Download presentation
Presentation is loading. Please wait.

1
Family Medicine Potpourri Some of the topics selected by editors of Journal Watch as top stories of 2013

2
Preview Mental Health – Varenicline safe and effective in mentally ill – Acupuncture and folic acid effective for depression General Medicine – JNC8 has arrived – New lipid guidelines controversy Women’s health – New early pregnancy loss guidelines – Poor vaccination rates for HPV Pediatrics – New guidelines on sinusitis – New guidelines on starting foods in infants

3
Preview Mental Health –V–Varenicline safe and effective in mentally ill –A–Acupuncture and folic acid effective for depression General Medicine –J–JNC8 has arrived –N–New lipid guidelines controversy Women’s health –N–New early pregnancy loss guidelines –P–Poor vaccination rates for HPV Pediatrics –N–New guidelines on sinusitis –N–New guidelines on starting foods in infants

4
Mental Health- Varenicline safety Varenicline Black Box Warning from FDA 2009 Neuropsychiatric Symptoms and Suicidality monitor for serious neuropsychiatric events incl. behavior change, hostility, agitation, depression, and suicidality as well as worsening of preexisting psychiatric illness which have occurred in pts taking varenicline and after discontinuation; some cases possibly complicated by nicotine withdrawal sx, but also reported in pts who continue to smoke while taking varenicline; weigh varenicline risks vs. benefits of smoking cessation (Am J Psychiatry 2013; 170:1460–1467)
.")
5
Mental Health- Varenicline safety Methods: NIMH funded metanalysis, two data sources – 8027 from Pfizer’s 17 placebo controlled RCTs – DOD database 35800 Results – In the randomized controlled trials, varenicline increased the risk of nausea (odds ratio=3.69, 95% CI=3.03–4.48) but not rates of suicidal events, depression, or aggression/agitation. It significantly increased the abstinence rate, by 124% compared with placebo and 22% compared with bupropion. Having a current or past psychiatric illness increased the risk of neuropsychiatric events equally in treated and placebo patients. (Am J Psychiatry 2013; 170:1460–1467)
.")
6
Mental Health- Varenicline safety – In the DOD study, after propensity score matching, the overall rate of neuropsychiatric disorders was significantlly lower for varenicline than for nicotine replacement therapy (2.28% compared with 3.16%). (Am J Psychiatry 2013; 170:1460–1467)
.")
7
Mental Health- Varenicline safety (Am J Psychiatry 2013; 170:1460–1467)
")
8
Mental Health- Acupuncture for depression Methods: Government funded “pragmatic” RCT – 755 adults from primary care randomized to usual care v 12 weeks of usual care plus ’humanistic counseling’ v 12 weeks acupuncture plus usual care – Moderate to severe depression at baseline (BDI-II of 20) and followed with PHQ-9 at 3 month intervals PLoS Med 10(9): e1001518. doi:10.1371/journal.pmed.1001518

9
Mental Health- Acupuncture for depression Results – Compared to usual care, there was a statistically significant reduction in mean PHQ-9 depression scores at 3 months for acupuncture (22.46, 95% CI 23.72 to 21.21) and counselling (21.73, 95% CI 23.00 to 20.45), and over 12 months for acupuncture (21.55, 95% CI 22.41 to 20.70) and counselling (21.50, 95% CI 22.43 to 20.58) PLoS Med 10(9): e1001518. doi:10.1371/journal.pmed.1001518

10
Mental Health- Acupuncture for depression PLoS Med 10(9): e1001518. doi:10.1371/journal.pmed.1001518

11
Preview Mental Health –V–Varenicline safe and effective in mentally ill –A–Acupuncture and folic acid effective for depression General Medicine –J–JNC8 has arrived –N–New lipid guidelines controversy Women’s health –N–New early pregnancy loss guidelines –P–Poor vaccination rates for HPV Pediatrics –N–New guidelines on sinusitis –N–New guidelines on starting foods in infants

12
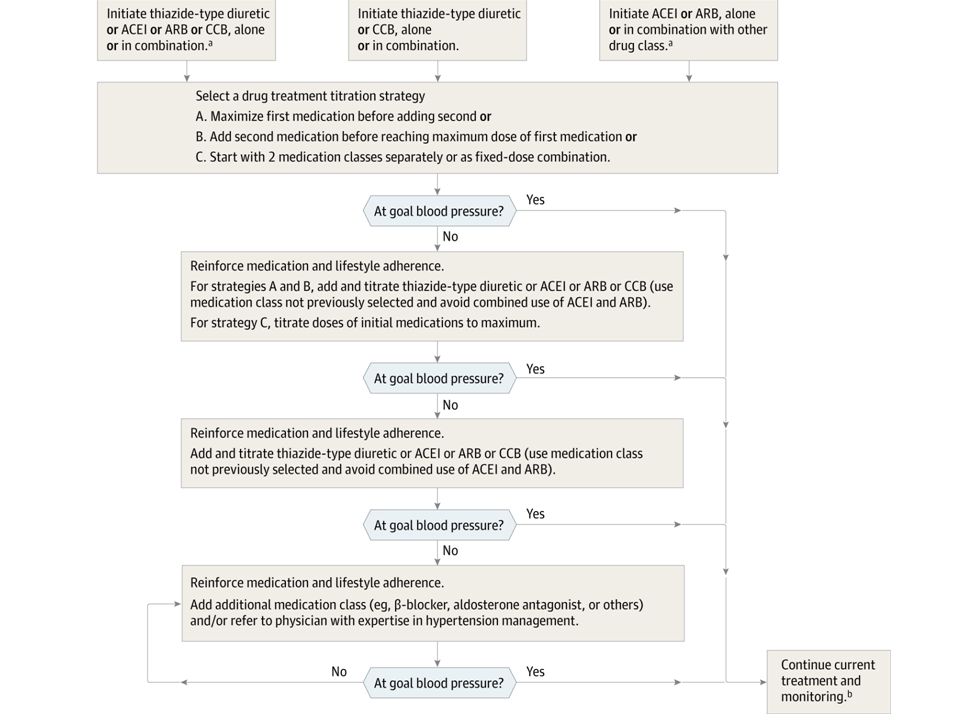
JNC8 What’s Changed – JNC 7 said 140/90 across the board; JNC 8 says 150/90 at 60 plus. – Diabetics/ CKD have same treatment goal in JNC 8 (was 130/80 in JNC 7) – Thiazides were first line in 7; now you can choose from any of four classes for nonblacks (ACE, CCB, thiazide, ARB) and two classes for blacks (thiazide or CCB). – Not BB as less protection against stroke December 18, 2013. doi:10.1001/jama.2013.284427
 – Thiazides were first line in 7; now you can choose from any of four classes for nonblacks (ACE, CCB, thiazide, ARB) and two classes for blacks (thiazide or CCB). – Not BB as less protection against stroke December 18, doi: /jama")
13
JNC8 Recommendation 1 – In the general population aged ≥60 years, initiate pharmacologic treatment to lower blood pressure (BP) at systolic blood pressure (SBP) ≥150 mm Hg or diastolic blood pressure (DBP) ≥90 mm Hg and treat to a goal SBP <150 mm Hg and goal DBP <90 mm Hg. (Strong Recommendation – Grade A) Corollary Recommendation – In the general population aged ≥60 years, if pharmacologic treatment for high BP results in lower achieved SBP (eg, <140 mm Hg) and treatment is well tolerated and without adverse effects on health or quality of life, treatment does not need to be adjusted. (Expert Opinion – Grade E) Recommendation 2 – In the general population <60 years, initiate pharmacologic treatment to lower BP at DBP ≥90 mm Hg and treat to a goal DBP <90 mm Hg. (For ages 30- 59 years, Strong Recommendation – Grade A; For ages 18-29 years, Expert Opinion – Grade E)
 Corollary Recommendation – In the general population aged ≥60 years, if pharmacologic treatment for high BP results in lower achieved SBP (eg, <140 mm Hg) and treatment is well tolerated and without adverse effects on health or quality of life, treatment does not need to be adjusted. (Expert Opinion – Grade E) Recommendation 2 – In the general population <60 years, initiate pharmacologic treatment to lower BP at DBP ≥90 mm Hg and treat to a goal DBP <90 mm Hg. (For ages years, Strong Recommendation – Grade A; For ages years, Expert Opinion – Grade E).")
14
JNC8 Recommendation 3 – In the general population <60 years, initiate pharmacologic treatment to lower BP at SBP ≥140 mm Hg and treat to a goal SBP <140 mm Hg. (Expert Opinion – Grade E) Recommendation 4 – In the population aged ≥18 years with chronic kidney disease (CKD), initiate pharmacologic treatment to lower BP at SBP ≥140 mm Hg or DBP ≥90 mm Hg and treat to goal SBP <140 mm Hg and goal DBP <90 mm Hg. (Expert Opinion – Grade E) Recommendation 5 – In the population aged ≥18 years with diabetes, initiate pharmacologic treatment to lower BP at SBP ≥140 mm Hg or DBP ≥90 mm Hg and treat to a goal SBP <140 mm Hg and goal DBP <90 mm Hg. (Expert Opinion – Grade E)
 Recommendation 4 – In the population aged ≥18 years with chronic kidney disease (CKD), initiate pharmacologic treatment to lower BP at SBP ≥140 mm Hg or DBP ≥90 mm Hg and treat to goal SBP <140 mm Hg and goal DBP <90 mm Hg. (Expert Opinion – Grade E) Recommendation 5 – In the population aged ≥18 years with diabetes, initiate pharmacologic treatment to lower BP at SBP ≥140 mm Hg or DBP ≥90 mm Hg and treat to a goal SBP <140 mm Hg and goal DBP <90 mm Hg. (Expert Opinion – Grade E).")
15
JNC8 Recommendation 6 – In the general nonblack population, including those with diabetes, initial antihypertensive treatment should include a thiazide-type diuretic, calcium channel blocker (CCB), angiotensin-converting enzyme inhibitor (ACEI), or angiotensin receptor blocker (ARB). (Moderate Recommendation – Grade B) Recommendation 7 – In the general black population, including those with diabetes, initial antihypertensive treatment should include a thiazide-type diuretic or CCB. (For general black population: Moderate Recommendation – Grade B; for black patients with diabetes: Weak Recommendation – Grade C) Recommendation 8 – In the population aged ≥18 years with CKD, initial (or add-on) antihypertensive treatment should include an ACEI or ARB to improve kidney outcomes. This applies to all CKD patients with hypertension regardless of race or diabetes status. (Moderate Recommendation – Grade B)
 Recommendation 7 – In the general black population, including those with diabetes, initial antihypertensive treatment should include a thiazide-type diuretic or CCB. (For general black population: Moderate Recommendation – Grade B; for black patients with diabetes: Weak Recommendation – Grade C) Recommendation 8 – In the population aged ≥18 years with CKD, initial (or add-on) antihypertensive treatment should include an ACEI or ARB to improve kidney outcomes. This applies to all CKD patients with hypertension regardless of race or diabetes status. (Moderate Recommendation – Grade B).")
16
JNC8 Recommendation 9 – The main objective of hypertension treatment is to attain and maintain goal BP. If goal BP is not reached within a month of treatment, increase the dose of the initial drug or add a second drug from one of the classes in recommendation 6 (thiazide-type diuretic, CCB, ACEI, or ARB). The clinician should continue to assess BP and adjust the treatment regimen until goal BP is reached. If goal BP cannot be reached with 2 drugs, add and titrate a third drug from the list provided. Do not use an ACEI and an ARB together in the same patient. If goal BP cannot be reached using only the drugs in recommendation 6 because of a contraindication or the need to use more than 3 drugs to reach goal BP, antihypertensive drugs from other classes can be used. Referral to a hypertension specialist may be indicated for patients in whom goal BP cannot be attained using the above strategy or for the management of complicated patients for whom additional clinical consultation is needed. (Expert Opinion – Grade E)
. The clinician should continue to assess BP and adjust the treatment regimen until goal BP is reached. If goal BP cannot be reached with 2 drugs, add and titrate a third drug from the list provided. Do not use an ACEI and an ARB together in the same patient. If goal BP cannot be reached using only the drugs in recommendation 6 because of a contraindication or the need to use more than 3 drugs to reach goal BP, antihypertensive drugs from other classes can be used. Referral to a hypertension specialist may be indicated for patients in whom goal BP cannot be attained using the above strategy or for the management of complicated patients for whom additional clinical consultation is needed. (Expert Opinion – Grade E).")
20
New Lipid Guideline New Pooled Cohort Equations for atherosclerotic cardiovascular disease (ASCVD) risk assessment – Stroke now included in ASCVD risk assessment, in addition to myocardial infarction (MI) – Separate equations for nonwhite populations No LDL-C or non-HDL-C treatment targets Four groups for statin therapy (see below) Cred johns hopkins this slide
 risk assessment – Stroke now included in ASCVD risk assessment, in addition to myocardial infarction (MI) – Separate equations for nonwhite populations No LDL-C or non-HDL-C treatment targets Four groups for statin therapy (see below) Cred johns hopkins this slide")
21
New Lipid Guideline – Patients with clinical atherosclerotic cardiovascular disease (ASCVD) should receive high-intensity (age, <75) or moderate-intensity (age, ≥75) statin therapy. – Patients with LDL cholesterol levels ≥190 mg/dL should receive high-intensity statin therapy. – Diabetic patients aged 40–75 with LDL cholesterol levels of 70–189 mg/dL and without clinical ASCVD should receive at least moderate-intensity statin therapy (and possibly high-intensity statin therapy when estimated 10-year ASCVD risk is ≥7.5%). – Patients without clinical ASCVD or diabetes but with LDL cholesterol levels of 70–189 mg/dL and estimated 10-year ASCVD risk ≥7.5% should receive moderate- or high- intensity statin therapy. Stone NJ et al. J Am Coll Cardiol 2013 Nov 12.
. – Patients without clinical ASCVD or diabetes but with LDL cholesterol levels of 70–189 mg/dL and estimated 10-year ASCVD risk ≥7.5% should receive moderate- or high- intensity statin therapy. Stone NJ et al. J Am Coll Cardiol 2013 Nov 12..")
22
Pooled Cohort Equations for Risk Assessment Equations predict 10-year risk of stroke & myocardial infarction – Former guidelines focused only on heart attacks – Highlights the large burden of disability from nonfatal events Separate equations for nonwhite populations – Importance of race/ethnicity in risk of ASCVD Cred Johns Hopkins this slide

24
Preview Mental Health –V–Varenicline safe and effective in mentally ill –A–Acupuncture and folic acid effective for depression General Medicine –J–JNC8 has arrived –N–New lipid guidelines controversy Women’s health –N–New early pregnancy loss guidelines –P–Poor vaccination rates for HPV Pediatrics –N–New guidelines on sinusitis –N–New guidelines on starting foods in infants

25
Early Pregnancy Loss Guidelines Four possibilities when faced with a patient with pain and bleeding in first trimester – Currently viable IUP – Failed or failing IUP – Ectopic Pregnancy Unless situation is life-threatening, question becomes: “Is there a chance of a viable pregnancy?” Doubilet PM et al. N Engl J Med 2013 Oct 10.

26
Early Pregnancy Loss Guidelines Authors felt that most important is to not falsely diagnose a pregnancy as nonviable (false positive rate for nonviable pregnancy of zero, or specifity of 100%) – Risk of damaging viable IUP usually outweigh risks of watchful waiting in stable monitored patient. Doubilet PM et al. N Engl J Med 2013 Oct 10.

27
Early Pregnancy Loss Guidelines These guidelines offer more stringent rules on ruling out viable pregnancy than in the past Fluid in the uterus is most likely a GS when using TV-US Doubilet PM et al. N Engl J Med 2013 Oct 10.

28
Early Pregnancy Loss Guidelines Two basic branches of evaluation – IUP visualized but viability uncertain – Pregnancy of unknown location Doubilet PM et al. N Engl J Med 2013 Oct 10.

29
Early Pregnancy Loss Guidelines IUP visualized but viability uncertain. Confirm nonviable If: Embryonic crown-rump length ≥7 mm and no heartbeat. Mean gestational sac diameter ≥25 mm and no embryo present. No embryo with heartbeat ≥2 weeks after TVUS showed a gestational sac without a yolk sac. No embryo with heartbeat ≥11 days after TVUS showed a gestational sac with a yolk sac. Doubilet PM et al. N Engl J Med 2013 Oct 10.

30
Figure 1. Early Intrauterine Gestational Sac. A transvaginal ultrasonogram obtained at 5 weeks of gestation (Panel A) shows a small, round, fluid-filled structure (arrow), which was confirmed to be an early intrauterine pregnancy 4 weeks later (Panel B) on a follow-up scan showing a fetus measuring 19.1 mm, corresponding to approximately 9 weeks of gestational age. Plus signs indicate calipers.
 shows a small, round, fluid-filled structure (arrow), which was confirmed to be an early intrauterine pregnancy 4 weeks later (Panel B) on a follow-up scan showing a fetus measuring 19.1 mm, corresponding to approximately 9 weeks of gestational age. Plus signs indicate calipers..")
31
Figure 2. Definite Pregnancy Failure Diagnosed in Three Women by Means of Transvaginal Ultrasonography. Panel A shows an embryo with a crown–rump length (between the plus signs, indicating calipers) of 7.1 mm. No cardiac activity was seen on real-time ultrasonography. Panels B and C show a gestational sac with a mean diameter of 27.7 mm (average of 35.4 mm, 19.7 mm, and 28.1 mm), with no visible embryo. SAG denotes sagittal view, and COR coronal view. Panel D shows an intrauterine gestational sac with a yolk sac, and Panel E (a scan obtained 2 weeks later) shows a yolk sac but no embryo within the gestational sac.
 of 7.1 mm. No cardiac activity was seen on real-time ultrasonography. Panels B and C show a gestational sac with a mean diameter of 27.7 mm (average of 35.4 mm, 19.7 mm, and 28.1 mm), with no visible embryo. SAG denotes sagittal view, and COR coronal view. Panel D shows an intrauterine gestational sac with a yolk sac, and Panel E (a scan obtained 2 weeks later) shows a yolk sac but no embryo within the gestational sac..")
32
Early Pregnancy Loss Guidelines Pregnancy of unknown location. – A single hCG assessment, regardless of level, does not reliably determine a pregnancy's location or viability (this is because hCG levels in women with nonviable IUPs, viable IUPs, and EPs overlap substantially). – A single hCG level <3000 mIU/mL should not elicit treatment for presumed EP. – A single hCG ≥3000 mIU/mL indicates that viable IUP is possible but unlikely. At least one additional hCG level should be measured before initiating treatment for EP. Doubilet PM et al. N Engl J Med 2013 Oct 10.
. – A single hCG level <3000 mIU/mL should not elicit treatment for presumed EP. – A single hCG ≥3000 mIU/mL indicates that viable IUP is possible but unlikely. At least one additional hCG level should be measured before initiating treatment for EP. Doubilet PM et al. N Engl J Med 2013 Oct 10..")
33
HPV Vaccination Rates Crumby Only 32% of adolescent girls (13-17 yoa) have received all three doses Lowest in those who live in southeast and uninsured; no difference across ethnicities Can do with religious beliefs and perception that vaccine will encourage promiscuity Certain HPV related cancers are on the rise (anus, oropharynx) Jemal A et al. J Natl Cancer Inst 2013 Jan 7. Brisson M et al. J Natl Cancer Inst 2013 Jan 7. - See more at: http://www.jwatch.org/wh2013013100000 02/2013/01/31/hpv-vaccination-just-do- it#sthash.dXekJe4e.dpuf

35
Preview Mental Health –V–Varenicline safe and effective in mentally ill –A–Acupuncture and folic acid effective for depression General Medicine –J–JNC8 has arrived –N–New lipid guidelines controversy Women’s health –N–New early pregnancy loss guidelines –P–Poor vaccination rates for HPV Pediatrics –N–New guidelines on sinusitis –N–New guidelines on starting foods in infants

36
Acute Bacterial Sinusitis in kids AAP Update(last 2001) Clinicians should make a presumptive diagnosis of acute bacterial sinusitis when a child with an acute URI presents with the following: – Persistent illness, ie, nasal discharge (of any quality) or daytime cough or both lasting more than 10 days without improvement; OR – Worsening course, ie, worsening or new onset of nasal discharge, daytime cough, or fever after initial improvement; OR – Severe onset, ie, concurrent fever (temperature ≥39°C/102.2°F) and purulent nasal discharge for at least 3 consecutive days (Evidence Quality: B; Recommendation). No IMAGING unless you suspect orbital or CNS involvement Wald ER et al. Pediatrics 2013 Jul. Smith MJ. Pediatrics 2013 Jul. - See more at: http://www.jwatch.org/na31073/2013/07/ 12/acute-bacterial-sinusitis- children#sthash.9LnCD5pu.dpuf

37
Acute Bacterial Sinusitis in kids AAP Update(last 2001) Treatment indicated if severe onset or worsening course criteria met. ‘Consider’ treatment if just persistent (abx v watchful waiting for three days) Amoxicillin at 45 mg/kg day for about 10 days (7 days after symptom free). Can use amox- clav 80-90 mg/kg/day if concerned about resistance or in severe illness/ younger patient Wald ER et al. Pediatrics 2013 Jul. Smith MJ. Pediatrics 2013 Jul. - See more at: http://www.jwatch.org/na31073/2013/07/ 12/acute-bacterial-sinusitis- children#sthash.9LnCD5pu.dpuf
 Amoxicillin at 45 mg/kg day for about 10 days (7 days after symptom free). Can use amox- clav mg/kg/day if concerned about resistance or in severe illness/ younger patient Wald ER et al. Pediatrics 2013 Jul. Smith MJ. Pediatrics 2013 Jul. - See more at: 12/acute-bacterial-sinusitis- children#sthash.9LnCD5pu.dpuf.")
38
Acute Bacterial Sinusitis in kids AAP Update(last 2001) Should improve within 72 hours, reassess if not or if worsen Wald ER et al. Pediatrics 2013 Jul. Smith MJ. Pediatrics 2013 Jul. - See more at: http://www.jwatch.org/na31073/2013/07/ 12/acute-bacterial-sinusitis- children#sthash.9LnCD5pu.dpuf

39
When and what to start feeding your baby?! The American Academy of Allergy, Asthma & Immunology (AAAAI) – Jan 2013 – Avoidance of allergenic foods during lactation is not recommended. – Avoidance of allergenic foods (except peanuts) during pregnancy is not recommended. Data are inconclusive on peanut ingestion during pregnancy and development of peanut allergy. This choice is left for parents to decide. Fleischer DM et al. J Allergy Clin Immunol In Pract 2013 Jan
 – Jan 2013 – Avoidance of allergenic foods during lactation is not recommended. – Avoidance of allergenic foods (except peanuts) during pregnancy is not recommended. Data are inconclusive on peanut ingestion during pregnancy and development of peanut allergy. This choice is left for parents to decide. Fleischer DM et al. J Allergy Clin Immunol In Pract 2013 Jan.")
40
When and what to start feeding your baby?! – Exclusive breast-feeding is recommended for the first 4 months of life, and breast-feeding ideally should continue through the first year. When breast-feeding is not possible in high-risk children, consider a partial whey hydrolysate formula or extensively hydrolyzed formula. Soy formula has no advantage over milk-based formula for prevention of allergy. – Complementary foods can be introduced between ages 4 and 6 months. Fleischer DM et al. J Allergy Clin Immunol In Pract 2013 Jan

41
When and what to start feeding your baby?! – Highly allergenic foods can be started in small doses at home once other foods such as grains and vegetables are tolerated. New foods can be tried every few days. Early introduction may actually reduce food allergy. – Acidic foods such as berries, tomato, and citrus can cause local irritant reactions but rarely cause systemic reactions and do not need to be delayed. – Routine allergy testing is not recommended prior to initiation of foods. Allergy consultation might be warranted in infants with severe eczema or history of adverse food reactions. Fleischer DM et al. J Allergy Clin Immunol In Pract 2013 Jan

42
When and what to start feeding your baby?! – A child with a sibling with peanut allergy has a 7% risk for peanut allergy. Allergy consultation can be considered for such children, although typically the slow introduction of peanut at home is safe. An initial fatal peanut reaction in an infant has never been reported. Fleischer DM et al. J Allergy Clin Immunol In Pract 2013 Jan

Similar presentations


















 Trial>")




