Download presentation
Presentation is loading. Please wait.

1
Dr Mark Cook Consultant Haematologist University Hospital Birmingham

2
Demonstrate there is a role for allogeneic stem cell transplant in myeloma and evaluate some of the composite elements of the transplant process Review the evidence to understand the current state of play Discuss how allogeneic transplant needs to evolve to be more commonly considered as an option

4
IMW 2011 Paris The Haematologist Who Suggested Allogeneic Transplant is Useful in Myeloma

5
Data on allograft in myeloma is generally a dog’s breakfast

7
Inter-trial comparison is understandably fraught with difficulties, but is generally all we have

8
Data on allograft in myeloma is generally a dog’s breakfast Inter-trial comparison is understandably fraught with difficulties, but is generally all we have Opinion is just that- an individual’s perspective on the data betrays their underlying instincts and biases

10
Tricot et al Blood 1996

11
Perez-Simon, BJH, 2003, 121; 104-8

12
Copyright ©2005 American Society of Hematology. Copyright restrictions may apply. Crawley, C. et al. Blood 2005;105:4532-4539 Figure 4. Overall survival with respect to the presence of chronic graft-versus-host disease

13
Copyright ©2005 American Society of Hematology. Copyright restrictions may apply. Crawley, C. et al. Blood 2005;105:4532-4539 Effect of alemtuzumab on progression

14
. Corradini P et al. Blood 2003;102:1927-1929 ©2003 by American Society of Hematology

15
Thus graft versus myeloma is evidenced by: Response to DLI Link with GVHD (esp chronic GVHD) Increased relapse with T-cell depletion And If you can get a deep response, you can get a durable response So why is use not more widespread? Age Comorbidities Performance status

16
Years 026 13 45 Probability of Survival, % HLA-matched sibling, Allo (N=878) autologous transplant (N=22,254) Unrelated, Allo (N=143) 0 20 40 60 80 100 10 30 50 70 90 0 20 40 60 80 100 10 30 50 70 90 P < 0.0001 68% 47% 28%
 autologous transplant (N=22,254) Unrelated, Allo (N=143) P < % 47% 28%")
17
The lure of GvM raises the prospect of cure TRM rates decreasing Prospects are better of post-transplant options

18
Kumar et al Blood 2011

20
Roos-Weil et al Haematologica 2011

21
Nishihori et al Cancer Control 2011

22
Presented by Giralt IMW 2011

23
Roos-Weil et al Haematologica 2011

24
Lokhorst et al Blood 2004

27
. El-Cheikh J et al. Haematologica 2008;93:455-458 ©2008 by Ferrata Storti Foundation

28
Kroger et al Blood 2004

29
13/24 patients given pre-emptive DLI after partial T-depleted allograft 4/13 developed GVHD grade II or above Levenga et al Bone Marrow transplant 2007

30
38 patients treated with RIC allo (2Gy TBI) 2-6 months post auto Lenalidomide 10mg daily for 21/28 days started 1-6 months post transplant 14 patients (47% of those evaluable) stopped lenalidomide by the end of the 2 nd cycle, primarily due to GVHD
 2-6 months post auto Lenalidomide 10mg daily for 21/28 days started 1-6 months post transplant 14 patients (47% of those evaluable) stopped lenalidomide by the end of the 2 nd cycle, primarily due to GVHD")
31
Utilising the following: RIC approach rather than myeloablative to increase the potential treatment population and reduce toxicity Combined Auto- RIC allo to optimise pre allo disease status If T-depleting, then a strategy to minimise risk of relapse post-transplant Pre-emptive DLI

32
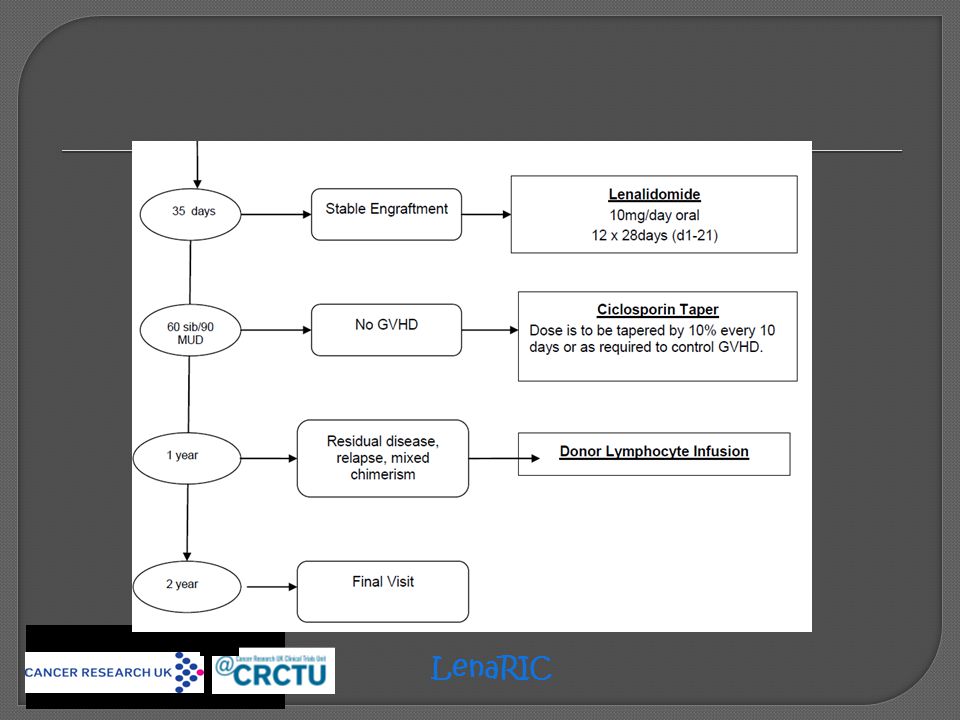
LenaRIC

34
Primary endpoint: Progression free survival at 2 years post-transplant Secondary endpoints: Donor engraftment Day +100 and 1 year post-transplant non-relapse mortality Graft versus host disease Disease free survival at 1 and 2 years post-transplant Overall survival at 1 and 2 years post-transplant Exploratory endpoints: Immune reconstitution samples NK receptor genetics and transplant outcome Flow cytometry assessment for minimal residual disease LenaRIC

35
(1) use a prior debulky autologous Transplantation (2) limit the procedure to patients with sensitive disease (3) use the best conditioning with fludarabine/melphalan or low-dose TBI with or without fludarabine and with no T- cell depletion (4) optimize DLI (ie, with low-dose thalidomide) for suboptimal responses
 use a prior debulky autologous Transplantation (2) limit the procedure to patients with sensitive disease (3) use the best conditioning with fludarabine/melphalan or low-dose TBI with or without fludarabine and with no T- cell depletion (4) optimize DLI (ie, with low-dose thalidomide) for suboptimal responses")
36
Presented by Einsele IMW 2011

37
Clarify the group that will benefit

38
Overhaul conditioning

39
Radioimmunotherapy (RIT) with anti-CD66 promising in autologous transplant ?potential role in allogeneic transplant Buchmann et al Eur J Nucl Med Mol Imaging 2009
 with anti-CD66 promising in autologous transplant potential role in allogeneic transplant Buchmann et al Eur J Nucl Med Mol Imaging 2009")
40
Clarify the group that will benefit Overhaul conditioning Look at the graft

41
Gabriel et al Blood 2010Benson et al prePub Blood October 2011

42
Towards Personalised Medicine Population Efficacy – Toxicity + Efficacy – Toxicity - Efficacy + Toxicity + Efficacy + Toxicity - Treatment e.g. Transplant

43
To conclude: Whilst trying to ignore my own biases, allografting offers the prospect of cure/long-term immune mediated control However, effective delivery remains hampered by toxicity which is especially high in the non- myeloablative context RIC allografting reduces toxicity but thereby diminishes efficacy The challenge is to transform how RIC allos are delivered, to reduce toxicity further and to increase efficacy There remain opportunities in the peri and post transplant period to effect further progress

Similar presentations







 patients Policy.>")






 Chemoimmunotherapy and Maintenance Lenalidomide in Relapsed/Refractory (R/R) Chronic Lymphocytic Leukemia (CLL) and Small.>")







![5-Azacitidine For Myelodysplasia Before Allogeneic Hematopoietic Cell Transplantation Field T et al. Bone Marrow Transplant 2009:[Epub ahead of print].](/33/8174862/big_thumb.jpg "5-Azacitidine For Myelodysplasia Before Allogeneic Hematopoietic Cell Transplantation Field T et al. Bone Marrow Transplant 2009:[Epub ahead of print].>")

