Download presentation
Presentation is loading. Please wait.

1
Apixaban in Patients with Atrial Fibrillation
AVERROES

2
Apixaban in Patients with Atrial Fibrillation
NEJM 10TH FEBRUARY 2011

3
Study at 522 centers in 36 countries
Study at 522 centers in 36 countries. Enrollment began on September 10, 2007, and was completed on December 23, Sponsored by Bristol-Myers Squibb and Pfizer. Double blind placebo trial

4
50 yearsof age or older and
Inclusion Criteria 50 yearsof age or older and Atrial fibrillation documented in the 6 months before enrollment or by 12- lead electrocardiography on the day of screening.

5
Plus 1 of these risk factors for stroke:
prior stroke or transient ischemic attack, age of 75 years or older, arterial hypertension (receiving treatment), diabetes mellitus (receiving treatment), heart failure (NYHA 2 or higher at the time of enrollment), LVEF of 35% or less, documented peripheral-artery disease.
, diabetes mellitus (receiving treatment), heart failure (NYHA 2 or higher at the time of enrollment), LVEF of 35% or less, documented peripheral-artery disease.")
6
Exclusion Criteria Vitamin K antagonist therapy
Other conditions other than AF requiring anticoagulation valvular disease requiring surgery, a serious bleeding event in the previous 6 months or a high risk of bleeding (e.g., active peptic ulcer disease, a platelets <100 or hemoglobin level of <10, stroke within the previous 10 days, Documented hemorrhagic tendencies, or blood dyscrasias)
")
7
current alcohol or drug abuse
Psychosocial issues, life expectancy of less than 1 year, Severe CKD (a serum creatinine level of >221 or creat clearance of <25) ALT or AST level greater than 2 times the upper limit of the normal range Total bilirubin more than 1.5 times the upper limit of the normal range, and allergy to aspirin.
 ALT or AST level greater than 2 times the upper limit of the normal range. Total bilirubin more than 1.5 times the upper limit of the normal range, and allergy to aspirin.")
8
Patients were randomly assigned to receive apixaban at a dose of 5 mg twice daily or aspirin at a dose of 81 to 324 mg per day. Randomization was performed with the use of a 24-hour central, computerized, automated voice-response system. In keeping with the double-dummy design.

9
A reduced dose of apixaban (2
A reduced dose of apixaban (2.5 mg twice daily) was used throughout the study for patients who met two of the following criteria: an age of 80 years or older, a body weight of 60 kg or less, or a serum creatinine level of 133 or higher
 was used throughout the study for patients who met two of the following criteria: an age of 80 years or older, a body weight of 60 kg or less, or a serum creatinine level of 133 or higher.")
10
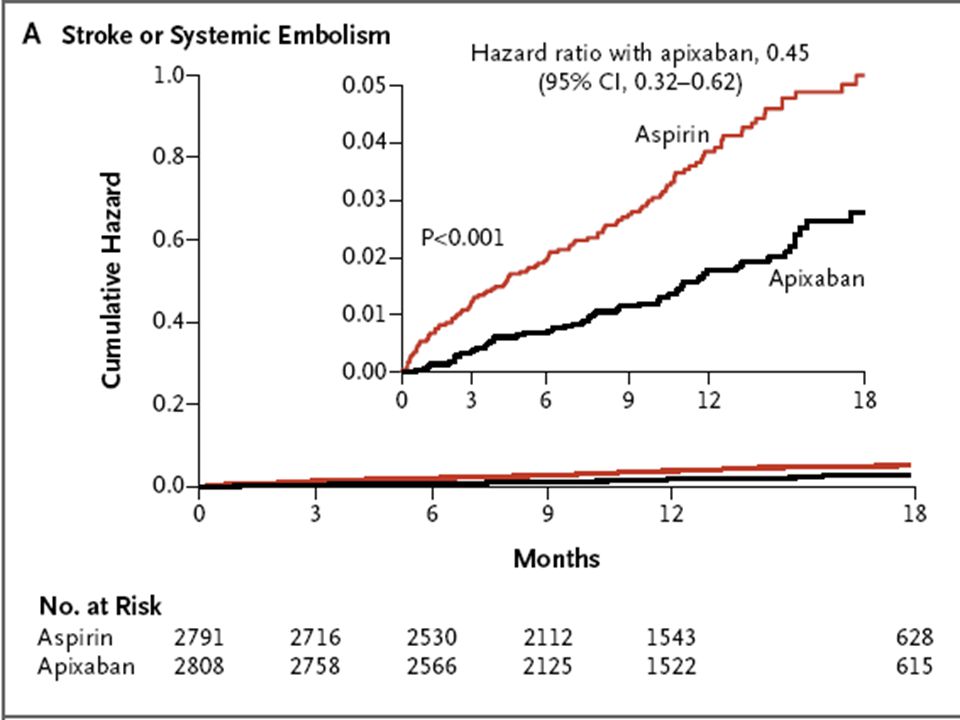
Primary efficacy outcome
Stroke or systemic embolization Primary safety outcome Major bleeds

11
Secondary outcomes MI Death from vascular cause Death from any cause
Composites of major vascular events

12
Results 5999 patients 37% from Northern America or Western Europe

13
Variable Apixaban Aspirin (N = 2808) (N = 2791) Age — yr 70±9 70±10 Heart rate — beats/min 74±14 74±14 Systolic blood pressure 132±16 132±16 Body-mass index† 28±5 28±5 Male sex — no. (%) 1660 (59) 1617 (58) Baseline ECG findings — no. (%) Atrial fibrillation 1923 (68) 1894 (68) Atrial flutter 19 (1) 20 (1) Sinus rhythm 707 (25) 730 (26) Paced or other rhythm 147 (5) 139 (5) LVH 490 (17) 498 (18)
 1660 (59) 1617 (58) Baseline ECG findings — no. (%) Atrial fibrillation 1923 (68) 1894 (68) Atrial flutter 19 (1) 20 (1) Sinus rhythm 707 (25) 730 (26) Paced or other rhythm 147 (5) 139 (5) LVH 490 (17) 498 (18) .")
14
Risk factors for stroke — no
Risk factors for stroke — no. (%) Prior stroke or TIA 390 (14) 374 (13) HTN, on treatment 2408 (86) 2429 (87) Heart failure 1118 (40) 1053 (38) NYHA class 1 or (33) 878 (31) NYHA class 3 or (7) 175 (6) LV EF ≤35% 144 (5) 144 (5) Peripheral-artery disease 66 (2) 87 (3) Diabetes, on treatment 537 (19) 559 (20) Mitral stenosis 64 (2) 50 (2)
 Prior stroke or TIA 390 (14) 374 (13) HTN, on treatment 2408 (86) 2429 (87) Heart failure 1118 (40) 1053 (38) NYHA class 1 or (33) 878 (31) NYHA class 3 or (7) 175 (6) LV EF ≤35% 144 (5) 144 (5) Peripheral-artery disease 66 (2) 87 (3) Diabetes, on treatment 537 (19) 559 (20) Mitral stenosis 64 (2) 50 (2)")
15
Classification of atrial fibrillation — no
Classification of atrial fibrillation — no. (%) Paroxysmal 760 (27) 752 (27) Persistent 587 (21) 590 (21) Permanent 1460 (52) 1448 (52) CHADS2‡ Mean score 2.0± ±1.1 Score — no. (%) 0 or (36) 1022 (37) (37) 954 (34) ≥3 758 (27) 812 (29) High-school education or more — no. (%) 1635 (58) 1635 (59) Use of vitamin K antagonist within 30 days before screening 401 (14) 426 (15) Use of aspirin within 30 days before screening 2137 (76) 2081 (75)
 Paroxysmal 760 (27) 752 (27) Persistent 587 (21) 590 (21) Permanent 1460 (52) 1448 (52) CHADS2‡ Mean score 2.0± ±1.1 Score — no. (%) 0 or (36) 1022 (37) (37) 954 (34) ≥3 758 (27) 812 (29) High-school education or more — no. (%) 1635 (58) 1635 (59) Use of vitamin K antagonist within 30 days before screening 401 (14) 426 (15) Use of aspirin within 30 days before screening 2137 (76) 2081 (75)")
16
Medication use at baseline — no
Medication use at baseline — no. (%) ACE inhibitor or ARB 1790 (64) 1786 (64) Verapamil or diltiazem 251 (9) 248 (9) Beta-blocker 1563 (56) 1534 (55) Digoxin 821 (29) 754 (27) Amiodarone 298 (11) 328 (12) Statin 883 (31) 879 (31)
 ACE inhibitor or ARB 1790 (64) 1786 (64) Verapamil or diltiazem 251 (9) 248 (9) Beta-blocker 1563 (56) 1534 (55) Digoxin 821 (29) 754 (27) Amiodarone 298 (11) 328 (12) Statin 883 (31) 879 (31)")
17
Region — no. (%) North America 408 (15) 396 (14) Latin America 589 (21) 596 (21) Western Europe 625 (22) 633 (23) Eastern Europe 639 (23) 611 (22) Asia and South Africa 547 (19) 555 (20) Study dose of aspirin or aspirin-placebo — no. (%) 81 mg 1816 (65) 1786 (64) 162 mg 718 (26) 750 (27) 243 mg 73 (3) 60 (2) 324 mg 193 (7) 184 (7) Data not available 7 (<1) 11 (<1) Study dose of 2.5 mg twice daily of apixaban or apixaban-placebo 179 (6) 182 (7)
 North America 408 (15) 396 (14) Latin America 589 (21) 596 (21) Western Europe 625 (22) 633 (23) Eastern Europe 639 (23) 611 (22) Asia and South Africa 547 (19) 555 (20) Study dose of aspirin or aspirin-placebo — no. (%) 81 mg 1816 (65) 1786 (64) 162 mg 718 (26) 750 (27) 243 mg 73 (3) 60 (2) 324 mg 193 (7) 184 (7) Data not available 7 (<1) 11 (<1) Study dose of 2.5 mg twice daily of apixaban or apixaban-placebo 179 (6) 182 (7) .")
18
outcomes Outcome Apixaban Aspirin P Value (N = 2808) (N = 2791) %/yr %/yr Stroke or systemic embolism <0.001 Stroke, systemic embolism, or death <0.001 Stroke, systemic embolism, myocardial infarction or death from vascular cause <0.001 Stroke, systemic embolism, myocardial infarction, death from vascular cause, or major bleeding Event
 (N = 2791) %/yr %/yr Stroke or systemic embolism <0.001 Stroke, systemic embolism, or death <0.001 Stroke, systemic embolism, myocardial infarction or death from vascular cause <0.001 Stroke, systemic embolism, myocardial infarction, death from vascular cause, or major bleeding Event")
19
Systemic embolism 0. 1 0. 4 0. 01 Myocardial infarction 0. 8 0. 9 0
Systemic embolism Myocardial infarction Death From any cause From vascular cause Hospitalization for cardiovascular cause <0.001

20
Bleeding event %/yr %/yr p-value Major 1. 4 1. 2 0. 57 Intracranial 0
Bleeding event %/yr %/yr p-value Major Intracranial Subdural‡ — Other intracranial, excluding hemorrhagic stroke and subdural‡ < — Extracranial or unclassified Gastrointestinal Non-gastrointestinal Fatal§

22
Limitations Study terminated early due to 1st interim analysis showed treatment benefit in favour of apixaban greater than 4 sd Theoretically could inflate the estimated benefit, however boundary had to be exceeded on 2 formal reviews.

23
Futher Studies… To look at comparison of Apixaban to Warfarin therapy in reducing stroke and adverse effects. (ARISTOTLE)
")
24
Summary In summary, among patients with atrial fibrillation who are at high risk for stroke and for whom vitamin K antagonist therapy is unsuitable: apixaban, as compared with aspirin, substantially reduced the risk of stroke, with no significant increase in the risk of major bleeding or intracranial bleeding. The net clinical benefit of apixaban in these patients was therefore substantial.

Similar presentations














>")




