Download presentation
Presentation is loading. Please wait.

1
Geriatric Delirium: Impact of National Guidelines and Interactive Educational Modules
Dr. Peter Chan, MD, FRCPC Consult-Liaison and Geriatric Psychiatrist, Vancouver General Hospital. Clinical Associate Professor, UBC Dept. of Psychiatry

2
Collaborators UBC Care for Elders Module
Dr. Martha Donnelly, MD, FRCPC Dr. Ram Randhawa, MD, FRCPC VGH Nursing Education Module (VCHA) Ms. Wendy Marr, RN Ms. Maureen Shaw, RN, MN
 Ms. Wendy Marr, RN. Ms. Maureen Shaw, RN, MN.")
3
Disclosure Honouraria for speaker engagements: Astra-Zeneca Eli-Lilly
Janssen-Ortho

4
Guidelines: Categories of Evidence:
Ia Evidence from meta-analysis of randomized controlled trials Ib Evidence from at least one randomized controlled trial IIa Evidence from at least one controlled study without randomization IIb Evidence from at least one other type of quasi-experimental study III Evidence from non-experimental descriptive studies, such as comparative studies, correlation studies and case-control studies IV Evidence from expert committees reports or opinions and/or clinical experience of respected authorities Shekelle et al 1999

5
Guidelines: Strength of Recommendation
A Directly based on category I evidence B Directly based on category II evidence or extrapolated recommendation from category I evidence C Directly based on category III evidence or extrapolated recommendation from category I or II evidence D Directly based on category IV evidence or extrapolated recommendation from category I, II, or III evidence Shekelle et al 1999

6
What’s in the Guideline
Background Prevention Detection, Assessment, Diagnosis & Monitoring Management Legal and Ethical Issues Education Systems of Care Research on Delirium Future Considerations

7
Canadian Coalition For Senior’s Mental Health: Practice Guidelines

8
Predisposing Factors Inouye, SK et al
Predisposing Factors Inouye, SK et al. A predictive model for delirium in hospitalized elderly medical patients based on admission characteristics. Ann Intern Med 1993; 119: cognitive impairment sleep deprivation immobility visual impairment hearing impairment dehydration

9
Screening Under-recognition, esp. in those:
Over 80 y.o. with hypoactive delirium with visual impairment and/or pre-existing dementia Inouye et al. Arch Int. Med 2001 No reliable screening tool to differentiate delirium and dementia Practically, acute-onset and/or fluctuation in cognition/function/abnormal behaviours Others signs New onset aphasia or dysarthria New onset or worsening incontinence

10
Confusion Assessment Method (Inouye et al. Ann.Int.Med. Dec.15/90)
acute onset and fluctuation AND inattention AND disorganized thinking OR altered level of consciousness excellent sensitivity, good specificity

11
Screening Instruments
We recommend… The Confusion Assessment Method is recommended for screening on acute medical/surgical wards and in the ER (C) CIWA-Ar is recommended for monitoring symptoms of alcohol withdrawal (C)
 CIWA-Ar is recommended for monitoring symptoms of alcohol withdrawal (C)")
12
Precipitating Factors in Hospital Inouye and Charpentier, JAMA 1996; 275: 852-57
Physical restraints (RR=4.4) Malnutrition (RR=4.0) More than 3 medications added (RR=2.9) Use of bladder catheter (RR=2.4) Any iatrogenic event (RR=1.9)
 Malnutrition (RR=4.0) More than 3 medications added (RR=2.9) Use of bladder catheter (RR=2.4) Any iatrogenic event (RR=1.9)")
13
Use of Restraints We recommend…
Physical restraints for geriatric patients suffering from delirium should be applied only in exceptional circumstances when: (D) a) There is a serious risk for bodily harm to self or others OR b) Other means for controlling behaviours leading to harm have been explored first, including pharmacologic treatments, but were ineffective AND c) The potential benefits outweigh the potential risks of restraints
 a) There is a serious risk for bodily harm to self or others OR. b) Other means for controlling behaviours leading to harm have been explored first, including pharmacologic treatments, but were ineffective AND. c) The potential benefits outweigh the potential risks of restraints.")
14
Pharmacologic Management
We recommend… Psychotropic medications should be reserved for older persons with delirium that are in distress due to agitation or psychotic symptoms, in order to carry out essential investigations or treatment, and to prevent older delirious persons from endangering themselves or others. (D) In the absence of psychotic symptoms causing distress to the patient, treatment of hypoactive delirium with psychotropic medications is not recommended (D) The use of psychotropic medications for the specific purpose of controlling wandering in delirium is not recommended (D)
 In the absence of psychotic symptoms causing distress to the patient, treatment of hypoactive delirium with psychotropic medications is not recommended (D) The use of psychotropic medications for the specific purpose of controlling wandering in delirium is not recommended (D)")
15
Pharmacologic Management
We recommend… Antipsychotics are the treatment of choice to manage the symptoms of delirium (with the exception of alcohol or benzodiazepine withdrawal delirium). (B) Haloperidol is suggested as the antipsychotic of choice based on the best available evidence to date. (B) Initial dosages are in the range of 0.25 mg- 0.5 mg. Od-bid (D) Atypical antipsychotics may be considered as alternative agents as they have lower rates of extra-pyramidal signs. (B) Benztropine should not be used prophylactically with haloperidol in the treatment of delirium. (D)
. (B) Haloperidol is suggested as the antipsychotic of choice based on the best available evidence to date. (B) Initial dosages are in the range of 0.25 mg- 0.5 mg. Od-bid (D) Atypical antipsychotics may be considered as alternative agents as they have lower rates of extra-pyramidal signs. (B) Benztropine should not be used prophylactically with haloperidol in the treatment of delirium. (D)")
16
Pharmacologic Management
We recommend… In older persons with delirium who also have Parkinson’s Disease or Lewy Body Dementia, atypical antipsychotics are preferred over typical antipsychotics. (D) Sedative-hypnotic agents are recommended as the primary agents for managing alcohol withdrawal delirium (B). Their use in other forms of delirium should be avoided (D).
 Sedative-hypnotic agents are recommended as the primary agents for managing alcohol withdrawal delirium (B). Their use in other forms of delirium should be avoided (D).")
17
Pharmacologic Management: Guidelines
Frequency: Regular vs. Prn; nighttime dosing Dosages: haloperidol bid (watch QTc) risperidone initiated at 0.25 mg od-bid olanzapine at mg per day quetiapine at mg per day
 risperidone initiated at 0.25 mg od-bid. olanzapine at mg per day. quetiapine at mg per day.")
18
Haloperidol in Delirium Management
“Evidence” based on 1 RCT (Breitbart 1996) AIDS Dementia population Comparator to atypicals (3 RCT’s in Cochrane) Prolonged QTc, especially I.V.– baseline ECG Risk of Extrapyramidal Symptoms, esp. elderly >4.5 mg/day in Cochrane Review
 AIDS Dementia population. Comparator to atypicals (3 RCT’s in Cochrane) Prolonged QTc, especially I.V.– baseline ECG. Risk of Extrapyramidal Symptoms, esp. elderly. >4.5 mg/day in Cochrane Review.")
19
Loxapine in Delirium Management
Conventional antipsychotic with atypical properties Singh et al Journal of Psychiatry and Neuroscience, 21:29-35 Mid-potency in D2 receptor blockade Effect on D1, D4, 5-HT2, NMDA receptors Parenteral IM/SC (IV in monitored setting) Widespread use in Vancouver Over 3500 VGH inpatients with Delirium since 1989 Use in all settings, including CCU, CSICU, ICU, ACE units Dosing mg/d (B.I.D. dosing at 1600h and 2000h)
 Widespread use in Vancouver. Over 3500 VGH inpatients with Delirium since Use in all settings, including CCU, CSICU, ICU, ACE units. Dosing mg/d (B.I.D. dosing at 1600h and 2000h)")
20
Subsequent Considerations
Risks of Atypical Antipsychotics Mortality CVA or related events Metabolic syndrome (less likely if short duration) Use of Cholinesterase Inhibitors Treatment of Hypoactive Delirium
 Use of Cholinesterase Inhibitors. Treatment of Hypoactive Delirium.")
21
Summary of Key Points in Managing Geriatric Delirium
Screening is important in identifying cases. Haloperidol is recommended based on available evidence, but atypicals are alternatives, esp. in those sensitive. Loxapine a viable alternative. The elderly can have prolonged delirium, and slower to recover in cognition and function when delirium has cleared.

22
Guideline and Literature Review
American Psychiatric Association. Practice guideline for the treatment of patients with delirium British Geriatrics Society. Guidelines for the diagnosis and management of delirium in the elderly Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adult. Crit Care Med 2002;30(3): Management of alcohol withdrawal delirium: an evidence-based guideline. Arch Intern Med 2004;164(13): Iowa Veterans Affairs Nursing Research Consortium. Research-based protocol: acute confusion/delirium. Iowa City, Iowa: The University of Iowa Gerontological Nursing Interventions Research Centre: Research Dissemination Core; 1998. Screening for delirium, dementia and depression in older adults. Toronto (ON): Registered Nurses Association of Ontario; 2003. Caregiving strategies for older adults with delirium, dementia and depression. Toronto (ON): Registered Nurses Association of Ontario; 2004. Sharon Inouye. Delirium in Older Persons. NEJM 354: March 16, 2006 Number 11 Gregory Fricchione. Postoperative Delirium. Am J Psychiatry 165: , July 2008
: Management of alcohol withdrawal delirium: an evidence-based guideline. Arch Intern Med 2004;164(13): Iowa Veterans Affairs Nursing Research Consortium. Research-based protocol: acute confusion/delirium. Iowa City, Iowa: The University of Iowa Gerontological Nursing Interventions Research Centre: Research Dissemination Core; Screening for delirium, dementia and depression in older adults. Toronto (ON): Registered Nurses Association of Ontario; Caregiving strategies for older adults with delirium, dementia and depression. Toronto (ON): Registered Nurses Association of Ontario; Sharon Inouye. Delirium in Older Persons. NEJM 354: March 16, 2006 Number 11. Gregory Fricchione. Postoperative Delirium. Am J Psychiatry 165: , July")
23
Web Resources Care for Elders Interactive Delirium Module
UBC Division of Geriatric Psychiatry VIHA Delirium information Virginia Case Study

24
A Quality Improvement Project
M. McKnight, H. Nagi, K. Ng, C. Reid, P. Tam Sponsored by Dr. A. Hill and Dr. P. Lee

25
Delirium Working Group
Collaboration of experts at VGH and the region, established Nov 2006 Why: Problem of idiosyncratic & disparate patterns of practice Mission: Use literature & expert opinion to establish best practice Standardize approach to patient care Implement best practice through PPOs and staff education Nurses Psychiatrists & Geri-psychiatrists General Surgeons Intensivists Geriatricians & Internists

27
1 1

28
2 2

29
3 3

30
PRISME: Maureen Shaw, RN, MN
P - PAIN R- RESTRAINT, RETENTION I - INFECTION S - SENSORY IMPAIRMENT, SLEEPLESSNESS M - MEDICATION, METABOLIC E - ENVIRONMENT, EMOTIONS

32
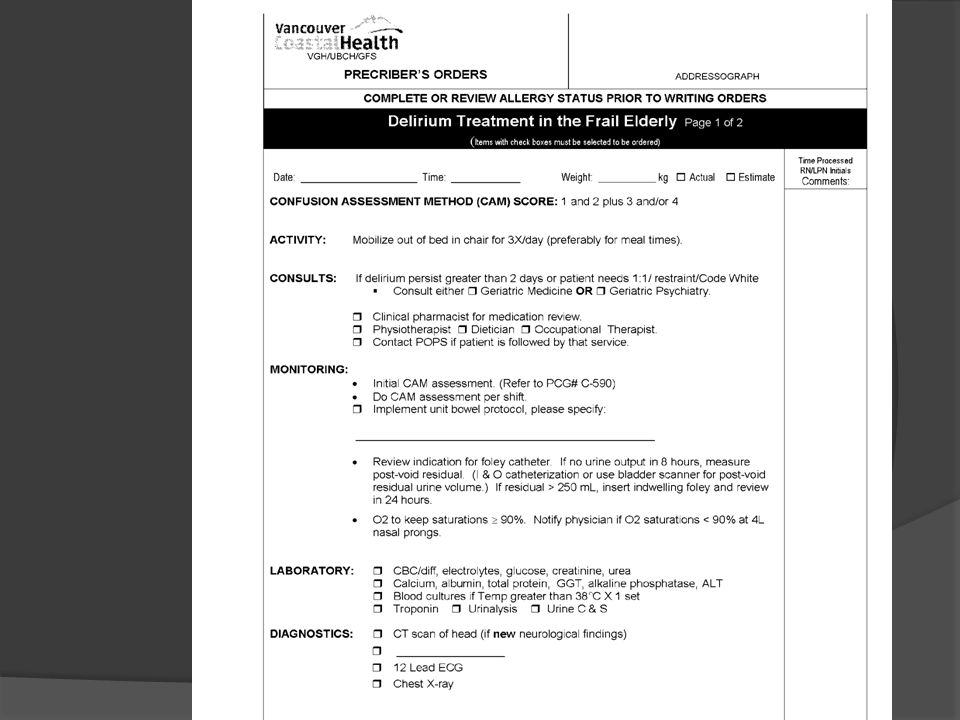
PPO: Pg 1

33
PPO: Pg 1

34
PPO: Pg 2

35
PPO: Pg 2

Similar presentations










 January 21, 2014 Delirium and Dementia.>")









