Download presentation
Presentation is loading. Please wait.

1
ARV failure and resistance for the paediatrician
Douglas Watson, M.D. University of Maryland 11 December 2013

2
REVERSE TRANSCRIPTASE INHIBITORS (NRTIs & NNRTIs)
Integrase inhibitors Reverse transcriptase inhibitors (nucleoside and non-nucleoside RT inhibitors) prevent the synthesis of a DNA copy of the viral RNA genome. Protease inhibitors act on the virus after it buds through the cell membrane, inhibiting the cutting of long inactive polypeptide chain into shorter functional proteins that the virus needs to infect the next cell. As our bodies do not perform reverse transciption, inhibiting that step should not adversely affect us. But many of the HIV nucleoside reverse transcriptase inhibitors do have an effect on the enzyme that replicates mitochondrial DNA- accounting for the toxicity of the NRTIs. There is one fusion inhibitor in clinical use, but it is extremely expensive to make. More useful integrase inhibitors show promising early results in humans. Fusion Inhibitors PROTEASE INHIBITORS Attachment Inhibitors HIV DRUG TARGETS
 prevent the synthesis of a DNA copy of the viral RNA genome. Protease inhibitors act on the virus after it buds through the cell membrane, inhibiting the cutting of long inactive polypeptide chain into shorter functional proteins that the virus needs to infect the next cell. As our bodies do not perform reverse transciption, inhibiting that step should not adversely affect us. But many of the HIV nucleoside reverse transcriptase inhibitors do have an effect on the enzyme that replicates mitochondrial DNA- accounting for the toxicity of the NRTIs. There is one fusion inhibitor in clinical use, but it is extremely expensive to make. More useful integrase inhibitors show promising early results in humans. Fusion Inhibitors. PROTEASE INHIBITORS. Attachment Inhibitors. HIV DRUG TARGETS.")
3
Antiretrovirals in the U.S.- 2013
Nucleoside analogues (NRTIs) Zidovudine (ZDV, AZT, Retrovir) Lamivudine (3TC, Epivir) Tenofovir (TDF, Viread) Emtricitabine (FTC, Emtriva) Abacavir (ABC, Ziagen) Stavudine** (D4T, Zerit) Didanosine** (DDI, Videx) Protease inhibitors Lopinavir/ritonavir (LPV/r, Kaletra) Atazanavir (ATV, Reyataz) Fosamprenavir (fAMP, Lexiva) Darunavir (DRV, Prezista) Tipranavir* (TPV, Aptivus) Saquinavir* (SQV, Invirase) Nelfinavir* (NFV, Viracept) Indinavir** (IDV, Crixivan) Non-nucleoside reverse transcriptase inhibitors (NNRTIs) Efavirenz (EFV, Sustiva) Nevirapine (NVP, Viramune) Etravirine (ETV, Intelence) Delavirdine** (DLV, Rescriptor) Rilpivirine (Edurant) Integrase inhibitors Raltegravir (RAL, Isentress) Elvitegravir Dolutegravir (Tivacay) Attachment inhibitor Maraviroc (Selzentry) Fusion inhibitor Enfuvirtide* (T-20, Fuzeon) P450 inhibitor (for “boosting” PIs) Ritonavir (RTV or r, Norvir) Cobicistat *Uncommonly used. **No useful role
 Zidovudine (ZDV, AZT, Retrovir) Lamivudine (3TC, Epivir) Tenofovir (TDF, Viread) Emtricitabine (FTC, Emtriva) Abacavir (ABC, Ziagen) Stavudine** (D4T, Zerit) Didanosine** (DDI, Videx) Protease inhibitors. Lopinavir/ritonavir (LPV/r, Kaletra) Atazanavir (ATV, Reyataz) Fosamprenavir (fAMP, Lexiva) Darunavir (DRV, Prezista) Tipranavir* (TPV, Aptivus) Saquinavir* (SQV, Invirase) Nelfinavir* (NFV, Viracept) Indinavir** (IDV, Crixivan) Non-nucleoside reverse transcriptase inhibitors (NNRTIs) Efavirenz (EFV, Sustiva) Nevirapine (NVP, Viramune) Etravirine (ETV, Intelence) Delavirdine** (DLV, Rescriptor) Rilpivirine (Edurant) Integrase inhibitors. Raltegravir (RAL, Isentress) Elvitegravir. Dolutegravir (Tivacay) Attachment inhibitor. Maraviroc (Selzentry) Fusion inhibitor. Enfuvirtide* (T-20, Fuzeon) P450 inhibitor (for boosting PIs) Ritonavir (RTV or r, Norvir) Cobicistat. *Uncommonly used. **No useful role.")
4
WHO 2013 recommendations for 1st-line ART in children < 3 y of age
“ABC should be considered the preferred NRTI whenever possible.” LPV//r should not be given to infants < 14 d of age or in premature infants until after 14 d after their due date

5
WHO 2013: Start with LPV/r and switching to NNRTI?
NOTE: The quoted study enrolled only children with history of SD NVP exposure The quoted study used < 50 copies/ml as primary endpoint and < 1,000 c/ml as secondary endpoint- NOT < 400 c/ml as stated above. The switch-to-NVP group had fewer cases of VL > 50 but more cases of VL > 1,000 and more resistance than group that stayed on LPV/r

6
WHO 2013 recommendations for 1st line ART in children > 3 y of age

7
Treatment failure: progressive steps, different definitions
Potency failure Adherence failure Virologic failure Genotypic failure (resistance) There are multiple definitions or types of treatment failure. If the regimen is inadequate or the dosage too low (potency failure), or if there is nonadherence (adherence failure), then virologic failure (a detectable viral load) will develop. Genotypic failure will develop, the time course depending on the genetic barrier to resistance and how high the viral load is- the lower barrier to resistance and higher the viral load, the more rapidly resistance is selected. With higher levels of viral load, eventually the CD4 stops going up and begins to fall (immunologic failure). Even later, the patient experiences renewed symptoms- clinical failure. Immunologic failure Clinical failure
 There are multiple definitions or types of treatment failure. If the regimen is inadequate or the dosage too low (potency failure), or if there is nonadherence (adherence failure), then virologic failure (a detectable viral load) will develop. Genotypic failure will develop, the time course depending on the genetic barrier to resistance and how high the viral load is- the lower barrier to resistance and higher the viral load, the more rapidly resistance is selected. With higher levels of viral load, eventually the CD4 stops going up and begins to fall (immunologic failure). Even later, the patient experiences renewed symptoms- clinical failure. Immunologic failure. Clinical failure.")
8
Expected fall in viral load
Time Log fold drop in viral load Fold-drop in viral load Viral load (example) -- 600,000 100,000 1 month 2 100+ < 6,000 < 1,000 3 months 3 1,000 600 100 6 months 4 10,000 60 <50 If viral load at these follow up times is 3-fold or more than these examples, full suppression not likely
 , , month < 6,000. < 1, months. 3. 1, months , <50. If viral load at these follow up times is 3-fold or more than these examples, full suppression not likely.")
9
Days = 0 is day HAART started (6 weeks of age)
Days = 0 is day HAART started (6 weeks of age). Note initial rapid rise in viral load after infection at birth. Also not 2-phase decay in viral load on HAART- an initial rapid drop (about 1000-fold) in first 2-3 weeks, then slower decline to undetectable by ultrasensitive assay by 140 days of treatment. This girl is now 8 years old and has had an undetectable viral load since about 4 months of age.
. Note initial rapid rise in viral load after infection at birth. Also not 2-phase decay in viral load on HAART- an initial rapid drop (about 1000-fold) in first 2-3 weeks, then slower decline to undetectable by ultrasensitive assay by 140 days of treatment. This girl is now 8 years old and has had an undetectable viral load since about 4 months of age.")
10
Course of treatment failure
Start ZDV/3TC/NVP Clinical deterioration Gradual ZDV resistance Nonadherence NVP resistance 3TC resistance CD4 Count Viral load The time course of treatment failure. The VL drops very rapidly after starting HAART, then more slowly. At the indicated point, the patient has a period of nonadherence. Very rapidly, NVP resistance (K103N mutation) is selected. What follows from this point will occur whether or not adherence improves. Within 1-3 months, 3TC resistance (M184V) is selected. This increases sensitivity to ZDV, but at this point ZDV is the only active drug- not enough to hold back the virus. The CD4 count has continued to improve, even after development of NVP resistance- we know that ZDV/3TC will make someone with AIDS better for a year or so. With time, however, the CD4 stops rising and starts to fall. One by one, ZDV-selected thymidine analogue mutations evolve. (TAMS: RT mutations at 41, 67, 69, 70, 210, 211, 215 and others- 215 and 41 being the most important.) Only as the viral load gets very high again and the CD4 has fallen does the patient have recurrent symptoms. At this point there is resistance to all 3 drugs with cross-resistance to EFV and complete or partial cross-resistance to all NRTIs. 1 year 2 years
 is selected. What follows from this point will occur whether or not adherence improves. Within 1-3 months, 3TC resistance (M184V) is selected. This increases sensitivity to ZDV, but at this point ZDV is the only active drug- not enough to hold back the virus. The CD4 count has continued to improve, even after development of NVP resistance- we know that ZDV/3TC will make someone with AIDS better for a year or so. With time, however, the CD4 stops rising and starts to fall. One by one, ZDV-selected thymidine analogue mutations evolve. (TAMS: RT mutations at 41, 67, 69, 70, 210, 211, 215 and others- 215 and 41 being the most important.) Only as the viral load gets very high again and the CD4 has fallen does the patient have recurrent symptoms. At this point there is resistance to all 3 drugs with cross-resistance to EFV and complete or partial cross-resistance to all NRTIs. 1 year. 2 years.")
11
Mechanism of reverse transcriptase inhibitors cDNA
NRTI = Nucleoside reverse transcriptase inhibitor NNRTI = Non-nucleoside reverse transcriptase inhibitor HIV reverse transcriptase cDNA ABC HIV reverse transcriptase copies the viral RNA into DNA. The nucleoside analogues (D4T in this case), are added onto the growing DNA chain. But because they are blocked at one end, the next natural dNTP cannot be added- and the DNA chain is terminated. The NNRTIs work by binding to the RT molecule, blocking its activity. NRTI (such as ABC(P3) is added onto cDNA chain, blocking further reverse transcription NNRTI (NVP or EFV) Blocks reverse transcriptase by binding at active site
, are added onto the growing DNA chain. But because they are blocked at one end, the next natural dNTP cannot be added- and the DNA chain is terminated. The NNRTIs work by binding to the RT molecule, blocking its activity. NRTI (such as ABC(P3) is added onto cDNA chain, blocking further reverse transcription. NNRTI (NVP or EFV) Blocks reverse transcriptase by binding at active site.")
12
The K103N mutation: how it can take over
Sensitive K103 HIV wild type (wt) Resistant 103N HIV NVP blocks sensitive HIV, not resistant HIV Nevirapine wt always present NVP blocks the grown of the wild-type virus (with K at position 103). But the extremely rare, randomly produced mutant, with N at position 103, is able to grow. Within 2-4 weeks the mutant resistant virus takes over as the predominant virus in the blood. In presence of NVP, only the resistant virus grows. Soon almost all virus is resistant!
 Resistant 103N HIV. NVP blocks sensitive HIV, not resistant HIV. Nevirapine. wt always present. NVP blocks the grown of the wild-type virus (with K at position 103). But the extremely rare, randomly produced mutant, with N at position 103, is able to grow. Within 2-4 weeks the mutant resistant virus takes over as the predominant virus in the blood. In presence of NVP, only the resistant virus grows. Soon almost all virus is resistant!")
13
Note that these patients were failing (by VL monitoring) for only 4-5 months- which is too early to detect failure using CD4 counts or clinical signs- yet they had developed significant resistance- nearly all NNRTI and 3TC resistance, and significant amount of other NRTI mutations. Note that these other mutations were more common in patients with VL > 4 log (> 10,000) copies/ml. Drug resistance mutations in Thai patients failing D4T/3TC/NVP for an average of 4-5 months by viral load monitoring. Sungkanuparph S. CID 2007; 44:447–52

14
Nucleoside reverse transcriptase inhibitor resistance and cross-resistance
Zidovudine (AZT) Stavudine (D4T) Tenofovir (TDF) Abacavir (ABC) Didanosine (DDI) Lamivudine (3TC) or Emtricitabine (FTC) Thymidine analogue mutations (TAMS) Resistance AZT D4T TDF TAMS +184V 3TC, FTC > D4T, DDI, AZT, ABC > TDF K65R Resistance TDF, ABC, DDI D4T 3TC, FTC Hypersensitivity AZT L74V + M184V Resistance ABC DDI 3TC FTC Hypersensitivity AZT TDF M184V Resistance 3TC FTC Hypersensitivity TDF > AZT > D4T Q151M Resistance AZT, D4T, DDI, ABC > TDF, 3TC, FTC
 Stavudine. (D4T) Tenofovir. (TDF) Abacavir. (ABC) Didanosine. (DDI) Lamivudine. (3TC) or Emtricitabine (FTC) Thymidine analogue mutations. (TAMS) Resistance. AZT. D4T. TDF. TAMS +184V. 3TC, FTC > D4T, DDI, AZT, ABC > TDF. K65R. Resistance. TDF, ABC, DDI. D4T. 3TC, FTC. Hypersensitivity. AZT. L74V. + M184V. Resistance. ABC. DDI. 3TC. FTC. Hypersensitivity. AZT. TDF. M184V. Resistance. 3TC. FTC. Hypersensitivity. TDF > AZT. > D4T. Q151M. Resistance. AZT, D4T, DDI, ABC > TDF, 3TC, FTC.")
15
Summary: NRTI resistance patterns & options
Regimen Common pattern Other patterns Geno Resistance Options* D4T/3TC M184V, TAMS 3TC > D4T, ZDV, ABC, DDI >TDF TDF/3TC (+/-ZDV)> (ZDV/3TC/ABC) (how good depends on # of TAMS) K65R, M184V or M184V, Q151M 3TC, TDF, ABC, DDI, d4T 3TC, ZDV, D4T, DDI, ABC, (TDF) ZDV/3TC (TDF/3TC) “ TDF/3TC K65R, (M184V) ABC/3TC M184V, L74V 3TC, ABC, DDI M184V, K65R DDI/3TC *Options: Underline = excellent, () = weak, others fair
> (ZDV/3TC/ABC) (how good depends on # of TAMS) K65R, M184V. or. M184V, Q151M. 3TC, TDF, ABC, DDI, d4T. 3TC, ZDV, D4T, DDI, ABC, (TDF) ZDV/3TC. (TDF/3TC) TDF/3TC. K65R, (M184V) ABC/3TC. M184V, L74V. 3TC, ABC, DDI. M184V, K65R. DDI/3TC. *Options: Underline = excellent, () = weak, others fair.")
16
NNRTI resistance 1st generation (nevirapine, efavirenz, delavirdine)
High potency but low genetic barrier to resistance Most commonly K103N- resistance to all 1st generation NVP also selects for Y181C (especially in newborns) which has mild effect on EFV but associated with increased failures Other mutation patterns also seen 2nd generation (Etravirine) NO EFFECT of K103N Resistance increases with other NNRTI mutations- 3 or more yield
 which has mild effect on EFV but associated with increased failures. Other mutation patterns also seen. 2nd generation (Etravirine) NO EFFECT of K103N. Resistance increases with other NNRTI mutations- 3 or more yield.")
18
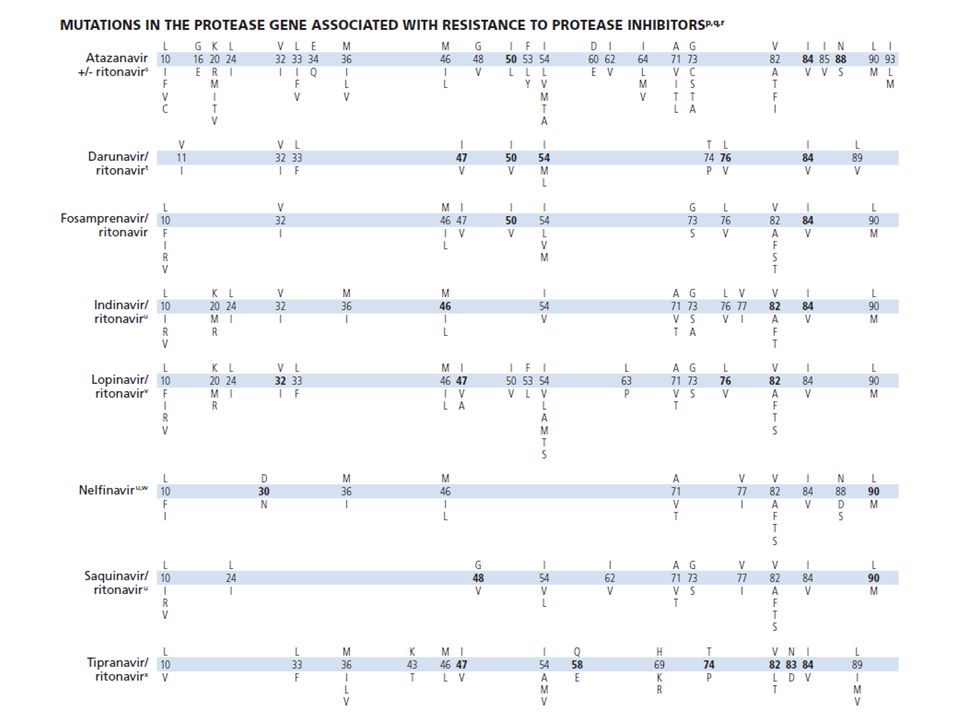
Protease inhibitor resistance
Some PIs select for drug-specific mutations (e.g. NFV, ATV) Some PIs can be boosted or unboosted (ATV, fAPV)- low-level resistance may be clinically significant if not boosted Boosted PIs more durable Resistance to LPV requires 5-10 mutations Virologic failure while receiving LPV/r usually due to nonadherence Prolonged virologic failure while on LPV/r eventually will lead to LPV resistance
 Some PIs can be boosted or unboosted (ATV, fAPV)- low-level resistance may be clinically significant if not boosted. Boosted PIs more durable. Resistance to LPV requires 5-10 mutations. Virologic failure while receiving LPV/r usually due to nonadherence. Prolonged virologic failure while on LPV/r eventually will lead to LPV resistance.")
19
Drug resistance testing
Commercial methods start with RT PCR of bulk virus in plasma Not sensitive to minor strains- e.g. genotyping (sequencing) cannot detect strain representing < 10-25% of circulating virus When to get resistance testing (resource-rich) Baseline: resistant strains (especially NNRTI resistance) circulating in population Whenever resistance suspected (e.g. failing and patient appears adherent) Selective pressure- patient taking medication
 cannot detect strain representing < 10-25% of circulating virus. When to get resistance testing (resource-rich) Baseline: resistant strains (especially NNRTI resistance) circulating in population. Whenever resistance suspected (e.g. failing and patient appears adherent) Selective pressure- patient taking medication.")
20
HIV drug resistance genotype
RT PCR bulk plasma virus to produce cDNA Sequence pol gene Derive predicted amino acid sequence Identify mutations known to confer resistance (e.g. Stanford database, IAS-USA, etc.) Virtual phenotype™ genotype interpretation Identified set of significant mutations is matched with massive database of genotype-phenotype correlations Reported as predicted fold resistance (used to also give number of matches) Fold-resistance interpreted according to in vitro or clinical measure of activity
 Virtual phenotype™ genotype interpretation. Identified set of significant mutations is matched with massive database of genotype-phenotype correlations. Reported as predicted fold resistance (used to also give number of matches) Fold-resistance interpreted according to in vitro or clinical measure of activity.")
22
IAS-USA, Topics in HIV Medicine, March 2013

23
IAS-USA, Topics in HIV Medicine, March 2013

26
Interpretation of resistance testing
Complete treatment and viral load history are essential What is current regimen and is patient taking it? Many resistance mutations cause decreased viral fitness: if there is not selective pressure, wild-type virus rapidly outgrows mutant, but archive of mutant remains

27
WHO 2013

28
Johnny B. Goode Newly infected adolescent CD4 = 320, VL = 58,000
Prescribed TDF/FTC/ATV/r VL 1 month later = 5,200 VL at 2 months = 4,000 Genotype is wild-type How do you interpret this situation? How to proceed?

Similar presentations












 University of Nairobi ISO 9001:2008 1 Certified>")




 Gareth Tudor-Williams.>")

 Stocrin (Efavirenz 600mg) Kaletra (Lopinavir 200mg.>")


