Download presentation
Presentation is loading. Please wait.

1
TUBERCULOSIS

3
WHAT IS IT ? Bacterial infection
Caused by Mycobacterium tuberculosis (also called tubercle bacillus) Damages a person’s lungs or other parts of the body Fatal if not treated properly
 Damages a person’s lungs or other parts of. the body. Fatal if not treated properly.")
4
Mycobacterium – Slender, aerobic rods
Gram +ve, Acid fast M.tuberculosis – Reservoir- Humans M.bovis –Reservoir – contaminated milk M.Avium intracellulare-opportunistic (AIDS)
")
5
TB flourishes in Poverty, Over crowding, Malnutrition DM, CRF Alcoholism Immunosuppression

6
TRANSMISSION Spreads through the air when a
person with active TB (Inhalation) Coughs Speaks Laughs Sneezes Ingestion
 Coughs. Speaks. Laughs. Sneezes. Ingestion.")
7
SPREAD OF TB Local Spread Lymphatic spread Haematogenous Spread
Natural passages – Pleurisy, Peritonitis (salpingitis), Laryngitis , Ileocaecal
, Laryngitis , Ileocaecal.")
8
PATHOGENESIS Breath in infected air and bacilli go to lungs through bronchioles Bacilli infect alveoli Macrophages attack bacteria, but some survive Infected macrophages separate and form tubercles

9
Hypersensitivity to tubercular antigens
Cell Mediated immunity Caseating granulomas, Cavitation

10
Host response to lipids such as Mycosides
(cord factor) & glycolipids ( Wax-D) on the bacterial cell wall Type IV Hypersensitivity
 & glycolipids ( Wax-D) on the. bacterial cell wall. Type IV Hypersensitivity.")
11
Primary cells infected
are MACROPHAGES

12
ACTIVE INFECTION Unhealthy person Bacilli overwhelm immune system
Bacilli break out of tubercles in alveoli and spread through bloodstream

13
LATENT INFECTION Initial infection controlled by immune system
Bacilli remain confined in tubercles for years

14
DIAGNOSIS Mantoux test Medical history, x-rays, and smears for
AFB, Sputum culture, PCR

16
SYMPTOMS Perpetual Cough Fever Weight loss Night sweats
Loss of appetite Fatigue Swollen glands Pain while breathing

19
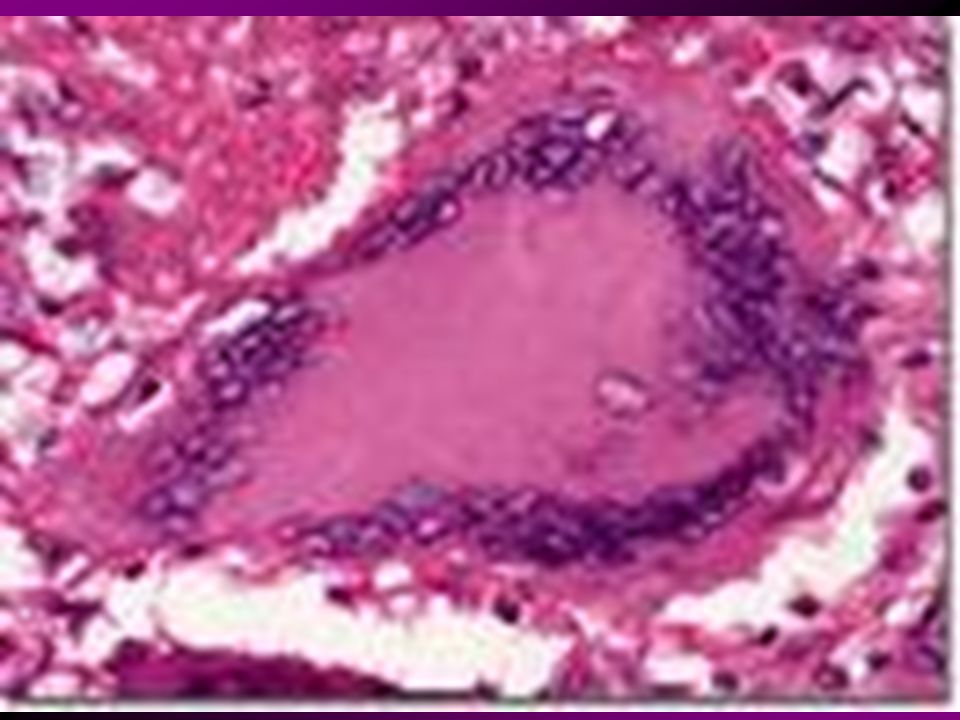
EVOLUTION OF TUBERCLE ( Granuloma)
PMN Macrophages Poorly degradable bacilli CD4+ T cells ( IFN, TNF) Epithelioid cells Hard Tubercle Soft Tubercle
 Epithelioid cells. Hard Tubercle. Soft Tubercle.")
20
GRANULOMA Central caseous necrosis surrounded by
epithelioid cells, Langhan’s giant cells, Rim of lymphocytes and fibroblasts.

26
FATE OF GRANULOMA Cold Abscess Sinus Formation Fibrosis Dystrophic calcification

27
CLINICAL SPECTRUM Secondary – Previously sensitized person
Primary – previously unexposed, unsensitized person Secondary – Previously sensitized person - Follows primary, - Reactivation of dormant lesion, - Exogenous reinfection ( Large inoculum of virulent bacilli)
")
29
Primary tuberculosis GHON’S COMPLEX( Primary complex)
Ghon’s Focus- Subpleural focus in the upper part of lower lobe/ lower part of upper lobe Lymphatic component Lymph node component – Hilar & Tracheo-bronchial

32
Fate of Primary TB Fibrosis, calcification Progressive Pulmonary TB
Primary Miliary TB Secondary TB

33
Secondary Tuberculosis
Initially -- small focus (2 cm) of consolidation in the apical pleura Develop a small area of caseation, fibrosis
 of. consolidation in the apical pleura. Develop a small area of caseation, fibrosis.")
35
Fate of secondary TB Heal with fibrosis Fibrocavitary TB Pneumonia Miliary TB

36
Progressive Pulmonary TB
Child, Elderly, Immunocompromised Erosion of blood vessels hemoptysis Erosion into bronchus Empyema, effusion, pleuritis

38
MILIARY TUBERCULOSIS Miliary = ‘millet seeds’ Spread thro’ lymphatics Lesions- small / microscopic Liver, Spleen, Kidney, Brain, Bonemarrow adrenals, fallopian tubes, epididymis, etc.

42
Isolated organ TB: Meningitis Renal Osteomyelitis Adrenals Salpingitis
Pott’s spine Lymphadenitis- Scrofula Intestinal

43
IMMUNIZATION Bacilli Calmette Guerin ( BCG) [ Attenuated Strains of Bovine type of Bacilli]
![IMMUNIZATION Bacilli Calmette Guerin ( BCG) [ Attenuated Strains of Bovine type of Bacilli]](http://slideplayer.com/slide/244670/1/images/43/IMMUNIZATION+Bacilli+Calmette+Guerin+%28+BCG%29+%5B+Attenuated+Strains+of+Bovine+type+of+Bacilli%5D.jpg "IMMUNIZATION Bacilli Calmette Guerin ( BCG) [ Attenuated Strains of Bovine type of Bacilli]")
44
THANK YOU

Similar presentations


















 INFLAMMATION>")


 Environmental.>")











 Gram (+) rod (bacilli). Acid-fast Pulmonary.>")

Caused by Mycobacterium.>")