Download presentation
Presentation is loading. Please wait.

1
HEART AND MUSCLE PARASITES

2
Taenia solium: life cycle

3
Taenia solium; cysticercosis: Calcified cysticerci in muscle.

4
Trichinella spiralis: life cycle

5
Trichinella spiralis migrating larvae

6
Trichinella spiralis encapsulted larvae

7
Trichinella spiralis calcified larvae

8
Trichinella spiralis larvae encysted in striated muscle

9
Trichinella spiralis larvae

10
Trichinella spiralis electron microscopy

13
B A

14
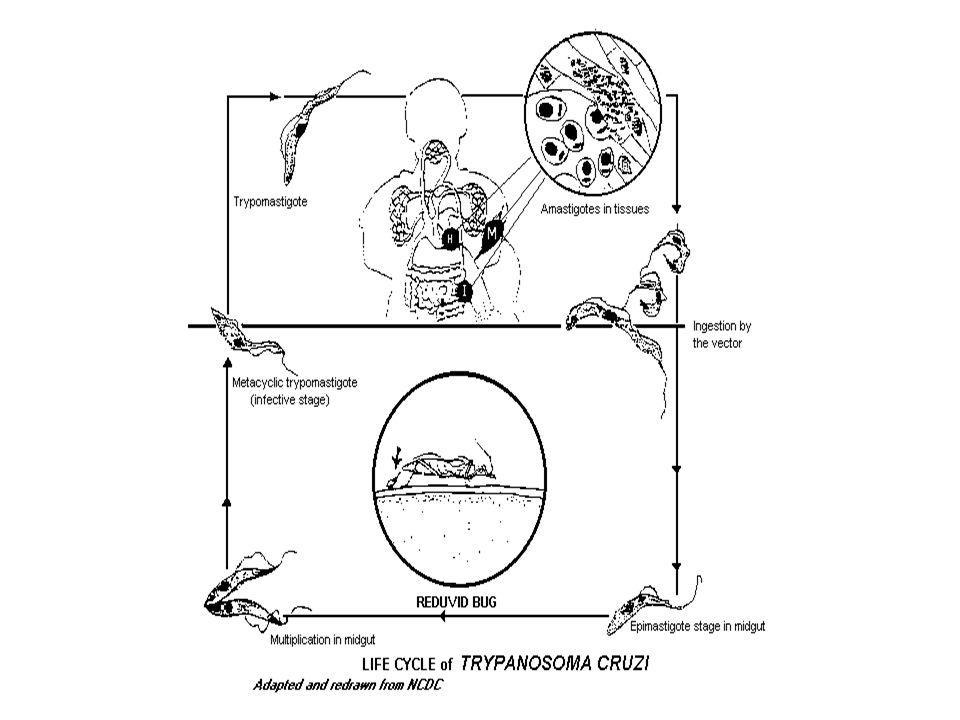
A. T.cruzi parasitize mainly the cardiac muscle but any cell type may be parasitized:cardiac muscle with amastigotes, H&E stain. B. Chagas' disease megacardia C. Apical aneurysm in Chagas' disease A B C

15
A. Chagasic megacolon with enlargement of the sigmoid B
A. Chagasic megacolon with enlargement of the sigmoid B. X-ray showing megaoesophagus in Chagas' disease C. X-ray showing megacolon in Chagas' disease

16
T. cruzi: can be observed in the peripheral blood only in the acute case of the disease. Its presence is the best definition of the acute phase as all other signs are variable. A T.cruzi trypomastigote: blood stream trypomastigotes are µm in lenght and appear with a typical C or S-shaped form. B In vitro infected fibroblast showing a large number of intracellular amastigotes. C

17
PARASITES INTESTINAL PARASITES

19
A.lumbricoides egg: regular fertile egg with a thick outer mammillated coat: eggs measure by µm and have a yellow to brown colour. (Formol-ether concentration).
..")
20
A.lumbricoides: embryonated egg having a second stage (L2) larva.
 larva.")
21
A.lumbricoides unfertile egg: the unfertile eggs are elongated and much larger (85-95x43-47 µm); they have a thin shell, an irregular, mammillated outer layer and a granular contents.
; they have a thin shell, an irregular, mammillated outer layer and a granular contents.")
22
Ascaris sp.

25
A B A. A.lumbricoides: immature or adult A.lumbricoides are sometimes passed in stools. Adult males measure cm in length by cm in diameter and have a ventrally curved tail; adult females measure cm in length by 0.5 cm in diameter. Adult female B. Adult Ascaris lumbricoides seen outlined in barium meal Xray of abdomen.

27
Enterobius vermicularis: gravid female worm.

28
Enterobius vermicularis: posterior end of a female
Enterobius vermicularis: posterior end of a female. Observe the eggs expelled by the worm in the field and the long, pointed tail (hence the name of Pinworm). (20 x, mounted in glycerine jelly)
. (20 x, mounted in glycerine jelly)")
29
Enterobius vermicularis: egg in human faeces (wet mount preparation)
")
30
Enterobius vermicularis: eggs are thin shelled, ovoid and flattened on one side and measure by µm; they often are embrionated.

31
Enterobius vermicularis: scotch-tape smear showing an egg of E
Enterobius vermicularis: scotch-tape smear showing an egg of E.vermicularis and some eggs of Taenia spp.

32
Enterobius vermicularis: eggs are thin shelled, ovoid and flattened on one side and measure by µm; they often are embrionated.

34
Strongyloides stercoralis
In the indirect development cycle several reproductive cycle of the free-living forms can occur; they produce eggs (40-70 µm) which can develop into rhabditiform larvae and into infectious third stage larvae; this life-cycle takes several weeks to be completed. The free living females measure about 1 mm in lenght by µm: a) a free living female containing embryonated eggs; b) the free living females have a rhabdithoid esophagus; c) eggs within the free-living female.
 which can develop into rhabditiform larvae and into infectious third stage larvae; this life-cycle takes several weeks to be completed. The free living females measure about 1 mm in lenght by µm: a) a free living female containing embryonated eggs; b) the free living females have a rhabdithoid esophagus; c) eggs within the free-living female.")
35
Rhabditoid larvae of Strongyloides stercoralis in faeces
Rhabditoid larvae of Strongyloides stercoralis in faeces. Wet mount preparation of unconcentrated faeces during hyperinfection.

36
Filariform larvae (L3) penetrate the skin by releasing hydrolitic enzymes, enter dermal vessels and migrate through the blood or lymphatic channels to the hearth and lungs. Filariform larvae measure µm in lenght by µm. Fecal culture of S.stercoralis larvae, filter paper technique, wet mount preparation.

37
The prepatent period (the time between infection and the recovering of larvae in faeces) lasts about 1 month; infections may persist for over 30 years. In the intestinal lumen rhabditiform larvae may directly transform in filariform larvae; here they may penetrate the colonic mucosa or the perianal skin causing autoinfection. Autoinfection explains the long duration of the infection and the possible multiplication within the host (hyperinfection). Filariform larvae are slender and have a notched tip of the tail. Fecal culture of S. stercoralis larvae, filter paper technique, wet mount preparation.
. Filariform larvae are slender and have a notched tip of the tail. Fecal culture of S. stercoralis larvae, filter paper technique, wet mount preparation.")
38
A. The common manifestations of the disseminated hyperinfection are diarrhea, sepsis, severe pneumonia with alveolar hemorrhage, meningitis with or without brain abscesses and purpura. Disseminated S.stercoralis hyperinfection: section of lung showing hemorrhagic pneumonia. (H & E stain). A thickening of the alveolar walls, an inflammatory infiltrate with eosinophils and sections of filariform larvae can be observed. This form of infection is usually fatal (50-75% of all cases) even with timely treatment. B. Disseminated S.stercoralis hyperinfection: section of lung showing hemorrhagic pneumonia. (H & E stain). Red cells, eosinophils and sections filariform larvae observed within an alveolus. C. Chest radiography shows bilateral confluent interstitial and alveolar infiltrates. Successful treatment of hyperinfection requires a prompt diagnosis and a timely initiation of antihelmintic (Thiabendazole, Ivermectine) and antibiotic therapy. Disseminated S.stercoralis hyperinfection. Chest radiography.
 and antibiotic therapy. Disseminated S.stercoralis hyperinfection. Chest radiography.")
40
Hookworm rhabditoid larva, fresh examination.
Hookworm: rhabditoid larvae can be differentiated by the long buccal cavity and the lack of genital primordium typical of S.stercoralis larvae.

41
Image of the adult worm Ancylostoma duodenale adults in gut (preserved post mortem specimen)
")
42
A. Ancylostoma duodenale:
anterior end of a male of Ancylostoma spp.. Observe its strong buccal capsule and the muscular oesophagus. (20 X in glycerine jelly) B. Ancylostoma duodenale: the intestine is wounded around the genital tube. (20 X in glycerine jelly)
 B. Ancylostoma duodenale: the intestine is wounded around the genital tube. (20 X in glycerine jelly)")
43
A B A. Hookworm: egg found in faeces are oval or can-shaped with a thin, hyaline shell; they measure by µm B. Necator americanus: egg. Almost indistinguishable, the eggs of Necator americanus are a little bit longer than Ancylostoma duodenale. Note the extremely thin shell. (1.000 X)
")
45
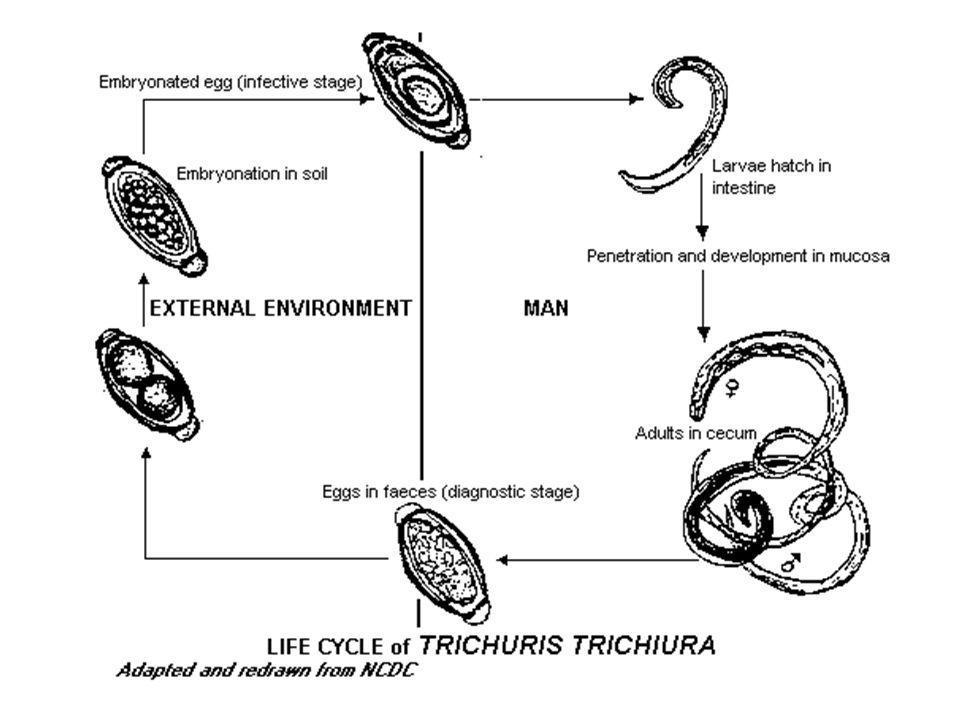
Trichuris trichiura: a macroscopic view of a tangled mass of adults (male and female) in pure glycerine. The adult female measures about mm in length, and the male about mm.

46
Trichuris trichiura adults in gut (preserved post mortem specimen)
")
47
A B A. Trichuris trichiura: vulvar region. (10 X in glycerine jelly) B. Trichuris trichiura: higher magnification of the figure 371 (20 X)
 .")
48
Trichuris trichiura: detail of bipolar prominences.

50
Hymenolepis nana: typical egg, measuring between 30 and 47 µm in diameter, containing an oncosphere with an internal cover with polar thickenings and 6 hooks (1.000 X).
.")
51
Taenia spp. (saginata and solium), adult worm: the chain of proglottides is called the strobila, and may be composed of over proglottides. T.saginata may measure 9 m, whereas T.solium may reach 6 m.
, adult worm: the chain of proglottides is called the strobila, and may be composed of over proglottides. T.saginata may measure 9 m, whereas T.solium may reach 6 m..")
52
Taenia spp. (saginata and solium): detail of an adult tapeworm, mature proglottides. Gravid T.saginata proglottides measure 19 by 7 mm and have uterine branches. T.solium proglottides measure 11 x 5-8mm and have 7-12 uterine branches. The scolex is square, 1-2 mm in diameter with 4 suckers. T.solium scolex has a rostellum with hooklets.

53
Taenia spp. (saginata and solium): eggs of the two species are identical, spherical (31-43 µm), brown to dark-yellow with a thick shell wall and contain an onchosphere.
: eggs of the two species are identical, spherical (31-43 µm), brown to dark-yellow with a thick shell wall and contain an onchosphere..")
54
Taenia spp. (T. saginata and T
Taenia spp. (T.saginata and T.solium): tapeworm eggs in scotch test preparation.
: tapeworm eggs in scotch test preparation.")
55
Taenia spp. (T. saginata and T
Taenia spp. (T.saginata and T.solium): cross-section of gravid proglottis of Taenia spp. observed in the appendix; numerous eggs are visible within the uterus of the gravid proglottis. (H&E, 250 X)
: cross-section of gravid proglottis of Taenia spp. observed in the appendix; numerous eggs are visible within the uterus of the gravid proglottis. (H&E, 250 X)")
56
Taenia spp. (T. saginata and T
Taenia spp. (T.saginata and T.solium): cross-section of gravid proglottis of Taenia spp. observed in the appendix; numerous eggs are visible within the uterus of the gravid proglottis. (H&E, 400 X)
: cross-section of gravid proglottis of Taenia spp. observed in the appendix; numerous eggs are visible within the uterus of the gravid proglottis. (H&E, 400 X)")
57
Taenia spp. (T. saginata and T
Taenia spp. (T.saginata and T.solium): cross-section of gravid proglottis of Taenia spp. observed in the appendix; egg within the uterus of the gravid proglottis. (H&E, X)
: cross-section of gravid proglottis of Taenia spp. observed in the appendix; egg within the uterus of the gravid proglottis. (H&E, X)")
59
Diphyllobothrium latum : eggs are operculated, measure by µm. A small knob is visible at the opposite site of the operculum.

61
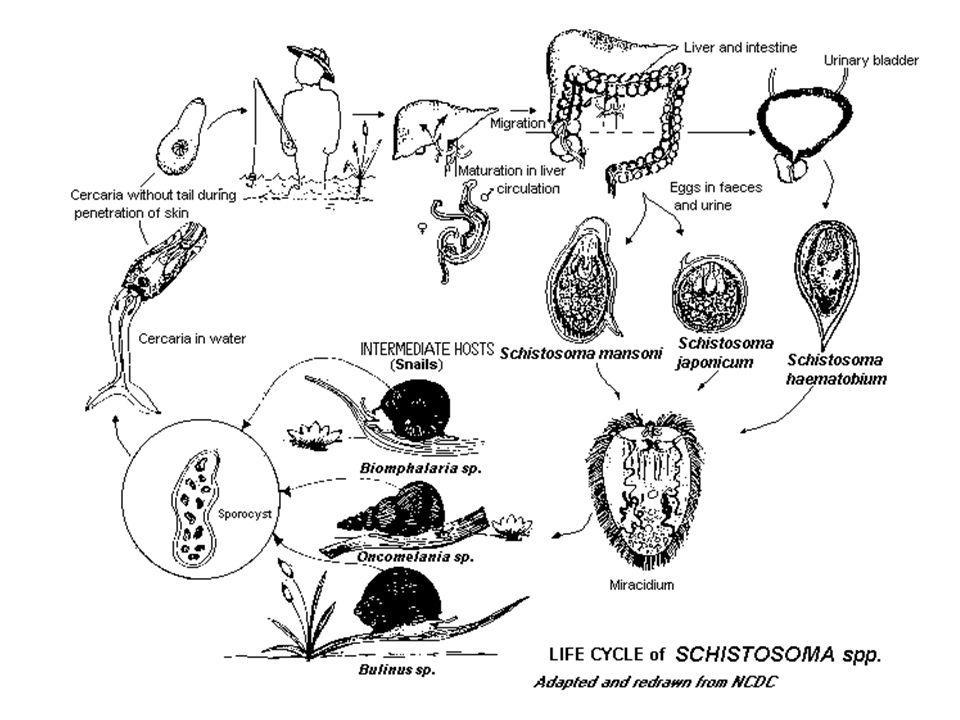
Schistosoma spp. : cercarae are the infective forms
Schistosoma spp.: cercarae are the infective forms. They measure about 500 micron. After encountering the skin, the cercariae penetrate and lose the tail transforming into schistosomulae.

62
S. mansoni: intermediate host of S
S.mansoni: intermediate host of S. mansoni are snails of the genus Biomphalaria.

63
S.mansoni egg: egg with typical spine in stools (formol-ether concentration). Demonstration of eggs in faeces and urine is the standard method of diagnosis of schistosomiasis. Sensitivity of one stool examination does not exceed 60%.

64
S. mansoni egg: lateral spine at higher magnification
S.mansoni egg: lateral spine at higher magnification. Other diagnostic methods include intestinal or liver biopsy. Serology is useful in travellers from endemic areas before shedding of eggs or in extraintestinal forms (spinal) but not in natives.
 but not in natives.")
65
S.mansoni: adult schistosomes live in pairs in the portal system and in the mesenteric venules; males are shorter (7-12 mm in lenght and 2 mm wide) and have a ventral infolding from the ventral sucker to the posterior end forming the gynecophoric canal. Adult male with female in the copulatory groove.

66
S.mansoni: Cross-section of granulomas around eggs of Schistosoma mansoni observed in the appendix.

67
S. mansoni: hepatosplenic schistosomiasis occurs in S. mansoni and S
S.mansoni: hepatosplenic schistosomiasis occurs in S.mansoni and S.japonicum infections; it results by eggs embolization in hepatic venules with formation of granulomas and portal fibrosis. Hepatosplenomegaly, bleeding oesophageal varices and hepatic insufficiency are the more severe manifestations. Praziquantel is the drug of choice. Liver biopsy: egg surrounded by granuloma and fibrosis of portal space.

68
Polyposis due to S.mansoni infection.

69
Splenomegaly and portal hypertension and ascites due to S.mansoni.
due to infection with S.mansoni.

70
S.japonicum egg: eggs are usually round and have a small spine or no spine. Other small knobby-spined or not spined schistosomes that affect humans are S.mekongi and S.malaysiensis.

71
S. japonicum: intermediate host of S
S.japonicum: intermediate host of S.japonicum are snails of the genus Onchomelania, hupensis spp.

73
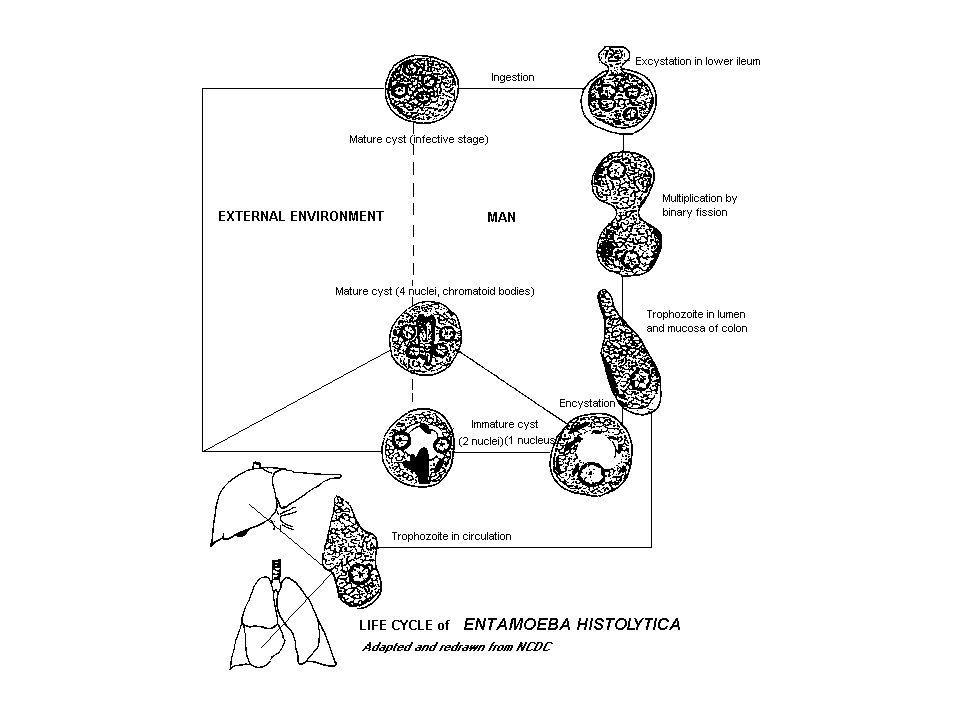
E. histolytica: cysts with 4 visible nuclei
E.histolytica: cysts with 4 visible nuclei. One cyst contains also elliptical chromidial body. The mature quadrinucleate cyst measures 8-15 µm in diameter. Stained fecal film. Wheatley modification of Gomori‘s trichrome technique. Objective 100 X

74
A. B. A. Entamoeba.histolytica cyst: cysts measure µm in diameter and are spherical. (Iodine stain). B. Entamoeba histolytica: cyst, Gomori's trichrome (1.000 X)
")
75
E. histolytica: trophozoite of E. histolytica forma minuta
E.histolytica: trophozoite of E.histolytica forma minuta µm in diameter. Stained fecal film. Wheatley modification of Gomori‘s trichrome technique. Objective 100 X

76
E.histolytica: trophozoite of E.histolytica forma magna (dysenterica) µm in diameter, with ingested erythrocytes in the endoplasm. Stained fecal film. Wheatley modification of Gomori‘s trichrome technique. Objective 100 X

77
E.histolytica, hepatic abscess: amebic trophozoites may reach the liver via the portal vein. Dissemination to lung, brain and skin may also take place.

78
The colonic mucosa is invaded by amoebae with lysis of inflammatory cells and tissue necrosis; progression of the invasion in the colonic mucosa usually leads the the formation of typical flask ulcers. In some cases ulcerations may extend to the submucosa causing microhaemorrhages and sometimes to the muscle layers and serosa leading perforation E. histolytica trophozoites within necrotic tissue

79
E.histolytica colitis: the usual presentation of the disease is the amebic dysentery. Sigmoidoscopy may show typical ulcers.

81
A. B. A. G.intestinalis cyst: cysts are oval, 8-14 x 5-10 µm, with four nuclei and fibrils and flagella longitudinally oriented. B. Giardia intestinalis: 1 cyst containing 4 nuclei, rest of flagella and sucking disc. Stained fecal film. Wheatley modification of Gomori‘s trichrome technique. Objective 100 X

82
Giardia intestinalis: trophozoites from diarrhoeal stools
Giardia intestinalis: trophozoites from diarrhoeal stools. Usually 12 X µm in size. Stained fecal film. Wheatley modification of Gomori‘s trichrome technique. Objective 100 X

83
G. intestinalis trophozoites in a jejunal section
G. intestinalis trophozoites in a jejunal section. Several sickle-like profiles are seen over the epithelium (H&E X400). Autopsy of a 6-years-old undernourished boy.
. Autopsy of a 6-years-old undernourished boy.")
84
Giardia intestinalis: trophozoite of Giardia intestinalis WB strain stained with Giemsa

85
G.intestinalis : trophozoites live upon the surface of the villi of the small intestine. A trophozoite attached to the columnar cells of the intestine.

87
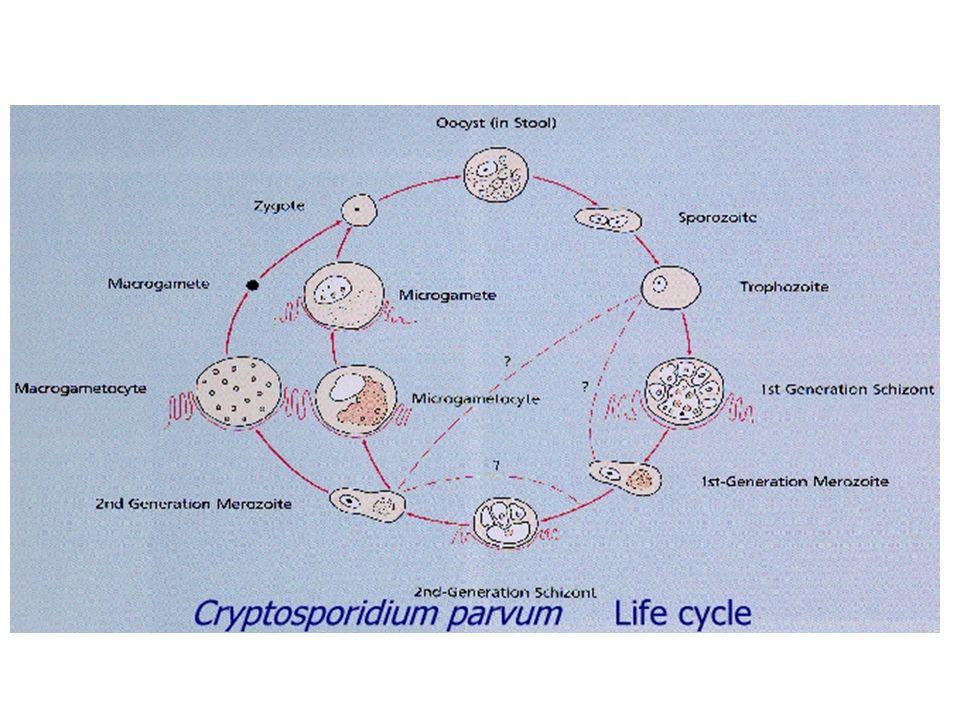
C.parvum oocysts: diagnosis is based on identification of oocysts with specific
stains as modified acid fast stain. Oocysts appear as bright pink to red organisms containing some dark granules and usually have a central clear area. (Mod. acid fast stain)
")
88
C.parvum oocysts (wet mount)
")
89
C.parvum, duodenal biopsy: histologic changes are not characteristic:
blunting or loss of villi, elongation of crypts, infiltration of the lamina propria are described. (H&E stain)
")
90
C.parvum, Electron micrograph: a trophozoite (2-2,5 µm in diameter)
attached to epithelial cells

91
C.parvum, Electron micrograph: meront type I (4-5 µm in diameter) attached
to an epithelial cell. Type I meront contains 8 merozoites

92
BLOOD, BONE MARROW SPLEEN PARASITES

95
Plasmodium sp.: the genus Anopheles includes more than 400 species of mosquitoes. Many may act as vectors of human diseases such as malaria, filariasis and some arbovirus. Eggs present a pair of lateral floats and are laid singly on the water surface, while larvae lay in a horizontal position under the water surface.

96
Plasmodium sp.: the resting position of the adult Anopheles is characteristic with the proboscid, head and abdomen in a straight line at an angle of about 45° with the surface on which they rest.

97
P. falciparum: species identification is possible on the basis of the appearance of parasites
of each of the four malaria species. Shape and size of asexual parasites and of macro- and microgametocytes, developmental stages in peripheral blood, modifications of infected erythrocytes, presence of dots or clefts on the red blood cells are the main differential characteristics.

98
P.falciparum trophozoites, thick smear, Giemsa stain.

99
P. falciparum: trophozoites are small rings with single or double small chromatin dots, and regular cytoplasm; multiple infection and high parasitemia (>5%) are common. Dots or cleft (Maurer's) can be observed on the infected RBCs. P.falciparum trophozoites, thin smear, Giemsa stain.
 are common. Dots or cleft (Maurer s) can be observed on the infected RBCs. P.falciparum trophozoites, thin smear, Giemsa stain..")
100
P. falciparum: sometimes trophozoites appear at the edge of the red blood cell (applique form), left. Erythrocytes maintain regular shape and size. P.falciparum trophozoites, thin smear, Giemsa stain right.
, left. Erythrocytes maintain regular shape and size. P.falciparum trophozoites, thin smear, Giemsa stain right..")
101
P. falciparum: late trophozoites and schizonts usually are not observed in peripheral blood unless in severe infections. P.falciparum, thin smear, Giemsa stain.

102
P.falciparum: micro- and macrogametocytes are easily recognized by their crescentic, cigar- or banana-like shape. Microgametocytes have a diffuse chromatin, while macrogametocytes have thickened chromatin. Microgametocyte, Giemsa thin smear.

103
P.falciparum: staining with fluorochromes is rapid (less than 1 min) and observation of slides can be performed at low magnification (400X) allowing rapid screening of smears even with low parasitemia. P.falciparum (DAPI-PI).
..")
104
P.falciparum: rosetting of infected and uninfected red blood cells and cytoadherence of parasitized erythrocytes to the vascular endothelium, play a crucial role in sequestration of parasites and obstruction of brain vessels. Induction of host cytokines and soluble mediators such as oxygen radicals and NO play an important role in the pathogenesis of the infection.

105
P.falciparum: the brain appears oedematous, hyperaemic and with pigment deposition; the capillaries, expecially of the white matter, appear dilated and congested and obstructed by parasitized RBCs.

106
P.falciparum: renal failure may result from sequestration of RBCs and alteration of the renal microcirculation. Glomerulal and interstitial vessels present RBCs adhering to the endothelium.

107
P.falciparum: sequestration and cytoadherence of parasitized RBCs in heart microcirculation is frequent but myocardial dysfunctions and cardiac arrhythmias are uncommon in severe falciparum malaria.

108
P.falciparum: jaundice and abnormalities of liver function tests are frequent
findings in severe falciparum malaria but hepatic failure is rare even in heavily infected individuals. P.falciparum: histological abnormalities include Kuppfer hyperplasia, mononuclear hyperplasia and sinusoid dilatation; swollen hepatocytes contain haemosiderin. Kuppfer cells contain a lot of malaria pigment.

109
A fatal case of P.falciparum malaria (liver): malarial pigment within Kupffer cells (H&E X 400)
: malarial pigment within Kupffer cells (H&E X 400)")
110
A fatal case of P.falciparum malaria (liver): note a parasitized erytrocyte (H&E X1000)
: note a parasitized erytrocyte (H&E X1000)")
111
P. malariae: trophozoites are usually small rings with a single dot of chromatin or have a compact, regular cytoplasm that seems to contain the nucleus. The pigment in late trophozoites is scattered. (Thin smear, Giemsa).
..")
112
P. malariae: trophozoites may assume a band form typical of the species. Red blood cells are not enlarged or rather smaller than normal. Multiple infection is rare. The parasitemia is usually low. No dots or clefts. (Thin smear, Giemsa).
.")
113
A C B P.malariae: schizonts are small and with a low number of merozoites (<12) arranged in regular forms (rosettes) with a thickened, often central, pigment. The complete erythrocytic cycle takes 72 hours and ends with the releasing of free merozoites (c). (Thin smear, Giemsa).
 arranged in regular forms (rosettes) with a thickened, often central, pigment. The complete erythrocytic cycle takes 72 hours and ends with the releasing of free merozoites (c). (Thin smear, Giemsa).")
114
A. B. A. Plasmodium ovale: trophozoite
B. P.ovale: all stages are seen in blood films; prominent Shuffner's dots are present at all stages. Trophozoites appear as rings with, usually, a compact cytoplasm; they do not have ameboid cytoplasm. A. B.

115
P.ovale: red blood cells are enlarged, ovalized and distorted with fimbriae
at poles. Schizonts have usually 8-10 merozoites.

116
P.vivax: the trophozoites increases in size and the cytoplasm becomes ameboid with rapid movements ("vivax"). The red blood cell enlarges and prominet Shuffner's dots are present. (Thin smear, Giemsa).
..")
117
P.vivax: in more advanced stage of development trophozoites occupy most of the RBC, and have a large vacuole and fine rods of pigment. The nucleus increases in size.

118
P.vivax: late trophozoites have a more dense cytoplasm, and a large vacuole.

119
P.vivax: in young schizonts the nucleus divides and the vacuole disappears; the cytoplasm is dense.

120
P. vivax: in about 48hours schizogony is completed
P.vivax: in about 48hours schizogony is completed. Mature schizont may contain merozoites. In thick smears schizonts look smaller than in thin smears and the Schuffner's dots are not always visible.

121
P.vivax: gametocytes are round or oval without vacuole; most of the RBC is occupied by the parasite. Macrogametocytes have a compact chromatin mass while microgametocytes have a more diffuse nucleus stained pink.

122
P.vivax: staining with fluorochromes is rapid (less than 1 min) and observation of slides can be performed at low magnification (400X) allowing rapid screening of smears even with low parasitemia. P. vivax (DAPI-PI).
..")
124
T. gondii: T.gondii encephalitis (TE) is the most common cerebral opportunistic infection in patients with AIDS. The typical lesion is an ipodense focal area with ring contrast-enhancement and edema. (CT scan of a toxoplasmic encephalitis).
 is the most common cerebral opportunistic infection in patients with AIDS. The typical lesion is an ipodense focal area with ring contrast-enhancement and edema. (CT scan of a toxoplasmic encephalitis)..")
125
T. gondii: tissue cysts, 100-300 µm, may contain up to 3
T. gondii: tissue cysts, µm, may contain up to bradyzoites. The wall of mature pseudocysts is believed to represent a combination of host and parasitic components.

126
T. gondii: direct detection of T
T. gondii: direct detection of T.gondii in clinical specimens is rare; parasites can be isolated from blood, CSF, amniotic fluid, tissue biopsies on cell lines (THP-1 or MRC-5). In clinical specimens the presence of parasites can also be demonstrated by PCR analysis.
. In clinical specimens the presence of parasites can also be demonstrated by PCR analysis.")
127
T. gondii: intracellular trophozoites of T. gondii in a cell culture
T. gondii: intracellular trophozoites of T.gondii in a cell culture. The trophozoites proliferate within the vacuole developing a pseudocyst. (Trophozoites in a THP-1 cell, Giemsa stain).
.")
128
T. gondii: in cell cultures T
T. gondii: in cell cultures T.gondii proliferates to form a pseudocyst of 8-20 parasites. (Trophozoites in a THP-1 cell, Giemsa stain).
.")
129
T. gondii: lysis of a THP-1 cell with release of tachizoites in culture. (Trophozoites in a THP-1 cell, Giemsa stain).
..")
130
T. gondii: : intracellular trophozoites of T
T. gondii: : intracellular trophozoites of T.gondii in a cell culture of human fibroblasts (MRC-5). The parasite was isolated from amniotic fluid.
. The parasite was isolated from amniotic fluid.")
131
T. gondii: microscopical features of tachizoites of Toxoplasma gondii and peritoneal macrophages of mouse in peritoneal exudate. (SEM)
.")
132
T. gondii: microscopical features of tachizoites of Toxoplasma gondii and peritoneal macrophages of mouse in peritoneal exudate. (SEM)
.")
133
T. gondii: cross-section through an endozoid in an advanced stage of endodiogeny. The daugther cells appear to be surrounded. In each of these news cells there are two round bodies that lengthen forming the first rhoptries.

134
T. gambiense and rhodesiense: about 20
T. gambiense and rhodesiense: about cases occur annually in the endemic areas. A. The African trypanosomiasis is transmitted by several species of tse-tse flies (Glossina spp.). B. Larva and pupae of Glossina morsitans C. Adult Glossina tachinoides in West Africa A. B. C.
. B. Larva and pupae of Glossina morsitans C. Adult Glossina tachinoides in West Africa. A. B. C.")
135
T. gambiense and rhodesiense: two forms of trypomastigote can be seen in peripheral blood: one is long slender, 30 µm in lenght, and is capable of multiplying in the host, the other is stumpy, not dividing, 18 µm in lenght.

136
Trypanosoma brucei gambiense and rhodesiense: the terminal stage of the infection ("sleeping sickness") is the result of a chronic meningoencephalomyelitis. (H&E stain).
..")
139
The infection is transmitted by various species of Phlebotomus, the sand fly.

140
Visceral leishmaniasis (Kala-azar) is caused by parasites of the genus Leishmania, subgenus Leishmania, complex donovani (donovani, infantum, chagasi species). Viscerotropic strains of L.infantum and L.tropica have been described. (bone marrow aspirate)
.")
141
L.major: confocal fluorescent microscopy of the GFP gene.

142
Leishamnia sp. : Leishmania promastigotes measure 15-20 by 1. 3-3
Leishamnia sp.: Leishmania promastigotes measure by µm and have a single flagellum, measuring µm.

143
GENITO-URINARY PARASITES

144
S. haematobium: intermediate host of S
S.haematobium: intermediate host of S.haematobium are snails of the genus Bulinus.

145
Schistosoma haematobium: the diagnosis of urinary schistosomiasis requires the
identification of eggs in urinary sediment. Eggs measure by µm and have a terminal spine; viable eggs contain a motile miracidium. (Urine sediment)
")
146
Schistosoma haematobium: the diagnosis of urinary schistosomiasis requires the
identification of eggs in urinary sediment. Eggs measure by µm and have a terminal spine; viable eggs contain a motile miracidium. (Urine sediment)
")
147
S.haematobium: Young men (35J) from Egypt with infertility and hematuria. Schistosoma haematobium eggs are concentrated in the tissue of the bladder. 4x magnification

148
S.haematobium: Young men (35J) from Egypt with infertility and hematuria. Schistosoma haematobium eggs are concentrated in the tissue of the bladder. 40xmagnification

149
Schistosoma haematobium: urine sediment, miracidium hatching from the egg (400 X).
.")
150
Trichomonas vaginalis: trophozoites live in vaginal cavity and urethra, where they multiply when the vaginal condition is favourable (at pH 4). Reproduction is by longitudinal fission. (Trophozoite, fresh examination).
..")
151
Trichomonas vaginalis: these flagellates are 10-30 µm in lenght and 6-20 µm in breadth.
Flagella, nucleus, axostyle and undullating membrane are visible. Filamentous form of Lactobacillus Döderleini is present. Acute trichomoniasis. Vaginal smear, Giemsa-Romanowski stain. Objective 100 X

152
Trichomonas vaginalis: Vaginal fluid; May Grunwald-Giemsa stain

153
PARASITES OF THE LIVER, LUNG AND CENTRAL NERVOUS SYSTEM

155
Echinococcus granulosus: the cysts (2 to 30 cm) are constituted by an external acellular cuticule and an inner cellular "germinal" layer (10-25 µ) that produces the brood capsules containing 6-12 protoscolices or single protoscolices. (Germinal layer with a protoscolex).
..")
156
Echinococcus granulosus: the larvae (scolices) develop from the germinal layer. The protoscolices are at first evaginated and measure by µ.

157
Echinococcus granulosus: the mature protoscolices have 4 suckers and a rostellum with hooklets and can be observed in the hydatid fluid.

158
Echinococcus granulosus: detail of the rostellum.

159
Echinococcus granulosus: the presence of isolated hooklets is diagnostic for hydatidosis. Hooklets can be observed in hydatid fluid and must be searched in sputum after a vomica .

160
Echinococcus granulosus: the protoscolices then become invaginated and measure 90-140 by 70-120 µm.

161
Echinococcus granulosus: the liver is the most common site of development of cysts (50-75%). Lesions can be detected by CT scan or echography; a septate structure is a characteristic of active cysts. Treatment is based on surgical and/or medical therapy (albendazole)
.")
162
Echinococcus granulosus: pulmonary infection is observed in about 20-30% of patients. Roengtenografic examination shows round mass lesions and CT scan demonstrates the fluid content of the lesion. Serology has a lower sensitivity in extrahepatic hydatidosis.

163
Acanthamoeba spp.: free living amoebae of the Acanthamoeba genus cause two clinical syndrome: 1) Granulomatous amoebic encephalitis (GAE) 2) Subacute and chronic amoebic keratitis A disseminated form of GAE is described in individuals with the Acquired Immunodeficiency Syndrome (AIDS) Several species of Acanthamoeba have been identified: A.castellani, A.culberstoni, A.polyphaga, A.zhysodes, A.hatchetti, A.astronyxis, A.palestinensis. (Trophozoites, trichrome stain).
..")
164
Acanthamoeba spp.: the cysts are spherical, µm in diameter, having a thick double wall. The outer wall may be spherical or wrinkled, the inner wall appear stellate or polyhedral. (Acanthamoeba trophozoites and a cyst, trichrome stain).
..")
165
Acanthamoeba spp.: trophozoite as seen under phase contrast microscope. Its big nucleolus, both lobopodia and acanthopodia and various vacuoles can be seen clearly.

166
Acanthamoeba spp.: cysts stained with Heidenhain’s iron alum-haematoxylin method.

167
N. gruberi: trophozoite as seen under phase contrast microscope
N. gruberi: trophozoite as seen under phase contrast microscope. Its big nucelolus, four lobopod type pseudopodia and the contractile vacuole can be clearly seen.

168
Naegleria spp.: trophozoite stained with Greenstein’s five dye stain and observed under dark field microscope.

Similar presentations

















>")
 Drs. Babcock and Hopkins Spring 2009>")

>")














