Download presentation
Presentation is loading. Please wait.

1
Abdominal Pain – Approach to Pain Management in the Palliative Care setting Dr Pam Cupples RHSC, Glasgow APPM November 2012

3
Case Study 1 12 year old girl diagnosed with type 1 Neurofibromatosis Complex retroperitoneal neurofibroma arising early in childhood, which was not fully resectable Age 11 the mass became symptomatic Significant abdominal pain & distension Protracted vomiting & weight loss Rx chemotherapy and radiotherapy and further surgery to partially resect the tumour – pathology showed localised malignant transformation With tumour progression and metastases

4
Case Study 1 5 months after surgery she presented with intractable vomiting & colicky abdominal pain due to malignant bowel obstruction Child averse to NG placement So not passed until day 4 > 1L of bilious gastric content Vomiting 15 times / day How would you manage the patients symtoms? Coronal view of CT abdomen and pelvis revealing large left-sided retroperitoneal round tumor causing obstruction, with marked dilatation of proximal first portion of duodedum and stomach.

5
Management Plan Symptom control Analgesia in the hospital setting & at home Antiemetics Decompression of bowel Any alternative Rx to consider

6
Octreotide Synthetic analogue of somatostatin – GH releasing inhibiting factor Inhibition of endocrine & exocrine secretions Inhibits gastrin, secretin, VIP, insulin, glucagon, cholecystokinin, pancreatic peptide Decreases splanchnic flow Inhibits secretion of Cl into the jejunum, which increase water reabsorption Decreased secretion of water and electrolytes, inhibits pancreatic secretions, increased absorption of of water and electrolytes

8
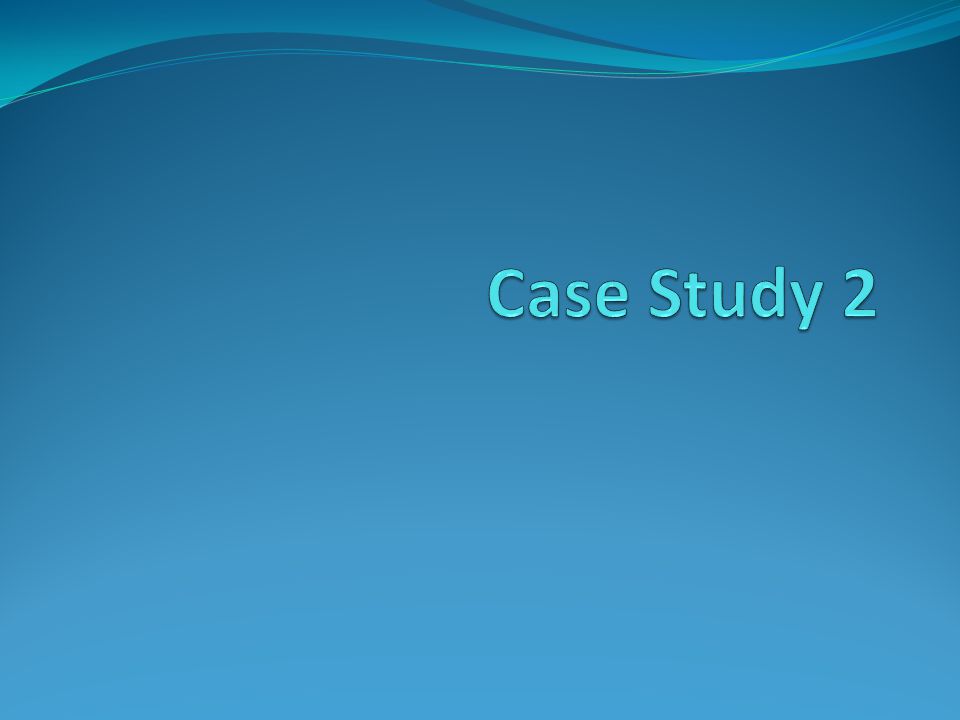
Case Study 2 3 year old boy with diagnosis of left sided Wilms Tumour Presents with palpable mass and constant abdominal pain Following Rx and surgical resection Complaining of sharp stabbing pain in scar and generalised upper abdominal pain, which has been present for > 3 months Not responsive to standard analgesics How would you manage this patient particularly with regards to his non opioid responsive abdominal pain Computed tomography scan of a large left Wilms' tumor with a small rim of functioning renal parenchym

9
Classification of Abdominal Pain Somatic Abdominal Pain Stimulation of the parietal peritoneum Accurate localisation sharp Visceral Pain Diffuse nature experienced of large area of the abdomen Associated with nausea and autonomic symptoms Few pain receptors Receptors in the walls of hollow viscera are very sensitive to distension Colicky type pain Perceived site of visceral pain relates to the embryological origin

10
Chronic Visceral Pain Heightened perception of GI sensation – visceral hyperalgesia Noxious stimuli – peripheral release of inflammatory mediators Activation and peripheral sensitisation of nociceptive afferents Reduced firing thresholds Expression & recruitment of previously silent nociceptors Transient receptor potential vallinoid 1 – TRPV1 Protease activated receptors – PAR Opioid agonists – limited by central action and side effects Voltage Gated Sodium Channels – VGSC – Nav 1.3-1.9 Central sensitisation – NMDA & PGE2 New Rx in the future – NMDA & PGE2 antagonists, serine protease inhibitors, TRPV1 antagonists

11
Rx Options to be considered TSE or TENS Oral Neuropathic medication Gabapentin Lamotrigine Regional techniques Epidural with ketamine

12
TENs Frequency dependent analgesia A (50-200Hz) A (2- 4Hz) Tingling sensation may be a problem TSE
 A (2- 4Hz) Tingling sensation may be a problem TSE")
13
Transcutaneous Spinal Electroanalgesia - TSE 1991 Biphasic waveform Ultrashort duration 4 sec

14
Chronic Neuropathic Pain Somatic Pain Gabapentin Blocks the voltage gated Ca > 50kg - max. dose up to 2400mg / 24hrs 35-50kg – max. dose up to 1600mg / 24hrs 25-35kg – max. dose up to 1200mg / 24hrs < 25kg – not recommended Visceral Pain Lamotrigine Blocks the Na channels > 50kg – start 10mg twice daily up to max. of 40mg b.d. 30-50kg – 5mg b.d up to max of 25mg <30kg – not recommended

15
Neural Modulation by Regional Blocks Epidural blocks Peripheral Nerve blocks Sympathetic Block Spinal Stimulation Act by blocking Na channels and preventing propagation of the AP

16
NMDA Antagonists Ketamine Binds to the phencyclidine site of the NMDA receptor and blocks IV– 15mg/kg/24 hours Diluted in normal saline to give a dose volume if 2- 4mls/hour Can increase to 25mg/kg/24hrs Epidural - 0.6mg/kg as a bolus and then infuse at 0.8 to 1mg/kg/24hours

18
Case No. 3 2 yearl old boy presents with intrahepatic mass Diagnosed with Hepatoblastoma Rx to date Chemotherapy Surgical resection Sharp constant upper quadrant pain Pain has improved with opioids but problems with opioid induced side effects What interventions could help control the abdominal pain in this setting?

19
Interventional Management opioid resistant pain Coeliac Plexus block Used for intractable pain due to upper abdominal malignancies

20
Intrathecal Drug Delivery & Epidurals Intrathecal infusion of LA, morphine, fentanyl, clonidine, Whyte E & Lauder G Paediatric Anaesthesia 2011

22
Case 4 8 year old Dx with metastatic stage IV neuroblastoma MYCN amplified Rx Chemotherapy, Peripheral stem cell harvest Laparotomy & resection of tumour High dose chemotherapy CEM and stem cell transplant Radiotherapy Enrolled in Immunotherapy trial Associated with several visceral pain during infusions

23
Case Study 4 - MRI

24
Cont. Despite Rx tumour progressed Palliative chemoRx and radioRx Ongoing issues of abdominal pain and pain in legs

25
Case 4 What treatment options are there for managing her visceral pain particularly during her immunotherapy? How would you manage her abdominal pain during her palliative care?

26
Summary Majority of abdominal pain can be managed using the WHO ladder Alternative Rx to consider Management strategies for chronic visceral pain Gabapentin & lamotrigine Ketamine infusions alone or in combination with opioids Epidural ketamine Intrathecal infusions Neuromodulation using Epidurals +/- ketamine Coeliac plexus blocks

27
Any Questions? ANY QUESTIONS?

28
Pharmacological Treatment Anticonvulsants Gabapentin Pregabalin Lamotrigine Carbamazepine Phenytoin Topiramate Levetiracetam Antidepressants 2°amines nortriptylline, desipramine 3°amines amitriptylline, imipramine, dothiepin Selective Serotonin Reuptake inhibitors fluoxetine,sertraline, citalopram 3rd Generation antidepressants venlafaxine

29
Treatment Options & Aims MANAGEMENT STRATEGY K.I.S.S. Non pharmacological – TENs, TSE, acupuncture Physiotherapy Pharmacological Regional techniques Psychological therapies & Pain Management Programmes GOALS Reduce Pain Improve function Develop coping strategies

30
Chronology of pain Constant pain – parietal inflammation or capsule distension Colicky pain - obstruction of viscera with peristaltic activity tend to be colicky Small & large bowel – colic over seconds or minutes Renal / biliary colic – hours / days Aggravating & relieving factors

31
Chronic Visceral Pain Heightened perception of GI sensation – visceral hyperalgesia Noxious stimuli – peripheral release of inflammatory mediators Activation and peripheral sensitisation of nociceptive afferents Reduced firing thresholds Expression & recruitment of previously silent nociceptors Transient receptor potential vallinoid 1 – TRPV1 Protease activated receptors – PAR Opioid agonists – limited by central action and side effects Voltage Gated Sodium Channels – VGSC – Nav 1.3-1.9 Central sensitisation – NMDA & PGE2

32
Parental Opioids Infusions Preterm 5mcg/kh/h Term up to 8mcg/kg/hr 1-3months up to 10mcg/hr >3 months up to 20mcg/hr PCA – 1mg/kg in 50mls of 0.9% saline bolus = 1ml = 20mcg/kg with a max of 1mg 5min lockout +/- background of 4mcg/kg/hour

33
Parental Opioids Infusions Preterm 5mcg/kh/h Term up to 8mcg/kg/hr 1-3months up to 10mcg/hr >3 months up to 20mcg/hr PCA – 1mg/kg in 50mls of 0.9% saline bolus = 1ml = 20mcg/kg with a max of 1mg 5min lockout +/- background of 4mcg/kg/hour

34
OPIOIDS MORPHINE Oral Morphine200- 400mcg/kg 4 hourly Convert to single/ twice daily sustained release MST continus Single daily dose of MXL Morphine not tolerated consider oxycodone DIAMORPHINE More potent, more soluble Subcutaneous Infusion 20-100mcg/kg/hour Converting from oral morphine total daily dose of morphine /3

35
OPIOIDS OXYCODONE Opioid Naive 0.2mg/kg 4 hourly Previous exposure to opioids Conversion ratio for morphine to oxycodone 2:1 Ie half the daily morpine dose FENTANYL Less sedation & constipation 25mcg, 50mcg, 75mcg & 100mcg patches Continue morphine for up to 12 hours after starting patch Remember breakthrough oral morphine Therapeutic levels 6-12 hrs Takes 24-48 hours to assess results

36
NCA - Nurse Controlled Analgesia Age < 1month self ventilating Bolus of 5mcg/kg lockout of 30min No background Age 1-3months Bolus of 10mcg/kg lockout of 30mins – no background Age >3months Bolus of 20mcg with max of 1mg Lockout of 20min Background of 20mcg/kg/hr

Similar presentations
















 Robert C. Byrd Center for Rural Health Marshall University.>")




