Download presentation
Presentation is loading. Please wait.

1
Mitral Stenosis Emerson Liu Echo conference Nov. 5, 2008

2
Etiologies Rheumatic Fever Congenital MS Rare complication of:
carcinoid, SLE, RA, mucopolysaccharidoses, Whipple, amyloid deposit MAC – may extend onto leaflet bases Obstructive physiology: myxoma, IE, cor triatriatum Cafergot Toxicity

3
MV Orifice Area Normal 4 - 6 cm2 Mild stenosis 1.6 - 2.5 cm2
Mod (usu Asx at rest) cm2 Severe ≤ 1.0 cm2
 cm2. Severe ≤ 1.0 cm2.")
4
S1 S2 OS S1 First heart sound (S1) is accentuated and snapping
Opening snap (OS) after aortic valve closure Low pitch diastolic rumble at the apex Pre-systolic accentuation (esp. if in sinus rhythm)
 after aortic valve closure. Low pitch diastolic rumble at the apex. Pre-systolic accentuation (esp. if in sinus rhythm)")
5
Tricuspid Regurgitation
Pathophysiology Right Heart Failure: Hepatic Congestion JVD Tricuspid Regurgitation RA Enlargement Pulmonary HTN Pulmonary Congestion LA Enlargement Atrial Fib LA Thrombi LA Pressure RV Pressure Overload RVH RV Failure LV Filling

6
Clinical Presentation
Dyspnea Hemoptysis Chest pain Palpitations and embolic events Ortner syndrome – hoarseness due to compression of the left recurrent laryngeal by dilated LA, tracheobronchial LN, and PA

7
Role of Echocardiography
Diagnose Mitral Stenosis Assess valve morphology – thickness, mobility, degree of calcification, extent of subvalvular involvement Assess hemodynamic severity: mean gradient, MV area, PAP Assess RV size and function. Assess suitability for percutaneous valvuloplasty Diagnose / assess concomitant valvular lesions Reevaluate pts with known MS with changing symptoms or signs, and F/U of asx pts with mod-severe MS

8
M-Mode 1. Thickened Mitral leaflets
2. Decreased E to F slope (increased EPSS) 3. Diastolic anterior motion of posterior leaflet 4. Abnormal septal motion 5. Left Atrial enlargement 6. Left Atrial thrombus 7. RV dilatation 8. Pulmonary hypertension 9. Small LV
 3. Diastolic anterior motion of posterior leaflet. 4. Abnormal septal motion. 5. Left Atrial enlargement. 6. Left Atrial thrombus. 7. RV dilatation. 8. Pulmonary hypertension. 9. Small LV.")
9
Thickened Leaflets in Mitral Stenosis
Mild Moderate Severe

10
Increased EPSS Mild Moderate Severe

11
Continuity equation

13
Diastolic Anterior Motion of Posterior Leaflet

14
2-D Echo Findings in MS 1. Thickened (> 3 mm) and calcified mitral leaflets and subvalvular apparatus. 2. “Hockey-stick” appearance of the anterior mitral leaflet in diastole (long-axis view). 3. “Fish-mouth” orifice in short-axis view. 4. Immobility of posterior leaflet. 5. Increased Left Atrial Size. 6. Small Left Ventricle.
. 3. Fish-mouth orifice in short-axis view. 4. Immobility of posterior leaflet. 5. Increased Left Atrial Size. 6. Small Left Ventricle.")
15
Rheumatic MS 31yo female w/ RF age 7, w/ palpitations. Mildly thickened mitral valve leaflets. Characteristic rheumatic deformity of the mitral valve leaflets with fused commissures and tethering of leaflet motion. LA upper limit of normal. MVA>2cm2. mild/mod MR

16
Rheumatic MS 36yo M w/ RMS. moderately thickened mitral valve leaflets. Characteristic rheumatic deformity of the mitral valve leaflets with fused commissures and tethering of leaflet motion. No MVP. Moderate thickening of mitral valve chordae.. Mild to moderate (1-2+) MR. PLAX LA 4.7cm
 MR. PLAX LA 4.7cm.")
18
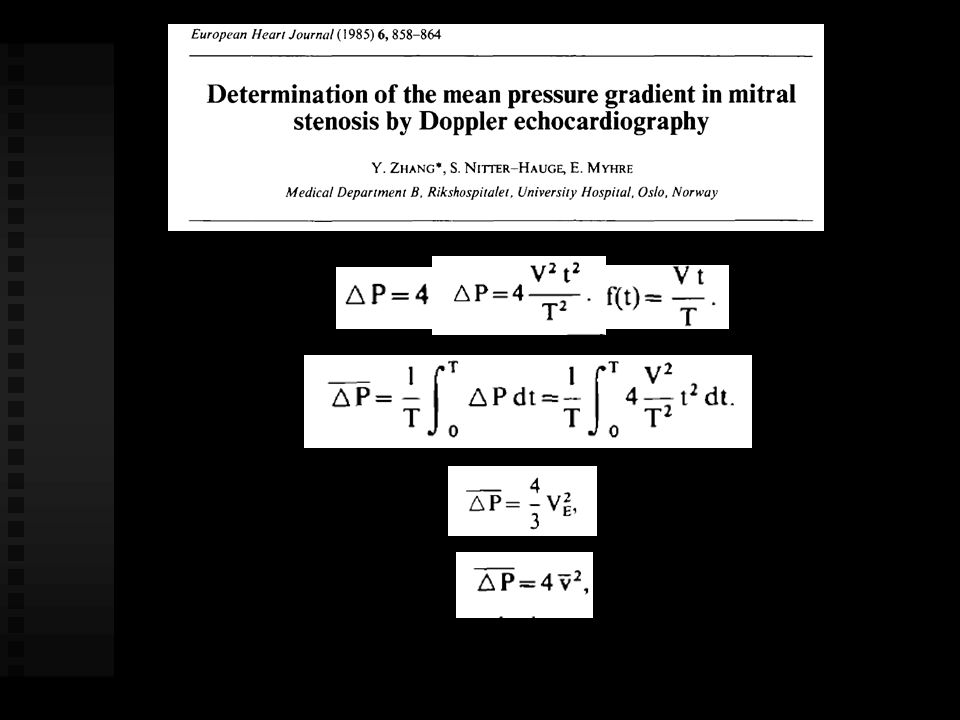
Pitfalls Pressure Gradient Intercept angle
beat to beat variability in AF Dependence on transmitral volume flow rate (exercise, coexisting mitral regurgitation)
")
19
Mitral valve Area the planar elliptical orifice is relatively constant in position in mid diastole, so that 2D short axis imaging of the diastolic orifice allows direct planimetry of the valve area The shape of the mitral valve inflow is similar to a funnel, with the narrowest CSA at the leaflet tips, and so it is important to move the image plan from apex to mitral valve to identify the smallest orifice. The approach is well validated compared with measurement of valve area by cardiac catheterization and at surgery This patient has relatively thin, flexible leaflets with little subvalvular involvement.

20
2D planimetry Mild valvular MS (MVA cm2)
")
21
Pitfalls 2D planimetry Image orientation Tomographic plane
2D gain settings Poor acoustic access Deformed valve anatomy post-valvuloplasty

23
220 t½ MVA =

25
Pitfalls T½ Valve Area Definition of Vmax and early diastolic slope
Nonlinear early diastolic velocity slope Sinus rhythm with a wave superimposed on early diastolic slope Afib: Hemodynamics averaged over 5-10 cycles Influence of coexisting AR Changing LV and LA compliances (post commisurotomy)
")
26
Continuity equation MVA x VTI (ms jet) = transmittal SV
= LVOT CSA x VTI* * in the absence of MR

27
PISA Method

28
Pitfalls Continuity equation Accurate measurement of transmitral SV
parallel intercept angle without significant MR

29
TEE Class IIa: 1. Check for LA thrombus in patients
considered for PBV or cardioversion. 2. Evaluate valve morphology and hemodynamics when transthoracic echo is suboptimal. Guide trans-septal puncture, or position of balloon, during PBV

30
Natural History Progressive, lifelong disease
Usually slow & stable in the early years Progressive acceleration in the later years 20-40 year latency from rheumatic fever to symptom onset Additional 10 years before disabling symptoms Twenty percent of patients in whom the diagnosis of symptomatic mitral stenosis is made die within 1 year, and 50% die within 10 years after diagnosis, without surgical intervention.

32
Exercise Hemodynamics
For patients who have exertional symptoms and in whom resting hemodynamics do not clearly indicate severe MS. With fixed valve area, ⇑ CO and HR will ⇑ transmitral gradient, LA pressure an PA pressure Dobutamine stress Doppler echocardiography is most useful where we used catheterization with exercise in the past: in those patients with symptoms not explainable by the calculated valve area, where a rise in mean mitral valve gradient to 18 mm Hg or above is consistent with a patient whose symptoms are due to obstruction to flow and who would benefit from mitral valve intervention.

33
Percutaneous Mitral Balloon Valvotomy
Class 1 Indications: Symptoms (NYHA II, III, IV), MVA ≤1.5cm², and valve morphology favorable for percutaneous balloon valvotomy, in the absence of left atrial thrombus or moderate to severe MR. Because MS is a mechanical obstruction to forward flow, the only definitive therapy is mechanical relief of this obstruction. Three procedures are effective in providing such therapy. These are BMV, open commissurotomy, and mitral valve replacement. Because clinical trials have found BMV to be superior to closed surgical commissurotomy, the latter procedure has been largely abandoned.
, MVA ≤1.5cm², and valve morphology favorable for percutaneous balloon valvotomy, in the absence of left atrial thrombus or moderate to severe MR. Because MS is a mechanical obstruction to forward flow, the only definitive therapy is mechanical relief of this obstruction. Three procedures are effective in providing such therapy. These are BMV, open commissurotomy, and mitral. valve replacement. Because clinical trials have found BMV to be superior to closed surgical commissurotomy, the latter procedure has been largely abandoned.")
34
Wilkins Score Patient selection for predicted hemodynamic results and risk of procedural complications. Suitability for BVM is determined by valve morphology and the amount of mitral regurgitation present. The Wilkins score gives a rough guide to the suitability of the mitral valve’s morphology for BMV. This scoring system assigns a point value from 1 to 4 for each of (1) valve calcification, (2) leaflet mobility, (3) leaflet thickening, and (4) disease of the subvalvular apparatus. In general, patients with a score of 9 and less than moderate mitral regurgitation have the best outcomes, although many patients have benefited from BMV despite higher valve scores.
 valve calcification, (2) leaflet mobility, (3) leaflet thickening, and (4) disease of the subvalvular apparatus. In general, patients with a score of 9 and less than moderate mitral regurgitation have the best outcomes, although many patients have benefited from BMV despite higher valve scores.")
35
Percutaneous Commissurotomy

36
Mitral Valve Repair Pts. with NYHA III-IV, MVA ≤ 1.5 cm², and valve morphology favorable for repair if PBV is not available. Pts. with NYHA III-IV, MVA ≤ 1.5 cm², and valve morphology favorable for repair if a left atrial thrombus is present despite anticoagulation. Pts. with NYHA III-IV, MVA ≤ 1.5 cm², and a nonpliable or calcified valve with decision to repair or replace valve made at time of surgery.

37
Mitral Valve Replacement
Pts. with NYHA III-IV, MVA ≤ 1.5 cm², and are not candidates for PBV or MV repair.

Similar presentations























 Assistant Professor of Medicine Medical Unit-4 LUMHS, Jamshoro.>")