Download presentation
Presentation is loading. Please wait.

1
Transposition of the Great Arteries
Francesca N. Delling, MD January 11, 2009

2
Cardiac Tube At the end of the third week of development one is left with a 5 chamber cardiac tube 1. Sinus Venosus – absorbed into the RA and contributes to formation of sinus node anterior cardinal veins become the IVC posterior cardinal veins become the SVC and coronary sinus 2. Atrial canal – develops into the atria 3. Ventricular canal – develops into the left venticle 4. Bulbis Cordis – develops into the RV and LV outflow tract (subpulmonic muscular conus and subaortic muscular conus. The subpulmonic conus elongates and the subaortic conus resorbs, allowing the aorta to move posteriorly and connect with the left ventricule: resorption of the subpulmonic instead of the subaortic conus may be central to transposition of the great arteries. Then ends of the tube are fixed – as the tube grows it is forced to bulge and twist. Looping of the heart tube changes it into a more complex structure consisting of two atria and two ventricles – the key is looping to the right

3
Heart is the 1st structure to demonstrate L-R asymmetry
1. Looping of the primitive heart tube ventrally and to the right to form the d-loop 2. D-loop places the bulbus cordis (future RV) to the right and the primitive ventricle to the left (future LV) 3. The postlooped heart then rotates slightly to place the RV in front of the left. The AV canal is devided by the endocardial cushions into the tricuspid and mitral orifices
 to the right and the primitive ventricle to the left (future LV) 3. The postlooped heart then rotates slightly to place the RV in front of the left. The AV canal is devided by the endocardial cushions into the tricuspid and mitral orifices.")
4
Complete Transposition of the Great Arteries
Ventriculoarterial discordance Also known as d-TGA (d = dextroposition of the bulboventricular loop) Aorta on the right and anterior 1. Aorta arises from the morphological RV 2. Pulmonary artery arises from the LV
 Aorta on the right and anterior. 1. Aorta arises from the morphological RV. 2. Pulmonary artery arises from the LV.")
5
Complete Transposition of the Great Arteries
Systemic and pulmonary circulation run in parallel need for a communication between the two - ASD, VSD (most common), or PDA to support life One of the most common cyanotic defects in the newborns If circulatory mixing via PDA, its physiological closure abrupt cyanosis and deterioration need for Rashkind atrial balloon septostomy until definite surgery When the ventricular septum (or atrial septum) is intact D-TGA is cyanotic in the first day of life (due to circulatory mixing via PDA).
, or. PDA to support life. One of the most common cyanotic. defects in the newborns. If circulatory mixing via. PDA, its physiological closure. abrupt cyanosis and. deterioration need for Rashkind. atrial balloon septostomy until. definite surgery. When the ventricular septum (or atrial septum) is intact D-TGA is cyanotic in the first day of life (due to circulatory mixing via PDA).")
6
Atrial switch procedures
Senning (1958): atrial baffle from autologous tissue to direct the venous return to the contralateral AV valve and ventricle Deoxygenated blood from the vena cava is directed to the MV and LV, PA, and PV blood is directed into the morphological RV and aorta
: atrial baffle from autologous tissue to direct the venous return to the contralateral AV valve and ventricle. Deoxygenated blood from the vena cava is directed to the MV and LV, PA, and PV blood is directed into the morphological RV and aorta.")
7
Atrial switch procedures
Mustard: atrial septum is excised, baffle is created with synthetic material Deoxygenated blood from the vena cava is directed to the MV and LV, PA, and PV blood is directed into the morphological RV and aorta. Both procedures provide excellent midterm results but are associated with long term complications

8
Late complications of atrial switch procedures:
Arrhythmias Late development of both brady and tachyarrhythmias Sinus node dysfunction common in adults Series of 534 children by Gelatt et al (J Am Coll Cardiol.1997;29: ) - NSR in 77% at 5 years, 40% at 20 years - 11% needed PPM - 14% had atrial flutter - 16% had a late death (due to arrhythmias and myocardial failure) Ventricular arrhythmias uncommon in the absence of severe ventricular dysfunction
 - NSR in 77% at 5 years, 40% at 20 years. - 11% needed PPM. - 14% had atrial flutter. - 16% had a late death (due to arrhythmias and myocardial. failure) Ventricular arrhythmias uncommon in the absence of severe. ventricular dysfunction.")
9
Late complications of atrial switch procedures:
Systemic Ventricular dysfunction and TR RV is the systemic ventricle TR secondary to annular dilatation (TVR not indicated) or damage at the time of VSD repair or endocarditis (TVR warranted) Treatment of systemic ventricular dysfunction is challenging: - No convincing data of utility of ACE-inhibitors - Caution with the use of beta-blockers (AVB, bradycardia) - Two-stage repair surgery (pulmonary artery banding to “retrain” the LV, followed by baffle take-down and arterial switch) is extensive and LV failure occurs after pulmonary banding
 or. damage at the time of VSD repair or endocarditis (TVR. warranted) Treatment of systemic ventricular dysfunction is challenging: - No convincing data of utility of ACE-inhibitors. - Caution with the use of beta-blockers (AVB, bradycardia) - Two-stage repair surgery (pulmonary artery banding. to retrain the LV, followed by baffle take-down and. arterial switch) is extensive and LV failure occurs after. pulmonary banding.")
10
Late complications of atrial switch procedures:
Atrial baffle obstruction and leaks Obstruction of SVC (with “SVC syndrome”) more common than IVC (hepatic congestion or cirrhosis). If significant stenosis, may need percutaneous balloon and stenting or even surgery Pulmonary vein stenosis much less common but may cause PHTN
 more common. than IVC (hepatic congestion or cirrhosis). If significant stenosis, may need percutaneous balloon. and stenting or even surgery. Pulmonary vein stenosis much less common but may. cause PHTN.")
11
Late complications of atrial switch procedures: Pulmonary hypertension
Occurs in 7% of those who survive to adulthood Cause unclear (in some cases: PV baffle obstruction) Risk factors: age > 2, shunts at ventricular or great artery level before repair (Newfeld EA et al. Am J Cardiol.1974;34: )
 Risk factors: age > 2, shunts at ventricular or great artery. level before repair (Newfeld EA et al. Am J Cardiol.1974;34: )")
12
Comparison between atrial switch procedures
Senning better than Mustard 340 pts (124 Mustard vs. 215 Senning) Heart, 2004; 90: Mortality 82 deaths (24%) Senning showed trend to better mortality but not statistically significant Baffle Obstruction 15% - Mustard 1% - Senning Senning patients had better functional status
 Heart, 2004; 90: Mortality. 82 deaths (24%) Senning showed trend to better mortality but not statistically significant. Baffle Obstruction. 15% - Mustard. 1% - Senning. Senning patients had better functional status.")
13
Atrial switch procedures and pregnancy
Pregnancy poses a significant volume load that may increase RV dimensions and is sometimes irreversible Poses a definite risk of deterioration of functional class, even if pt is asymptomatic Risk of congenital heart disease in the offspring, in the absence of a family history, is probably < 5% (Clarkson PM et al. J Am Coll Cardiol.1994;24: )
")
14
Arterial switch procedure
Jatene 1976 Usually performed in the first month of life Involves: transection of the great arteries, detachment of the coronary arteries with a “button” from the aortic wall Complications: coronary stenoses with sudden death or MI, RV outflow tract distortion, dilatation of neo-aortic root with AI

15
Rastelli procedure Used when d-TGA + large subaortic VSD and pulmonary stenosis A patch directs blood from the LV through the VSD to the aorta (1) PV is oversewn and a valved conduit is inserted from the RV to the PA to bypass the pulmonary stenosis (2)
")
16
Rastelli procedure (continued)
Advantages: LV functions as systemic ventricle Disadvantages: - Conduit degeneration and stenosis, necessitating reoperation - Atrial and ventricular arrhythmias with sudden death - Possible RV and LV failure

17
Echo: parasternal long-axis
Posterior pulmonary artery and anterior aorta aligned rather than in the usual crossing arrangement

18
Parasternal short-axis
Aorta is anterior and on the right

20
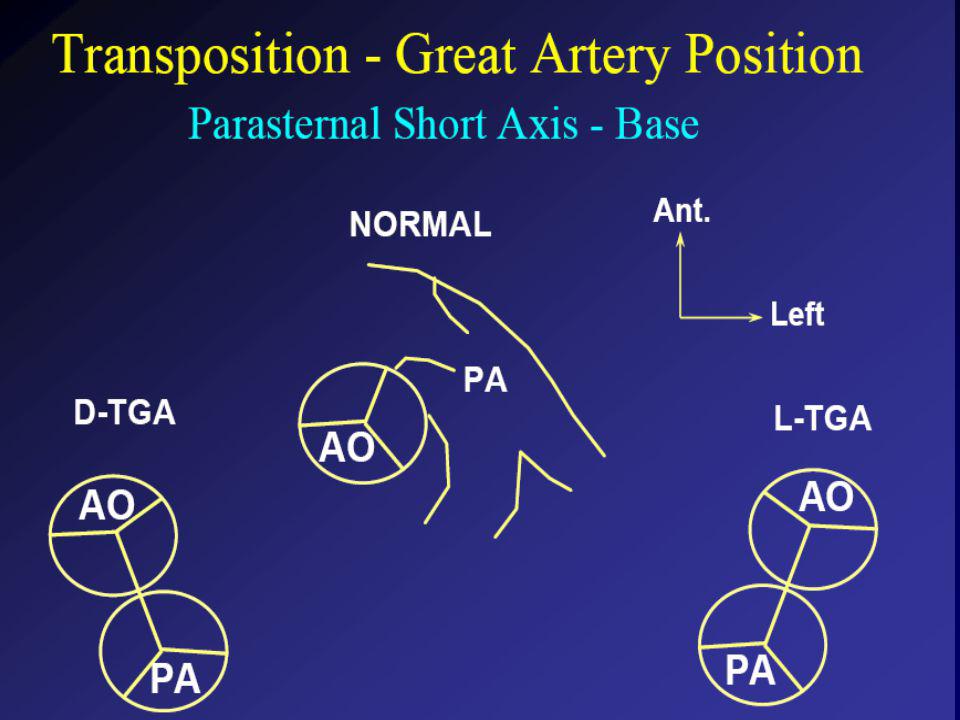
Parasternal short-axis base

21
4-chamber view

22
CMR: 4-chamber

25
LVOT

26
RV 2-chamber

27
Short axis

28
Congenitally corrected Transposition
RA enters the morphological LV PA, and left atrium communicates with morphological RV aorta

29
Congenitally corrected Transposition (continued)
Left-handed looping of the heart tube morphologic RV in levo-position AV discordance Aortopulmonary septum fails to rotate 180 ventriculoarterial discordance (although blood flows in the normal directions, it passes through the “wrong” chamber) Aorta anterior and to the left, great arteries may be side to side
 Aorta anterior and to the left, great arteries may be side to side.")
30
Congenitally corrected Transposition (continued)
Because the TV always enters a morphological RV it too is on the left side in the systemic circulation and is termed systemic AV valve The crux anatomy facilitates recognition of AV morphology because the TV is always lower than the MV and always enters a morphological RV (more difficult to identify, trabeculations are not always easy to see!) AV concordance AV discordance
 AV concordance. AV discordance.")
31
Congenitally corrected Transposition:
Associated anomalies VSD (70%): if large (LR flow), pts present in infancy or childhood with congestive heart failure. Reversal of flow R L leads to desaturation Pulmonary stenosis (40%), commonly subvalvular. Associated valvular PS also occurs Abnormalities of the systemic (tricuspid) AV valve (90%) Ebstein’s anomaly: - apical displacement of valve BUT no “saillike” anterior leaflet
: if large (LR flow), pts present in infancy. or childhood with congestive heart failure. Reversal of flow. R L leads to desaturation. Pulmonary stenosis (40%), commonly subvalvular. Associated. valvular PS also occurs. Abnormalities of the systemic (tricuspid) AV valve (90%) Ebstein’s anomaly: - apical displacement of valve BUT no saillike anterior. leaflet.")
32
Congenitally corrected Transposition:
Conduction anomalies AV node and His have unusual position Many have dual AV nodes Conduction system is vulnerable to fibrosis 2% per year incidence of CHB

33
Congenitally corrected Transposition:
CXR Levocardia or dextrocardia: vascular pedicle abnormally straight because ascending aorta is not visible on the R, and the convexities from desc aortic knob and PA are absent on the left; ventricular border is more straight. Dextrocardia: should be suspected when there is abdominal situs solitus (gastric bubble on the left) Levocardia Dextrocardia
 Levocardia. Dextrocardia.")
34
Congenitally corrected Transposition:
EKG Ventriculuar excitation begins at the septal endocardium of the right sided LV results in septal vector directed from r to L and posterior (inversion of the q waves) Ventriculuar excitation begins at the septal endocardium of the right sided LV
 Ventriculuar excitation begins at the septal endocardium of the right sided LV.")
35
Congenitally corrected Transposition:
Echocardiography Hypertrophied RV on the left Moderator Band Apical attachment of the TV

36
Congenitally corrected Transposition:
Echocardiography Overriding great vessels a. Aorta arises anteriorly and comes off the RV b. PA arises posteriorly from the LV

37
Congenitally corrected Transposition:
Echocardiography anterior and leftward aorta

39
Congenitally corrected Transposition:
Cardiac cath: hemodynamic assessment of associated anomalies evaluation of systemic AV valve regurgitation and ventricular function MRI: Defines ventricular function and volumes

40
Systemic ventricular failure and AV valve regurgitation
? Cause Inherent vulnerability to failure - concordant coronary anatomy: morphological RV perfused by single right coronary artery with limitations of perfusion Acar et al. Heart 1999: 20 pts with L-TGA and ETT MIBI all 20 had perfusion defects at rest, 17 worsened with exercise Controversy exists as to which comes first: AV valve regurgitation or ventricular failure

41
Systemic ventricular failure and AV valve regurgitation
PM implantation may precipitate deterioration in systemic ventricular function and worsening of AV valve regurgitation EF 40% prior to PM implantation, mod regurg. 18 months later EF 15% severe regurg

42
Congenitally corrected Transposition:
Surgical repair Two schools of thought: Classic approach – fix only the defects associated with the condition (VSD, systemic AV valve regurgitation) Newer approach is to restore the LV as the systemic ventricle (anatomical repair) Major advantage is drastically reduces risk of TR which is associated with RV failure and late sudden death
 Newer approach is to restore the LV as the systemic ventricle (anatomical repair) Major advantage is drastically reduces risk of TR which is associated with RV failure and late sudden death.")
43
Congenitally corrected Transposition:
Classical repair 118 pt classical repair J Thorac Cardiovasc Surg 117 (1999), pp. 1190–1203 15 % operative mortality 56% underwent reoperation within 20 yrs 48% survival rate at 20 years – CHF > 70%
, pp. 1190– % operative mortality. 56% underwent reoperation within 20 yrs. 48% survival rate at 20 years – CHF > 70%")
44
Congenitally corrected Transposition: Double switch operation
Venous Switch via Mustard or Senning Great vessel Switch Closure of VSD

45
Congenitally corrected Transposition
And VSD A patch can be inserted to tunnel the LV flow into the aorta, and the morphological RV is connected to the pulmonary artery via conduit “Rastelli technique”

46
Before anatomic repair (either double switch or Rastelli) LV needs to be prepared to function as a systemic ventricle pulmonary banding
 LV needs to be prepared to function as a systemic ventricle pulmonary banding")
47
Congenitally corrected Transposition:
Anatomic repair 54 pt restoration of LV – J Thorac CV Surg. 2003;125: Early mortality 5.6 % (3 pts) Long term mortality: 1 year – 94% survival 4 year – 90% survival 9 year – 90% Survival vs. Classic 60 – 83% (10 years)
 Long term mortality: 1 year – 94% survival. 4 year – 90% survival. 9 year – 90% Survival vs. Classic 60 – 83% (10 years)")
48
Congenitally corrected Transposition:
Anatomic repair Early mortality of 5% encouraging, but: - 7 pts with Rastelli needed repeat conduit, aortic valve replacement or transplantation. Balloon angioplasty of baffle obstruction or pulmonary stenosis also needed Need for re-intervention post anatomic repair confirmed by more recent paper by Sharma et al (J Thorac Cardiovasc Surg Feb;137) 68 patients (31 Rastelli/atrial switch; 37 arterial switch/atrial rerouting) early deaths, late re-operations, late deaths (LV dysfunction, tachyarrhytmias observed in both groups
 68 patients (31 Rastelli/atrial switch; 37 arterial switch/atrial rerouting) early deaths, late re-operations, late deaths (LV dysfunction, tachyarrhytmias. observed in both groups.")
49
Pregnancy and C-TGA Women with systemic EF <40% or significant systemic AV valve regurgitation should be counseled against pregnancy Series of Connolly et al ( J Am Coll Cardiol.1999;33:1962) 60 pregnancies 22 ♀ resulting in 50 live births (83%) none of the offspring had congenital heart disease no pregnancy related deaths 1 woman with significant AV valve regurgitation 1 had CHF 45 pregnancies 19 ♀ (Am J. Card. 1999;84:820-24) 27 live births; 12 miscarriages; 6 elective term 1 child with a congenital heart defect Mothers with 6 CV events 3 episodes of CHF 2 Episodes of increasing cyanosis, one CVA
 60 pregnancies 22 ♀ resulting in 50 live births (83%) none of the offspring had congenital heart disease. no pregnancy related deaths. 1 woman with significant AV valve regurgitation. 1 had CHF. 45 pregnancies 19 ♀ (Am J. Card. 1999;84:820-24) 27 live births; 12 miscarriages; 6 elective term. 1 child with a congenital heart defect. Mothers with 6 CV events. 3 episodes of CHF. 2 Episodes of increasing cyanosis, one CVA.")
50
Antibiotic prophylaxis
Prophylaxis is reasonable in patients with CHD with the highest risk for adverse outcome from infective endocarditis patients with prosthetic valves previous endocarditis unrepaired and palliated CHD repaired CHD within 6 months after the procedure repaired CHD with residual defects at or adjacent to the site of a prosthetic patch or prosthetic device that inhibits endothelization ACC/AHA guidelines for the management of adults with congenital heart disease. J Am Coll Cardiol Dec 2;52(23):e1-121
:e")
51
References Carole A. Warnes. Transposition of the great arteries. Circulation 2006;114: Yale University School of Medicine. Congenital Heart Disease Echo Atlas.

52
Thank you

Similar presentations