Download presentation
Presentation is loading. Please wait.

1
Ruptured Abdominal Aortic Aneurysms
Eliza Long

2
Treatment of the Ruptured Abdominal Aortic Aneurysm
Diagnosis Clinical Imaging Resuscitation Surgery Different options Complications

3
Diagnosis Clinical Presentation
“Classic triad:” Severe abdominal pain Hypotention An episode of syncope may be a hint Pulsatile mass Large girth may obscure Less common symptoms: Groin/flank pain, hematuria, groin hernia all secondary to increased intra-abdominal pressure Congestive Heart Failure with JVD and abdominal bruit if patient has ruptured into the Vena Cava

4
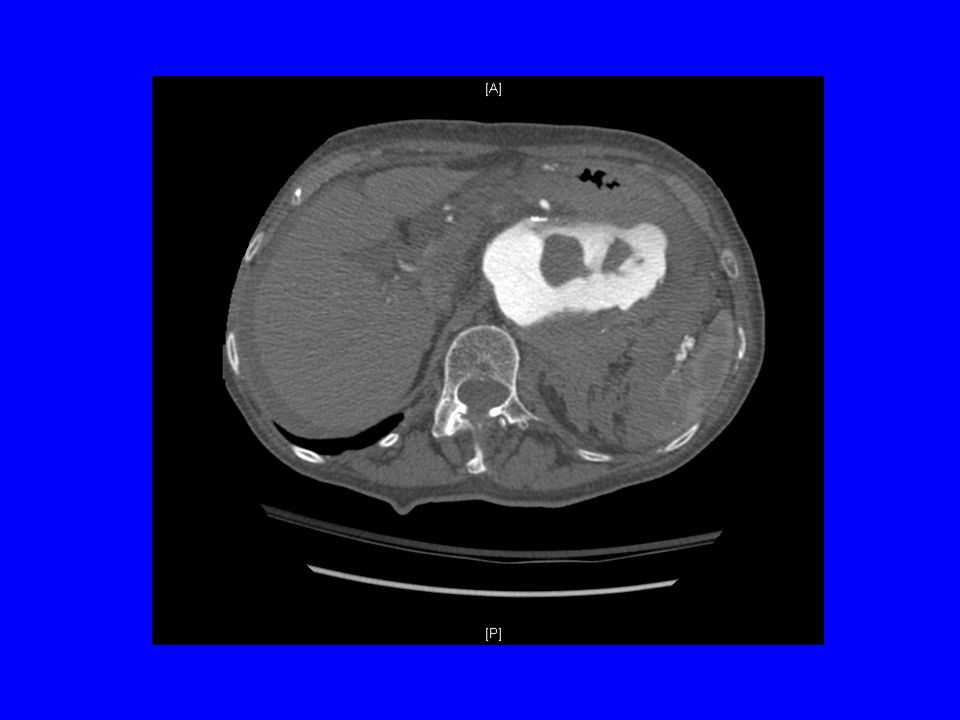
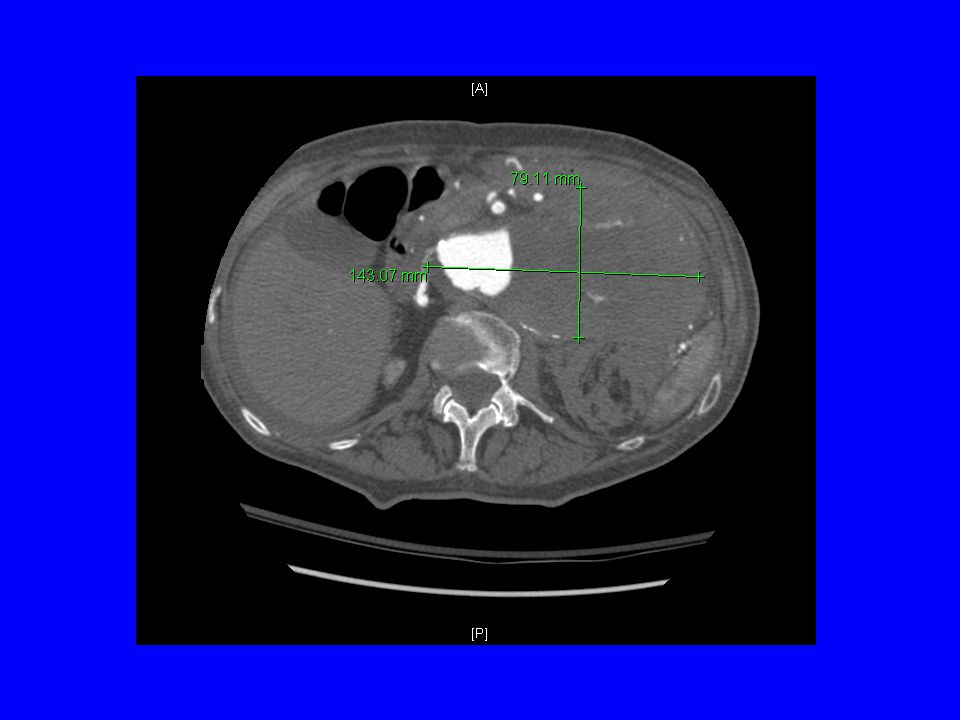
14 x 8 cm abdominal aortic aneurysm arising from the supraceliac aorta and extending to just above the take off of the left renal artery is visualized with extensive thrombus but also extensive flow

7
Diagnosis Clinical Presentation
RAAA is misdiagnosed 16% - 30% of the time Common misdiagnosis: Renal colic, perforated viscous, diverticulitis, gastrointestinal hemorrhage and ischemic bowel Mortality rates for correctly diagnosed was 58%, and 44% for misdiagnosed Likely due to fact that less severe ruptures have a more subtle presentation and can survive longer before going to OR

8
Diagnosis Imaging Plain Films Abdominal U/S Abdominal CT
Enlarged outline of calcified aortic wall A retrospective review showed that 65% of x-rays form RAAA had calcified aortic wall Loss of psoas shadow Abdominal U/S Sensitive in detecting aneurysm but not in detecting rupture Abdominal CT Most accurate method See presence of retroperitoneal blood (77% sensitive and 100% specific)
")
9
Enlarged outline of calcified aortic wall
Loss of psoas shadow Enlarged outline of calcified aortic wall

10
Sensitive in detecting aneurysm but not in detecting rupture

11
See presence of retroperitoneal blood
See presence of retroperitoneal blood. Here there is not a large retroperitoneal hematoma, but stranding of blood into surrounding tissues

12
Resuscitation If suspecting rAAA: Confirmed rAAA: 2 Large bore IVs
Type and Cross for at least 6 Units of pRBCs Confirmed rAAA: Transfer to Operating room (transfer to center with experienced surgeons prepared for rAAA) Establish art line and foley Prep and drape before and during anesthetic induction
 Establish art line and foley. Prep and drape before and during anesthetic induction.")
13
Resuscitation Actual Pre-Op resuscitation Controversial
Aggressive crystalloid can elevate BP and cause rupture of temporary aortic seal that forms after initial rupture Minimally resuscitate to “maintain conconsciousness” (~80 systolic) and use blood No randomized trials testing the different degrees of resuscitation with rAAA Animal studies show increased mortality when resuscitation occurs before control of hemorrhage
 and use blood. No randomized trials testing the different degrees of resuscitation with rAAA. Animal studies show increased mortality when resuscitation occurs before control of hemorrhage.")
14
Surgery OPEN TRANSPERITONEAL OPEN RETROPERITONEAL ENDOVASCULAR

15
Surgery Open Repair Hypotension No Hypotension
Inspect Retroperitoneum Reflect bowel and duodenum Supraceliac Clamp Pararenal Extensive Hematoma No Hematoma Careful Dissection for Infrarenal Control Uncontrolled Bleeding Develops

16
Surgery Open Repair TRANSPERITONEAL
Transperitoneal allows the fastest and easiest approach for Supraceliac clamp Retract the left lobe of the liver to right to show supraceliac aorta at diaphragm NG tube identifies esophagus and proximal stomach and retracts to the left Enter lesser sac by opening gastrohepatic omentum Aorta is found between crura of diaphragm and is clamped Can reposition clamp to infrarenal neck of aneurysm once aneurysm is opened or can make first anastamosis in aneurysm sac and then transfer clamp to graft to reperfuse kidneys and viscera.

17
Enter lesser sac by opening gastrohepatic omentum
Retract the left lobe of the liver to right to show supraceliac aorta at diaphragm NG tube identifies esophagus and proximal stomach and retracts to the left Enter lesser sac by opening gastrohepatic omentum

18
Sometimes crura may need to be split with electrocautery for appropriate visualization

19
Aorta is found between crura of diaphragm and is clamped

20
Surgery Open Repair TRANSPERITONEAL
Supraceliac Clamp Coordinate with anesthesia after clamp “crank up” the resuscitation before releasing supraceliac clamp prepare for hypotension Advantages quick solution to severe hypotension from intraperitioneal rupture. avoids injury to renal and gonadal vein injury from blind dissection of infrarenal neck Disadvantage ischemic injury injury to liver, bowel, and kidneys

21
Surgery Open Repair RETROPERITONEAL
ESPECIALLY for pararenal or suprarenal RAAA 10th interspace incision 1) Left colon mobilized to incise lateral peritoneal attachments. 2) Colon, pancreas, spleen, and kidney are elevated access diaphragmatic crura. 3) Divide crura access entire intra-abdominal aorta and visceral and renal vessels 4) May need a thoracoabdominal incision, or extra thoracic incision for the larger people, or the hostile abdomen
 Left colon mobilized to incise lateral peritoneal attachments. 2) Colon, pancreas, spleen, and kidney are elevated access diaphragmatic crura. 3) Divide crura access entire intra-abdominal aorta and visceral and renal vessels. 4) May need a thoracoabdominal incision, or extra thoracic incision for the larger people, or the hostile abdomen.")
22
Surgery Open Repair Extras
Brachial/femoral cut-down for occlusive balloon into aorta Aortic compressor to supraceliac aorta if rapid control needed before establishing exposure for clamp Aortocaval fistula direct digital pressure above and below the fistula and suture of the fistula from within the sac If iliac aneurysms are present leave alone unless ruptured, if so repair easiest first (allow for pelvic reperfusion) Use cellsaver, its use is justified if anticipate large blood loss
 Use cellsaver, its use is justified if anticipate large blood loss.")
23
Aortic compressor to supraceliac aorta if rapid control needed before establishing exposure for clamp

24
Surgery Open Repair Anatomic abnormalities
Venous anomalies that can cause bleeeding during clamping: Retroaortic renal vein Circumaortic renal vein Left-sided vena cava Duplicate inferior vena cava Horseshoe kidney If at neck of aneurysm it prevents adequate exposure (another reason to perform supraceliac clamping) Isthmus often contains renal tissue, collecting system and blood supply If known before surgery, retroperitoneal approach
 Isthmus often contains renal tissue, collecting system and blood supply. If known before surgery, retroperitoneal approach.")
25
Surgery Open Repair Closing
25%-30% cases, the abdomen cannot be closed without significant tension from swollen bowel or retroperitoneal hematoma Abdominal compartment syndrome (ACS) is bladder presser > 30cm H2O or 25mm Hg Use early mesh to reduce incidence of multi organ failure from ACS Especially with pre-op anemia, prolonged shock, pre-op cardiac shock, pre-op cardiac arrest, massive resuscitation, profound hypothermia, or severe acidosis Use nonabsorbable mesh covered with plolyurethane Early mesh closure vs takeback mesh resulted in 6% and 40% colon ischemia respectively
 is bladder presser > 30cm H2O or 25mm Hg. Use early mesh to reduce incidence of multi organ failure from ACS. Especially with pre-op anemia, prolonged shock, pre-op cardiac shock, pre-op cardiac arrest, massive resuscitation, profound hypothermia, or severe acidosis. Use nonabsorbable mesh covered with plolyurethane. Early mesh closure vs takeback mesh resulted in 6% and 40% colon ischemia respectively.")
26
Surgery Endovascular Repair
Institution requirements: 1) Rapid CT scanning For neck diameter, angulation, and iliac size Only about 20-46% of rAAA are suitable for EVAR 2) Training 3) Devices 4) Suite for Endovascular procedure
 Rapid CT scanning. For neck diameter, angulation, and iliac size. Only about 20-46% of rAAA are suitable for EVAR. 2) Training. 3) Devices. 4) Suite for Endovascular procedure.")
27
Surgery Endovascular Repair
Stratagies for Repair: Aorto-unifemoral graft ipisalateral internal iliac exclusion and a femorofemoral crossover graft (Montefiore group) Modular aortouniiliac and aortobiiliac Now rupture kits for repair
 Modular aortouniiliac and aortobiiliac. Now rupture kits for repair.")
28
Aorto-unifemoral graft
Endovascular Grafts and Other Image-Guided Catheter-Based Adjuncts to Improve the Treatment of Ruptured Aortoiliac AneurysmsTakao Ohki and Frank J. VeithAnn Surg October; 232(4): 466–479.
: 466–479.")
29
Modular aortouniiliac and aortobiiliac
Early Experience with the Talent™ Stent-Graft System for Endoluminal Repair of Abdominal Aortic AneurysmsFrank J. Criado, MD, Eric P. Wilson, MD, Eric Wellons, MD, Omran Abul-Khoudoud, MD, and Hari Gnanasekeram, MD Tex Heart Inst J. 2000; 27(2): 128–135.
: 128–135.")
30
Surgery Endovascular Repair
Anesthesia Can use local (unless patients are squirming) Don’t loose the sympathetic tone that can maintain pressure Some start under local and convert to general for positioning and release of graft
 Don’t loose the sympathetic tone that can maintain pressure. Some start under local and convert to general for positioning and release of graft.")
31
Surgery Endovascular Repair
Mortality Rates 10% to 45%, but limited numbers of patients Causes Colon ischemia MOF Continued hemorrage Endoleaks are a much bigger problem in this setting as hemorrhage isn’t controlled

32
RAAA RE-EVALUATED (no.)
Table Reported Data on Ruptured Abdominal Aortic Aneurysms (RAAA) Treated by Endovascular Aneurysm Repair FIRST AUTHOR RAAA RE-EVALUATED (no.) EVAR COMPLETED (%) EVAR MORTALITY (%) CONVERSION RATE (%) Ohki, 25 100 10 20 Hinchliffe, 20019 85 45 15 Lachat, 57 37 9.5 Orend, 21 71 14 29 Resch, 19 Scharrer-Pamler, 24 12.5 4 Peppelenbosch, 40 65 Reichart, 23 17 Totals 219 18 8.5
 Treated by Endovascular Aneurysm Repair. FIRST AUTHOR. RAAA RE-EVALUATED (no.) EVAR COMPLETED (%) EVAR MORTALITY (%) CONVERSION RATE (%) Ohki, Hinchliffe, Lachat, Orend, Resch, Scharrer-Pamler, Peppelenbosch, Reichart, Totals")
33
Complications Local Postoperative bleeding related to coagulapathy from hypothermia (12%-14%) Limb ischemia embolization from aortic debris, or clot formed in illiacs if retrograde flushing is not performed Colonic ischemia (3%-13%) leads to mortality in 73%-100% of time Degree and duration of hypotension Patency of IMA Collateral supply Site of hematoma Spinal Cord Injury: incidence 2.3%. Interuption of pelvic blood supply, prolonged aortic cross-clamping, introperative hypotension, aortic embolization, internal iliac interuption
 leads to mortality in 73%-100% of time. Degree and duration of hypotension. Patency of IMA. Collateral supply. Site of hematoma. Spinal Cord Injury: incidence 2.3%. Interuption of pelvic blood supply, prolonged aortic cross-clamping, introperative hypotension, aortic embolization, internal iliac interuption.")
34
Complications Systemic
Respiratory Failure 26-47% (mortality up to 68%) High O2 requirements, increased lung permeability, decrease in lung compliance Factors that predispose Large shifts in fluid and blood Pre-existing pulmonary dysfunction Long cross-clamp time Renal Dysfunction Incidence is 26-42% in patients in symptomatic aneurysms or rAAA Higher with suprarenal cross-clamp, longer duration of cross-clamp, pre-existing renal dysfunction, shock, old age
 High O2 requirements, increased lung permeability, decrease in lung compliance. Factors that predispose. Large shifts in fluid and blood. Pre-existing pulmonary dysfunction. Long cross-clamp time. Renal Dysfunction Incidence is 26-42% in patients in symptomatic aneurysms or rAAA. Higher with suprarenal cross-clamp, longer duration of cross-clamp, pre-existing renal dysfunction, shock, old age.")
35
Complications Systemic
Irreversible Shock 10-15% of rAAA mortality Irreversible state in which aortic clamping, aggressive fluid resuscitation, and inotropic support can fail to reverse hypotension Cardiac Complications MI – mortality of 19-66% Arrhythmias – mortality 46% Cardiac arrest – mortality % CHF – mortality of 41% Common as patients usually have simultaneous cardiac dz

36
Complications Systemic
Liver Failure Due to hypoxic injury Although the liver is robust; can deal with a large degree of hypoxic injury it still must reabsorb hematoma and the increase in metabolism that is required to do this Patients usually develop jaundice on day 7 Multisystem Organ Failure Incidence of 64% Most common cause of death after 48 hrs Also referred to as a systemic inflammatory syndrome

37
Complications Systemic
Multisystem Organ Failure “Two hit” hypothesis 1) Hemorrhagic shock – first ischemic insult primes the inflammatory response 2) Aortic Clamping – second ischemic insult 3) Resuscitation – first reperfusion insult 4) Aortic unClamping – second reperfusion insult Animal models support PMNs primed by pre-op hemorrhage, and after operative repair there was further activation with elevations of oxidative burst. These patients are walking into the hospital with oxidative injury
 Hemorrhagic shock – first ischemic insult primes the inflammatory response. 2) Aortic Clamping – second ischemic insult. 3) Resuscitation – first reperfusion insult. 4) Aortic unClamping – second reperfusion insult. Animal models support. PMNs primed by pre-op hemorrhage, and after operative repair there was further activation with elevations of oxidative burst. These patients are walking into the hospital with oxidative injury.")
38
Mortality Between 43% to 70% depending on the study Predictors
Scoring systems POSSUM – 12 physiologic variables and 6 operative variables for calculated risk Hardman index – Based on age, creatinine, hemoglobin, EKG evidence of ischemia, h/o loss of consciousness Multiple Organ dysfunction score (based on respiratory, renal, hepatic, hematologic, neurologic, and cardiac) Deaths bimodal Those that died 48 after repair had sig increases in MODS Renal failure followed by hepatic failure at Day 10 are at highest risk for mortality
 Deaths bimodal. Those that died 48 after repair had sig increases in MODS. Renal failure followed by hepatic failure at Day 10 are at highest risk for mortality.")
39
PROBABILITY OF SURVIVAL (%)
Table Logistic Regression Model Showing the Interaction of Significant Preoperative and Intraoperative Variables That Predicted Early Survival After Ruptured Abdominal Aortic Aneurysm Repair CREATININE (mg/dL) CLAMP SITE URINE OUTPUT (mL) PROBABILITY OF SURVIVAL (%) ≤1.3 Infrarenal ≥200 90 1-199 76 >1.3 71 Suprarenal 65 52 46 39 33 23 18 15 6
 CLAMP SITE. URINE OUTPUT (mL) PROBABILITY OF SURVIVAL (%) ≤1.3. Infrarenal. ≥ > Suprarenal")
40
MYOCARDIAL INFARCTION PROBABILITY OF SURVIVAL (%)
Logistic Regression Model Showing the Interaction of Significant Postoperative Complications That Predicted Early Survival After Ruptured Abdominal Aortic Aneurysm MYOCARDIAL INFARCTION RESPIRATORY FAILURE COAGULOPATHY RENAL DYSFUNCTION PROBABILITY OF SURVIVAL (%) No 96 Yes 91 74 66 ↑Cr 58 49 48 21 20 15 Dialysis 11 8 2 1 Cr, creatinine. Modified from Johnston KW: Ruptured abdominal aortic aneurysm: Six-year follow-up results of a multicenter prospective study. Canadian Society for Vascular Surgery Aneurysm Study Group. J Vasc Surg 19:888, 1994. page 1486 page 1487
 No. 96. Yes ↑Cr Dialysis Cr, creatinine. Modified from Johnston KW: Ruptured abdominal aortic aneurysm: Six-year follow-up results of a multicenter prospective study. Canadian Society for Vascular Surgery Aneurysm Study Group. J Vasc Surg 19:888, page page")
41
Conclusions Diagnosis – Have RAAA on the differential, don’t miss the diagnosis Resuscitation – Less is more until aorta is clamped Surgery – Quick, safe exposure. Use a method that you are experienced with. Complications – Expect them

42
I would like to end with one more aorta…
mine

44
If substantial hematoma prevents distal dissection use occlusive balloons placed from inside the aneurysm

45
Surgery Open Repair TRANSPERITONEAL
Hypotention Supraceliac Clamp If no hypotension Inspect Retroperitoneum Reflect bowel and duodenum Pararenal Extensive Hematoma SupraceliacClamp If no hematoma Careful Dissection for Infrarenal Control Uncontrolled Bleeding Developes SupraceliacClamp

46
She was evaluated for an intra-abdominal process because of abdominal pain. The patient was signed out to me by Dr. Lynn at the end of his shift. The patient suddenly called out to the nurse and was noted to be unresponsive. She was breathing shallow. I was called to the bedside. The patient appeared pale to me with pale conjunctivae. She was breathing shallow. Pulse oximetry was 100%. She had a paced rhythm of about 60. Blood pressure was 175/64. Her abdomen was mildly distended but otherwise soft. Because of the patient's shallow breathing and her low cognitive function, I immediately obtained an Accu-Chek, which was I was concerned about anemia, but the hemoglobin was 10. On the other hand, while we were assessing her, I got a call from the radiologist, who reported that the patient had a ruptured AAA. Advance directives did not show any DNR status. The patient was immediately updated to room 5 for resuscitation. Vascular Surgery was called and immediately came down. We were giving the patient oxygen, attempting a central line placement. O negative blood was ordered. The patient, however, was taken immediately up to a waiting operating room by the vascular surgeons. Transfer nurse helped take the patient up. Oxygen was given 100%.

Similar presentations

 Practice Group Logo here.>")



 Division of Thoracic Surgery May 28, 2009.>")














