Download presentation
Presentation is loading. Please wait.

2
Antidotes for cardiovascular drug poisoning New York University Department of Emergency Medicine/Medical Toxicology David H. Jang Assistant Professor Masters of Science Degree in Clinical Investigation (K30) Clinical and Translational Science Institute (CTSI) *Funded by the American Academy of Clinical Toxicology Junior Investigator Research Grant and also supported in part by grant 1UL1RR029893 from the National Center for Research Resources, National Institutes of Health.
 Clinical and Translational Science Institute (CTSI) *Funded by the American Academy of Clinical Toxicology Junior Investigator Research Grant and also supported in part by grant 1UL1RR from the National Center for Research Resources, National Institutes of Health..")
3
Case 44 year-old man presents with a “overdose” after an argument with his mother Patient obtained these medications from his mother who he still lives with in her basement

4
Case Vitals on presentation: Blood pressure: 140/90 mmHG Heart rate: 90 BPM Respiratory rate: 12 Temperature: 98.6 Oxygen saturation: 100% RA

5
Case 6 hours later…

6
Case Repeat Vitals: Blood pressure: 85/40 mmHG Heart rate: 40 BPM Respiratory rate: 20 Temperature: 98.6 Oxygen saturation: 100% RA

7
Case Intubated Hemodynamic support On norepinephrine On dopamine On epinephrine Still hypotensive…

8
Options?

10
Antidotes for cardiovascular drug poisoning

11
Cardiovascular drug class Antihypertensives Imidazolines Beta-blockers Calcium channel blockers ACE-Is and ARBs Cardioactive steroids Digoxin Antidysrhythmics Flecainide

12
Cardiovascular drug class Antihypertensives Imidazolines Beta-blockers Calcium channel blockers ACE-Is and ARBs Cardioactive steroids Digoxin Antidysrhythmics Flecainide

13
Not all things are created equal…

14
Beta-blockers Non-selective Carvedilol B 1 -selective Atenolol Esmolol Intrinsic sympathomimetic Pindolol

15
Beta-blockers Potassium channel blockers Sotalol Membrane-stabilizing Propanolol

16
Calcium channel blockers Phenylalkylamine Verapamil Benzothiazepine Diltiazem Dihydropyridines Nifedipine Amlodipine Nicardipine

17
Epidemiology

21
Beta and calcium channel blocker poisoning Clinical Features Bradycardia Hypotension Management Isotonic fluids Glucagon Inotropes/Pressors High-insulin Lipid emulsion

22
Beta and calcium channel blocker poisoning Clinical Features Bradycardia Hypotension Management Isotonic fluids Glucagon Inotropes/Pressors High-insulin Lipid emulsion

23
Beta and calcium channel blocker poisoning Clinical Features Bradycardia Hypotension Management Isotonic fluids Glucagon Inotropes/Pressors High-insulin Lipid emulsion

24
High insulin-euglycemic therapy (HIE)
")
25
Historical use Glucose-insulin- potassium (GIK) Acute myocardial infarction Heart failure Myocardium
 Acute myocardial infarction Heart failure Myocardium")
26
Background Hallmark of BB and CCB poisoning Bradycardia Vasodilation Decreased contractility

27
Background Altered myocardial physiology Hyperglycemia (pancreas/liver) Altered myocardial substrate use Inhibition of lactate oxidation
 Altered myocardial substrate use Inhibition of lactate oxidation")
28
Mechanism of action Alters ions homeostasis (potassium/calcium/so dium) Metabolic support Increase lactate uptake Epi and glucagon promote FFA use (increase energy)
 Metabolic support Increase lactate uptake Epi and glucagon promote FFA use (increase energy)")
29
Experimental evidence

30
Groups 1. Control: (0/6) 2. Epi: (4/6) (2/4) 3. HIE: (6/6) (6/6) 4. Glucagon: (3/6) (0/3)
 2. Epi: (4/6) (2/4) 3. HIE: (6/6) (6/6) 4. Glucagon: (3/6) (0/3)")
31
Experimental evidence Groups 1. Control: (0/6) 2. Epi: (4/6) (2/4) 3. HIE: (6/6) (6/6) 4. Glucagon: (3/6) (0/3)
 (2/4) 3. HIE: (6/6) (6/6) 4. Glucagon: (3/6) (0/3).")
32
Clinical experience

34
Adverse events Hypoglycemia Hypokalemia

35
Treatment guidelines

36
Intralipid

37
Background Triglycerides and phospholipids Primary triglycerides composed of linoleic, linolenic, and stearic acid pH 8, isotonic, various concentrations availiable (20% is primarily used)
")
38
Mechanism of action 1. Modulation of intracellular metabolism 2. Lipid sink 3. Activation of ion channels

39
Experimental evidence

41
Clinical experience

42
Adverse events

44
Treatment guidelines www.lipidrescue.org

45
Treatment guidelines

46
Summary Consider HIE early for suspected CCB poisoning Consider lipid emulsion when a patient is perimortem with suspected lipid-soluble medication

47
Methylene blue (MB)
")
48
Methylene blue Sentinel node detection Acquired methemoglobinemia Vasodilatory shock Anaphylaxis Sepsis

49
Nitric oxide synthase

50
Physiology of vascular tone

51
The evidence for MB

52
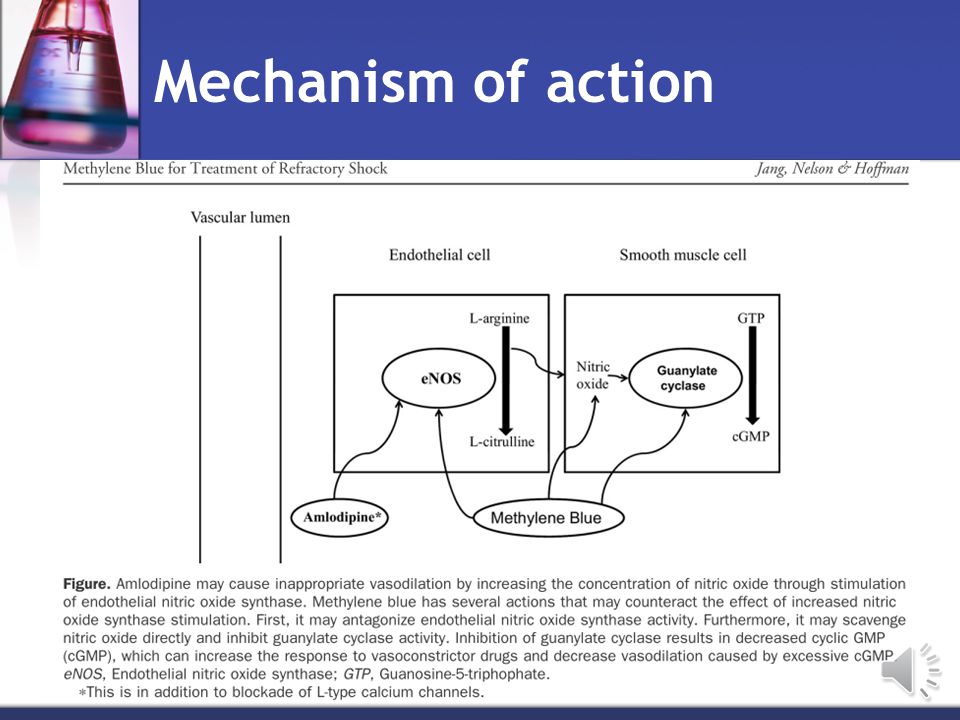
Mechanism of action

53
Vasodilatory shock from overdose?

54
Why calcium channel blockers?

56
Mechanism of action

57
So to test this…

58
Methods Design: Controlled, blinded animal design Subjects: Adult Sprague-Dawley rats (300-600 grams) Preparation (Instrumentation/sedation) Protocol: Phase 1: Dose-finding Phase 2: Methylene blue
 Preparation (Instrumentation/sedation) Protocol: Phase 1: Dose-finding Phase 2: Methylene blue")
59
Protocol summary and timeline Phase 1: Amlodipine dose determination 4 mg/kg: Incrementally increase dose 50% and decrease 50% (5 rats per group – 1, 2, 4, 6, 8 mg/kg) End-point: Decrease of mean arterial pressure to10% of baseline
 End-point: Decrease of mean arterial pressure to10% of baseline")
60
Amlodipine dose

61
Protocol summary and timeline Group 1: Amlodipine Normal saline (Control group) Group 2: Amlodipine Methylene Blue (Treatment group)
 Group 2: Amlodipine Methylene Blue (Treatment group)")
62
Protocol summary and timeline BaselineAmlodipine MB (2 mg/kg) or saline 0 mins180 mins Phase 2: Methylene blue treatment 15 min5 min 3-hours or until death Group 1: Amlodipine Normal saline (Control group) Group 2: Amlodipine Methylene Blue (Treatment group)
 or saline 0 mins180 mins Phase 2: Methylene blue treatment 15 min5 min 3-hours or until death Group 1: Amlodipine Normal saline (Control group) Group 2: Amlodipine Methylene Blue (Treatment group)")
63
Results Methylene blue-Pending Normal Saline-Pending

64
Questions?

Similar presentations














 Drug Therapy (Antihypertensives) ACEi B.B CCB D iuretics. Centrally acting agents: alphametyldopa, HTN + pregnancy.>")
 Dr Ivan Lambev>")



. CARDIOVASCULAR DISEASE AND DRUGS ► Basic cardiovascular physiology and pathology depends on the control of heart.>")



 for last 4 hours. He is.>")

