Download presentation
Presentation is loading. Please wait.

1
INHIBITOR TO ANTIHEMOPHILIC FACTOR Djajadiman Gatot Division of Hematology Oncology Department of Child Health FMUI - CMGH

2
What is inhibitor? (to factor VIII) Inhibitor are polyclonal allo-antibodies of the IgG molecules predominantly of the IgG4 subclass that directed to FVIII Highly heterogeneous among patients Display changes in epitope specificity over time Its synthesis requires activated CD4+ cells Neutralized the procoagulant activity of FVIII and render infusion of FVIII inefficient
 Inhibitor are polyclonal allo-antibodies of the IgG molecules predominantly of the IgG4 subclass that directed to FVIII Highly heterogeneous among patients Display changes in epitope specificity over time Its synthesis requires activated CD4+ cells Neutralized the procoagulant activity of FVIII and render infusion of FVIII inefficient.")
3
How do inhibitor develop? FVIII is a soluble glycoprotein; its adminis- tration to an individual with normal immunocompetence will results in immune response The FVIII genotype has major influence for the development of inhibitors

4
Who will develop inhibitor? FVIII genotype and the risk of developing inhibitor: - large deletion ( 88%) - nonsense mutations ( 60%) - intron-22 inversion ( 21%) - small deletions/insertions ( 20%) - missense mutations ( 5%)
 - nonsense mutations ( 60%) - intron-22 inversion ( 21%) - small deletions/insertions ( 20%) - missense mutations ( 5%).")
5
Inhibitor Location of major factor VIII inhibitory epitopes

6
Who will develop inhibitor? HLA and the risk of developing inhibitor ethnic group, African-American 2x than whites family history of antibodies to FVIII inherited predisposition hemophilic siblings >> extended hemophilic relatives any severe hemophilia

7
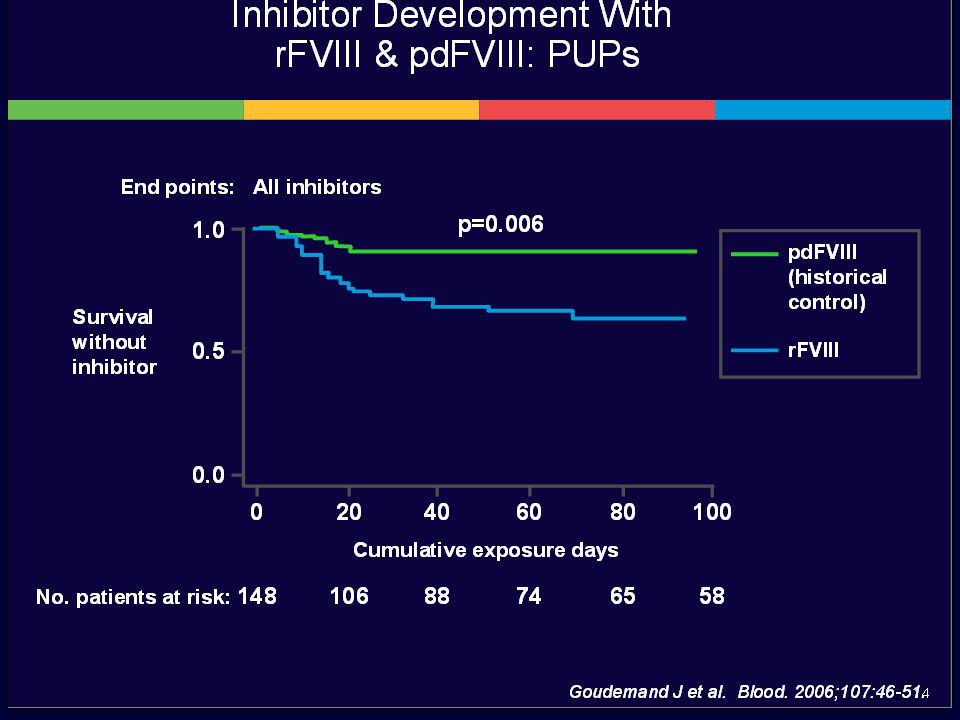
When will inhibitor develop? The majority of inhibitors develop during childhood, at an average of 12 years Reported studies: Inhibitor development occurred between the age of 1 – 2 yrs, after an average of 10 treatments with rFVIII Inhibitor risk is greatest during the first 50 exposures to rFVIII

8
What is the incidence of inhibitor? Inhibitors of FVIII develop in up to 30% of hemophilia A patients and significantly more frequent in severe hemophilia

9
Why ‘only’ 30% of hemophilia patients have inhibitor? There are several possible mechanisms: 1)anti-FVIII antibodies are neutralized in the periphery, 2)B cells (and T cells) can be rendered anergic by intrinsic mechanism, 3)any antibodies produced are primarily directed towards sites of the FVIII molecule that are not involved in its function
anti-FVIII antibodies are neutralized in the periphery, 2)B cells (and T cells) can be rendered anergic by intrinsic mechanism, 3)any antibodies produced are primarily directed towards sites of the FVIII molecule that are not involved in its function.")
10
InhibitorClassificationTreatment Low titer (< 5 BU) Higher/more frequent dose of factor concentrate High titer (> 5 BU) By-passing agent Immune tolerance induction Rituximab (?) Haemophilia 2006;12:7–18. Haemophilia 2006;12:218–22.

11
Management of bleeding in patient with inhibitor The ultimate goals of treatment are: 1.Resolution of bleeding diathesis 2.The elimination of the inhibitor

21
Resolution of Bleeding Diathesis Replacement therapy: ~ human FVIII (high-dose) ~ recombinant FVIII (2 nd and 3 rd generation) ~ porcine FVIII Bypass therapy: ~ prothrombin complex concentrate (PCC) ~ activated PCC ~ recombinant FVIIa
 ~ recombinant FVIII (2 nd and 3 rd generation) ~ porcine FVIII Bypass therapy: ~ prothrombin complex concentrate (PCC) ~ activated PCC ~ recombinant FVIIa")
22
Contact activation XIa IXa+VIII APC TM TF-VIIa Xa+V IIaFibrinFibrinolysis TAFI TFPI TM

23
The elimination of inhibitor Immune tolerance induction (ITI), - may take up to 1 – 3 years to achieve tolerance - very high cost - successfully eradicating up to 90% of FVIII inhibitor Immunomodulation, + cytostatics: cyclophosphamide, 6-mercaptopurine + immunosuppressant: azathioprine, cyclosporin + corticosteroids + gamma globulin + plasmapheresis
, - may take up to 1 – 3 years to achieve tolerance - very high cost - successfully eradicating up to 90% of FVIII inhibitor Immunomodulation, + cytostatics: cyclophosphamide, 6-mercaptopurine + immunosuppressant: azathioprine, cyclosporin + corticosteroids + gamma globulin + plasmapheresis")
24
Immune tolerance induction The dose: High level inhibitors (>100 BU), treated with high-dose regimen: 100-200 IU kg -1 day -1 Low titer inhibitors (5-100 BU), treated either with high- or low-dose regimen: 50 IU kg -1, 3 times per week
, treated with high-dose regimen: IU kg -1 day -1 Low titer inhibitors (5-100 BU), treated either with high- or low-dose regimen: 50 IU kg -1, 3 times per week")
25
Immune tolerance induction The cost: British: 0.25 – 1 million £ per patient Italy: 18,000 € per patient, monthly USA: 1,7 million $ per patient

26
Thank You

Similar presentations








>")


 Resistance-Associated Variant (RAV) Loci in Genotype 1a and 1b Patients:>")














