Download presentation
Presentation is loading. Please wait.

1
Haematology Case based discussions
Dr Nnenna Osuji Dr Stella Appiah-Cubi Dr Stella Kotsiopoulou 21/05/2014

2
Objectives Focus on primary/secondary care interface
Discuss cases encountered and practical lessons Highlight diagnostic clues Encourage confidence around community care of chronic stable haematological malignancies Information gathering Sickle vaccinations USC referrals Marker analysis/immunophenotyping Serum free light chains

3
Quiz Name the current consultants.
How do you contact haematology for advice? Blood film suggests CLL. How are you going to refer this patient? Indications for 2WR Haematology Referrals

4
MALIGNANT HAEMATOLOGY
Monoclonal Protein MGUS Vs Multiple Myeloma Case Discussions CLL Case Discussion

5
Varies greatly with age.
What is an M protein? It is a monoclonal immunoglobulin secreted by an abnormally expanded clone of plasma cells that can be detected by immunofixation of serum and/or urine. Varies greatly with age. 1 - 2% of people in their 6th decade 2-4% in their 7th decade 4-5% in their eighth decade 14% over the age of 90 Racial variation Twice as common in black people as white people

7
Incidence of M-proteins
Varies greatly with age. 1 - 2% of people in their 6th decade 2-4% in their 7th decade 4-5% in their eighth decade 14% over the age of 90 Racial variation Twice as common in black people as white people

8
Monoclonal gammopathies occur in the following conditions
Haematological malignancies Multiple myeloma Solitary plasmacytoma (skeletal or extra- medullary) Waldenstrom's macroglobulinaemia Low grade non-Hodgkin’s lymphoma Monoclonal gammopathy of undetermined significance ( MGUS) AL amyloidosis Connective tissue disorders RA, SLE, scleroderma, polymyositis and ankylosing spondylitis. Skin disorders Infections Hepatitis C virus (HCV)-related chronic liver disease HIV Helicobacter pylori
 Waldenstrom s macroglobulinaemia. Low grade non-Hodgkin’s lymphoma. Monoclonal gammopathy of undetermined significance ( MGUS) AL amyloidosis. Connective tissue disorders. RA, SLE, scleroderma, polymyositis and ankylosing spondylitis. Skin disorders. Infections. Hepatitis C virus (HCV)-related chronic liver disease. HIV. Helicobacter pylori.")
10
Predicting Progression
There were only 2 statistically significant risk factors for progression The concentration of monoclonal protein The type of monoclonal protein IgA and IgM gammopathy more likely than IgG to progress IgM rarely becoming myeloma

11
Monitoring in the low risk group
Low risk defined as IgG M-protein <15g/l IgA or IgM M-protein <10g/l No symptoms/signs of myeloma, lymphoproliferative disorders or AL amyloidosis This group forms the vast majority of M proteins detected in routine practice

12
Acronym: CRAB

13
New International Staging System: ISS
Stage Criteria Median survival I Beta2 microglobulin<3.5 mg/L and Serum albumin >3.5 g/dl 62 mo. II Neither I or III 45 III Beta2 microglobulin >5.5 mg/L 29

14
Clinical presentation
Symptoms of bone disease, persistent unexplained backache Impaired renal function Anaemia Hypercalcaemia Recurrent or persistent bacterial infection Hyperviscosity Spinal cord/nerve root compression Symptoms suggestive of amyloidosis (nephrotic syndrome, cardiac failure) High ESR (incidental finding)
 High ESR (incidental finding)")
18
Case 1. - Patient G.R. 13/07/2005 67-year old Afro-Caribbean
Right hypochondrial pain Fatigue Recently treated for epistaxis

19
Patient G.R. FBC: Hb 6.6, WBC 5.0, plts 85 Urea 10.2, creatinine 128
Adj. Ca 4.38, albumin 28 ESR 138 mm/h

20
Patient G.R. Admit Anaemia due to 3 units of blood transfusion
? Malignancy ? Epistaxis 3 units of blood transfusion i.v. fluids + Pamidronate

21
Patient G.R IgA λ paraprotein 75 g/l (t.prot 127 g/l)
β2 microglobulin 5.6mg/l BM – plasma cells 40% INR 1.32, APTTr 1.34, fibrinogen 1.67 g

22
Patient G.R Drowsy Transfer to ITU Bleeding from mouth
HD Methylprednisolone Subsequent C-VAD, Z-Dex chemotherapy

23
EMERGENCY !!! Hyperviscosity
Treatment – plasmapheresis, HD steroids, iv hydration

24
Case 2. Patient B.B. 05/08/2005 49-year old Afro-Caribbean
Back pain - 9 mo. (6 mo. off work) Not able to mobilize from bed without help
 Not able to mobilize from bed without help.")
25
Patient B.B. FBC – clotted Urea 6.5, creatinine 150
Adj. Ca 2.68, albumin 19 Total protein 174 g/L Paraprotein 141 g/L IgGκ

26
Patient B.B. Hb 3.4 (citrate blood)
INR 1.5, APTTr 1.25, fibrinogen 1.41

27
Patient B.B. 3 sessions of plasmapheresis at RMH
Blood transfusion after plasmapheresis Z-Dex chemotherapy Abnormal ECHO CThal Dex chemotherapy

28
Case 3. Patient J.M. 01/08/2005 48-year old Afro-Caribbean
Sudden lower-back pain on sneezing 3 mo. prior to admission 5/7 history back pain and reduced power in left leg

29
Patient J.M. FBC: Hb 10.5, WBC 6.8, plts 278
Urea, creatinine, adj. Ca - N T. protein 99 paraprotein 45 g/L IgGκ

30
Patient J.M. 05/08/2005 Left leg – no movement
Right leg – reduced power

31
EMERGENCY !!! Spinal cord compression Treatment – radiotherapy, Dexamethasone

32
Patient J.M. 1st August – Lumbar spine X ray 2nd August – MRI
2nd August – CT- guided biopsy 4th August - diagnosis ?MM, ?NHL 4/5th August – referral to haematology 5th August - referral for radiotherapy 6th August - radiotherapy

33
Patient J.M. 20 Gy – 5 doses 1 course Z-Dex, 3 courses C-VAD
!! Able to take few steps with crutches Right leg – back to normal Left leg – much improvement

34
Case 4. Patient N.H. 12/08/2005 71-year old Caucasian 3/12 back pain
Spine X-ray – lytic lesion lumbar

35
Patient N.H. FBC: Hb 15.6, N 5.7, plts 237
Us&Es, Ca, t. protein – normal Small IgG paraprotein BM – 3% plasma cells CT-guided biopsy – plasma cells

36
Patient N.H. PLASMACYTOMA Treatment 40 Gy in 20 fractions

37
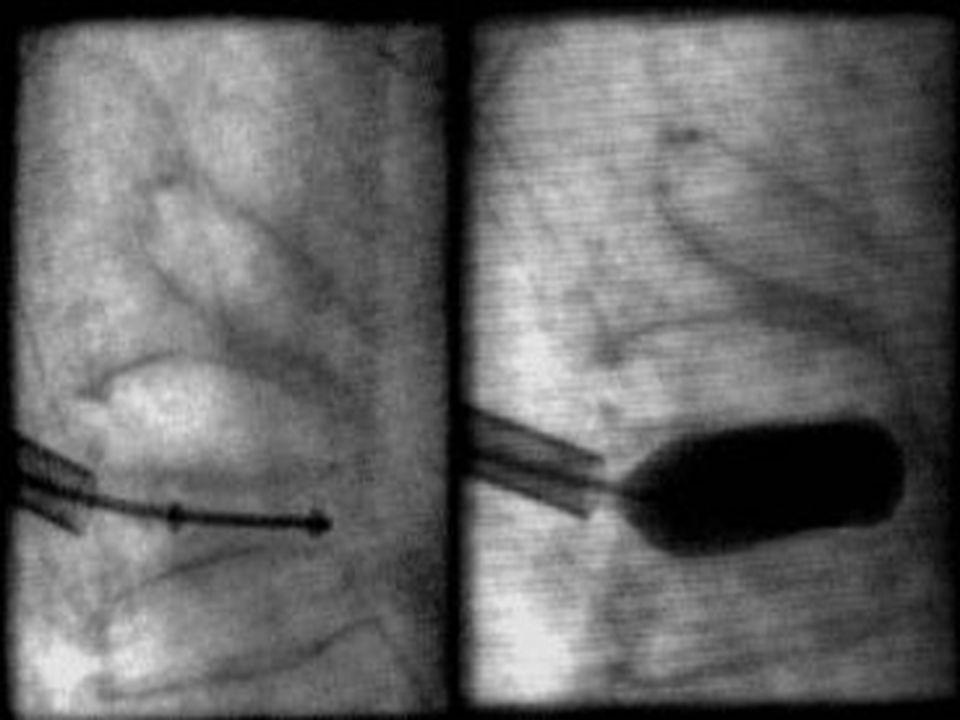
Management of persistent pain
SURGERY Contraindicated in the absence of structural instability Management of persistent pain Vertebroplasty – bone strengthening and pain relief but does not restore height (polymethacrylate) Kyphoplasty – vertebral height can be restored (small inflatable balloon)
 Kyphoplasty – vertebral height can be restored (small inflatable balloon)")
40
Chronic Lymphocytic Leukaemia CLL

41
CLL Clonal B cell malignancy.
Progressive accumulation of long lived mature lymphocytes Most common leukemia of Western world. Male to female ratio is 2:1. Median age at diagnosis is years. Small proportion are familial Aetiology unknown

42
Clinical features Mostly disease of elderly with Often asymptomatic.
Classic B symptoms recurrent infections Lymphadenopathy, hepatosplenomegaly. Marrow failure Autoimmune haemolytic anaemia/thrombocytopenia

43
Diagnosis Persistent lymphocytosis > 5 x 109/l.
Morphology Mature looking lymphocytes -clumped chromatin Immunophenotyping BM not required for diagnosis.

44
Immunophenotyping Majority score 4/5 Score < 3 not CLL

45
Staging- classification systems

46
CLL Complications Infection Autoimmune – ITP/Haemolytic anaemia
Bacterial – hypogammaglobulinaemi a Viral – T-cell dysfunction (H. Zoster) Autoimmune – ITP/Haemolytic anaemia Other malignancies Transformation Richter’s, Hodgkin’s Shingles High dose therapy 800mg 5 x per day for 10 days then prophylactic dose 400mg tds Neuropathic pain
 Autoimmune – ITP/Haemolytic anaemia. Other malignancies. Transformation. Richter’s, Hodgkin’s. Shingles. High dose therapy 800mg 5 x per day for 10 days then prophylactic dose 400mg tds. Neuropathic pain.")
47
CLL treatment Many watch and wait – stage A Chemotherapy
Bone marrow failure=stage progression B symptoms – weight loss, sweats, fevers (unexplained) Symptoms from enlarged lymph nodes/spleen Transformation Not for high WBC alone Median survival 10 years What? Chemotherapy FCR- fludarabine, cyclophosphamide, rituximab Chlorambucil - elderly Steroids Alemtuzumab – anti CD52
 Symptoms from enlarged lymph nodes/spleen. Transformation. Not for high WBC alone. Median survival 10 years. What Chemotherapy. FCR- fludarabine, cyclophosphamide, rituximab. Chlorambucil - elderly. Steroids. Alemtuzumab – anti CD52.")
48
“Watch and wait” policy
When to refer back B symptoms Lymphadenopathy Hepatosplenomegaly Falling haemoglobin, platelets, rapidly rising lymphocyte count Recurrent infections Autoimmune complications How often? Every 3 months Then reduce frequency if stable

49
Mrs ID 2004 Aged 80, Routine FBC- lymphs 8. Normal Hb/neutrophils/plats Well , no B symptoms, lymphadenopathy or hepatosplenomegaly Diagnosis CLL ‘Watch and wait ’ policy Discharged 2011 – GP to monitor

50
BENIGN HAEMATOLOGY Anaemias B12 Deficiency Case Discussion
Iron Deficiency Vs Thalassaemia Trait Elevated Ferritin

51
ANAEMIA Definition Categorized according to Red Cell indices MCV and MCH: Hypochromic and Microcytic (low indices) Normochromic and Normocytic (normal indices) Macrocytic (high MCV) Can you name one cause for each category?
 Macrocytic (high MCV) Can you name one cause for each category")
52
MACROCYTIC ANAEMIA How do we investigate?
1st line tests: B12, Folate, TSH, reticulocyte count, LDH, LFTs, blood film: ? Any dysplastic features. ? History of alcohol consumption 2nd line tests: SPE, UPE, DAT/haemolysis screen 3rd Line: Bone Marrow investigations

53
A guide to the management of B12 deficiency in the primary care

54
Outline Sources of dietary vitamin B12 Vitamin B12 absorption
Causes of B12 deficiency Indications for measuring B12 level Clinical presentation of B12 deficiency Investigations to help define the cause of B12 deficiency. A guide to management

55
Sources Foods of animal origin- meat, fish, eggs, milk, cheese but not in plants. Recommended daily requirement is 1- 2µg/day Total body stores of µg Mainly stored in the liver( up to 2yrs stores)
")
56
Absorption

57
Who is at Risk

58
Causes of B12 deficiency • Inadequate vitamin B12 in diet
▪ strict vegans • Vitamin B12 malabsorption ▪ Pernicious anaemia-loss of GP→IF↓( increased of CA stomach ~ 2-3%) ▪ Long term use of PPI or H2-antagonist ▪ Chronic alcoholism ▪ Coeliac disease ▪ Small bowel( esp. terminal ileal) surgery ▪ Generalised malabsorption e.g. Tropical sprue, IBD ▪ Blind loop syndrome +/- small bowel bacterial overgrowth ▪ Fish tapeworm •Drugs ▪ Biguanides e.g.. Metformin ▪ Oral contraceptive pill ▪ Slow K, Cholestyramine
 ▪ Long term use of PPI or H2-antagonist. ▪ Chronic alcoholism. ▪ Coeliac disease. ▪ Small bowel( esp. terminal ileal) surgery. ▪ Generalised malabsorption e.g. Tropical sprue, IBD. ▪ Blind loop syndrome +/- small bowel bacterial overgrowth. ▪ Fish tapeworm. •Drugs. ▪ Biguanides e.g.. Metformin. ▪ Oral contraceptive pill. ▪ Slow K, Cholestyramine.")
59
Indications for measuring serum vitamin B12 level
Haematological ▪ Isolated red cell macrocytosis ▪ Macrocytic anaemia ( esp. if MCV> 110fl) ▪ Pancytopenia ( esp. if MCV> 110fl) Neurological or psychiatric ▪ Peripheral neuropathy ▪ Cognitive change e.g. dementia ▪ Optic neuritis Gastrointestinal ▪ Investigation of possible malabsorption process Other (rare) ▪ Angular stomatitis, glossitis (sore beefy red tongue)
 ▪ Pancytopenia ( esp. if MCV> 110fl) Neurological or psychiatric. ▪ Peripheral neuropathy. ▪ Cognitive change e.g. dementia. ▪ Optic neuritis. Gastrointestinal. ▪ Investigation of possible malabsorption process. Other (rare) ▪ Angular stomatitis, glossitis (sore beefy red tongue)")
60
Clinical features Slow onset – symptoms of mild anaemia
Pallor and mild Jaundice( ineffective erythropoesis) Glossitis & angular stomatitis Neurological changes( B12< 60ng/L)( SCDC) ▪ Glove and stocking parasthesia ▪ Early loss of vibration sense ▪ Progressive weakness and ataxia ▪ Dementia SCDC: Subacute Combined Degeneration of the Spinal Cord
 Glossitis & angular stomatitis. Neurological changes( B12< 60ng/L)( SCDC) ▪ Glove and stocking parasthesia. ▪ Early loss of vibration sense. ▪ Progressive weakness and ataxia. ▪ Dementia. SCDC: Subacute Combined Degeneration of the Spinal Cord.")
61
Investigations FBC-Megaloblastic anaemia with hypersegmented neutrophils Serum B12 level- low Serum folate may be normal or high Anti-intrinsic factor ( anti-IF)- highly specific but +ve in 50-60% of PA. Parietal cell antibodies- +ve in 90%( PA) but less specific TSH & anti-thyroid Ab Test for coeliac disease Test for generalised malabsorption Endoscopy Schilling test- obsolete
- highly specific but +ve in 50-60% of PA. Parietal cell antibodies- +ve in 90%( PA) but less specific. TSH & anti-thyroid Ab. Test for coeliac disease. Test for generalised malabsorption. Endoscopy. Schilling test- obsolete.")
62
Treatment-Symptomatic
B12 deficiency without neurological involvement: ▪ 1mg Hydroxocobalamin 3 times a week for 2 weeks then every 3 months B12 deficiency with neurological involvement: ▪ 1mg Hydroxocobalamin every other day until no further improvement then every 2 months ▪ Folic acid 5mg daily for 4 weeks

63
Treatment-Asymptomatic
Serum B12> 150ng/l- Confirm test Significant proportion of these patients will go on to become symptomatic. Treat with oral vitamin B12 supplements + monitor level every 2-3months If no response then consideration given to parenteral B12 replacement

64
Case 1- Patient LS 53y old legal secretary Previously fit & well
A&E with RIF 3/12 general lethargy & inability to concentrate

65
Patient LS PMHx- Nil relevant
SHx-Single, good diet with mixture of animal & diary products No alcohol or smoking

66
On examination Pale, mildly jaundiced, sore and smooth tongue.
No pedal oedema, no hepatosplenomegally BP- 95/50, Pulse -110/min RIF tenderness with guarding? appendicitis

67
Investigations FBC- Hb- 6.8g/dl, WBC- 2.5 Plt- 58, MCV- 130fl,
U&E- NAD, LFT-Normal except Bili=26( 21- …), LDH- 8498, TSH- Normal, Hepatitis, HIV –ve.
, LDH- 8498, TSH- Normal, Hepatitis, HIV –ve.")
68
Blood film

71
What other investigations would you consider?
Folate- 9 B12- 72 GP & IF ab- Positive Coeliac Screen Negative

72
What is the management Vitamin B12 replacement- 1mg X 3 for 2 weeks.
Then 3 monthly Folic acid 5mg daily for 4 weeks

73
Case 2 - Patient MS 47yr man South East Asian origin
Saw GP with tiredness, SOBO PMHz- II DM on metformin SHx- Banker, strict vegetarian, Alcoholo, smokingo O/E- Unremarkable

74
Investigations Hb WBC- 3.2 Plt- 223, MCV- 120, LFT-NAD, LDH-640, U&E-NAD, TSH- Normal Blood film- macrocytosis with occasional hypersegmented neutrophils seen Serum B , Folate- 12, Ferritin 45 GP & IF ab, Coeliac screen- Negative

75
What is the management? Oral supplementation
Cyanocobalamin µg PO daily Recheck serum B12 in 2-3 months. Continue if replete If not, consider parenteral B12 injections.

76
Case 3- Patient DT 48y old Female Long H/O bloatedness Good diet.
SHx- Research nurse, no smoking or alcohol

77
Patient DT O/E- Unremarkable Bloods- Hb-9.8 WBC- 7.8 Plt-350 MCV-86fl
Blood film unremarkable U&E, LFT, TSH- NAD

78
Patient DT Ferritin- 6µ/dl, serum B12 – 160, Folate- 8
Tissue transglutaminase (tTG)
")
79
Patient DT Referred to gastroenterologist Given oral B12 and FeSO4
Recheck 3 monthly

80
MICROCYTIC HYPOCHROMIC ANAEMIA
What tests would you consider in the following cases: (Fer Vs Fer+HbEP) 25 y.o. lady, Norwegian, fatigued, Hb:100 g/l, RBC: 3000, MCV: 74fl, MCH: 26pg 50 y.o. lady , Cypriot, routine check, Hb:100 g/l, RBC 5000, MCV 70fl, MCH 24 pg
 25 y.o. lady, Norwegian, fatigued, Hb:100 g/l, RBC: 3000, MCV: 74fl, MCH: 26pg. 50 y.o. lady , Cypriot, routine check, Hb:100 g/l, RBC 5000, MCV 70fl, MCH 24 pg.")
81
Hb structure

82
Beta-Thalassaemia inheritance

83
Alpha-Thalassaemia inheritance

84
Regarding Ferritin Low Ferritin = Iron Deficiency
Raised Ferritin = Too much iron??

85
Causes of raised ferritin
Iron overload( Primary & Secondary) High Ferritin Without Iron Overload
 High Ferritin Without Iron Overload.")
86
Causes of Fe overload Primary ▪ Hereditary haemochromatosis Secondary
▪ Hereditary aceruloplasmin( Wilsons’ disease) Secondary ▪ Transfusion overload ▪ Ineffective erythropoiesis( thalassemia, sideroblastic anaemia) ▪ Excess dietary iron
 Secondary. ▪ Transfusion overload. ▪ Ineffective erythropoiesis( thalassemia, sideroblastic anaemia) ▪ Excess dietary iron.")
87
Causes of high ferritin without Fe overload
Liver disease Alcohol excess Chronic inflammatory conditions( RA, IBD, bacterial infection) Malignancy
 Malignancy.")
88
Evaluation of Fe loading tendency
FBC LFT Ferritin Transferrin saturation

89
Patient FT 59yr old female Severe RA On immunosuppressive drugs

90
Patient FT Hb- 99 WBC- 13.5 Plt-420 ESR- 43 CRP- 35, Ferritin 400µg/l
U&E, LFT- NAD Blood film Normochromic normocytic anaemia Serum electrophoresis- polyclonal increase in immunoglobulin

91
Patient FT Cause of raised ferritin- acute phase response
No specific therapy/investigations required for this Treat the RA

92
Patient GM 38yr old German ancestry Fit & well City Banker
Alcohol- 10u/week Well man clinic

93
Patient GM Hb- 154 WBC- 8.7 Plt- 210 Ferritin- 200µg/l
B12/Folate- within normal range U&E, LFT-NAD O/E- Nicely tanned but unremarkable otherwise Transferrin saturation ( serum Fe & TIBC)- 89%
- 89%")
94
What is the next specific test?
Test for HFE mutation Homozygous for C282Y/C282Y Diagnosis: Hereditary Haemochromatosis

95
Hereditary haemochromatosis
Elevated Fe with no obvious cause Family history TS > 55% for men & post menopausal women TS > 50% in premenopausal woman Test for HFE mutation Refer patient to gastro-enterologist in CUH Venesection will be done by haematologist

96
Other issues Sickle cell vaccination
Community follow up for long term haematological conditions Any others?

97
Sickle cell vaccinations
Pneumococcal Vaccine every 5 years Hib immunisation (once in lifetime) Tetravalent Meningococcal vaccine ACWY (once in lifetime) Hepatitis B vaccination Seasonal Flu Vaccination (annually) WHY????
 Tetravalent Meningococcal vaccine ACWY (once in lifetime) Hepatitis B vaccination. Seasonal Flu Vaccination (annually) WHY")
98
Community Follow-up for long term haematological conditions
Can you name 2 (previously presented in this talk)? Can you suggest others?
 Can you suggest others")
99
Any Questions??????

100
Thank you! Dr Stella Kotsiopoulou Haematology Specialty Doctor Croydon University Hospital

Similar presentations





















 Haematological Irritations Dr Anna Wood.>")
>")



i.>")
