 mg/dl if pregnant l If More than 0.5 u/hr IV Insulin Required with Normal BG Start Long Acting Insulin Hospital Diabetes Plan Protocol for Insulin in Hospitalized Patient")
86
Hospital Diabetes Plan Protocol for Insulin in Hospitalized Patient Hospital Diabetes Plan Protocol for Insulin in Hospitalized Patient l Daily Total: Pre-Admission or Weight (kg) x 0.5 u –50% as Glargine (Basal) –50% as Total Rapid-acting insulin (Bolus) Give in Proportion to Meals CHO EatenGive in Proportion to Meals CHO Eaten l BG >140 mg/dl: (BG-100) / CF CF = 1700 / Total Daily Insulin or 3000 / Wt (kg) Do Not Use Sliding Scale As Only Diabetes Management
 x 0.5 u –50% as Glargine (Basal) –50% as Total Rapid-acting insulin (Bolus) Give in Proportion to Meals CHO EatenGive in Proportion to Meals CHO Eaten l BG >140 mg/dl: (BG-100) / CF CF = 1700 / Total Daily Insulin or 3000 / Wt (kg) Do Not Use Sliding Scale As Only Diabetes Management")
87
Hospital Diabetes Plan What Can We Do For Patients Admitted To Hospital? l Get Diabetes Education Consult l Instruct Patient in Monitoring and Recording See That Patient Has Meter on Discharge l Decide on Case Specific Program for Discharge l Arrange Early F/U with PCP

88
Conclusion l Our journey is not over, it has only begun l We must normalize glucose in all hospital patients l By implementing, assessing and revising protocols/pathways for hyperglycemic management, we can achieve this ultimate goal of normal glycemia

89
Future Devices l Pens and Pen safety needles l Continuous glucose sensors (SC and IV) l Patch insulin pumps l Closed loop systems for both IV and SC insulin delivery
 l Patch insulin pumps l Closed loop systems for both IV and SC insulin delivery")
90
Insulin Pens The first insulin pen was developed by NovoNordisk in 1926 but not launched until 1985. Since then, numerous pens, both disposable and reusable, have been developed adding to accuracy in dosing and convenience to insulin injection therapy. Disposable Lilly Pen Novo Reusable Pen with disposable cartridge Disposable NovoNordisk Pen Aventis Reusable Pen with disposable cartridge

91
NovoFine ® AutocoverSteps for Use For training purposes only. Not to be distributed. Step 1Step 2Step 3

92
Photograph reproduced with permission of manufacturer. Current Insulin Pumps

93
Pump infusion sets: perpendicular vs oblique Perpendicular (Sof-set, Quick-set, Ultraflex) - Easier insertion - Prone to kink Oblique (Silouette, Tender, Comfort) - More difficult insertion - Less kinking
 - Easier insertion - Prone to kink Oblique (Silouette, Tender, Comfort) - More difficult insertion - Less kinking")
94
Disposable Patch Pumps

95
Continuous Monitoring Systems Medtronic MiniMed CGMS Guardian RT DexCom Abbott Navigator

96
Implanted Closed-Loop External Closed-Loop Vision towards the Artificial Pancreas * This product concept not yet submitted to the FDA for commercialization.

97
For Further Information l Guidelines –American Academy of Clinical Endocrinology: www.aace.com/pub/ICC/inpatientStatement l Protocols –Georgia Hospital Association: www.gha.orgwww.gha.org –Atlanta Diabetes Associates: www.adaendo.comwww.adaendo.com –Glucommander: www.glucommander.com

Similar presentations































![INSULIN THERAPY IN ICU Dr SANJAY KALRA, D.M. [AIIMS]](/1/259452/big_thumb.jpg "INSULIN THERAPY IN ICU Dr SANJAY KALRA, D.M. [AIIMS]>")









>")



