Download presentation
Presentation is loading. Please wait.

1
Case Examples – severe lower limb injuries
March 2014 Trauma Conference Andy Gray Newcastle Hospitals

2
Example 1 42 year old fit and well male
RTA – 28th March 2013 (1 year ago!) Transferred to RVI A,B,C normal. GCS 15 Pan CT scan – no significant injury to head, neck, thoracolumbar spine, chest, abdo etc
 Transferred to RVI. A,B,C normal. GCS 15. Pan CT scan – no significant injury to head, neck, thoracolumbar spine, chest, abdo etc.")
3
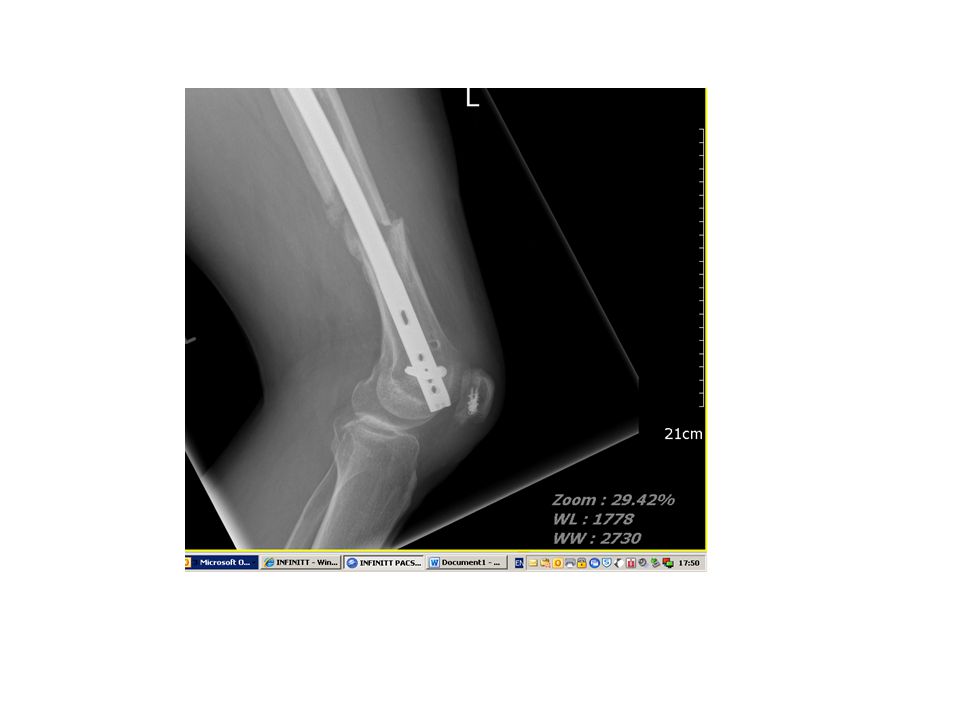
Secondary survey Bilateral distal femoral shaft fractures
Left thigh wound Both kneecaps damaged Classic ‘dashboard’ injury Hips and pelvis fine Arterial line being inserted into wrist during secondary survey Ortho trauma theatre free (consultant led) On call consultant going to fracture clinic
 On call consultant going to fracture clinic.")
4
Theatre Stable patient / base excess OK (no acidosis)
Debridement and irrigation of wound Bilateral retrograde nailing Left performed / supervised by consultant 1 Right performed by consultant 2 Transferred to ITU/HDU after surgery

6
Day 1 post op Left wrist pain Pins and needles median nerve
Going to theatre for 2nd debridement and DPC of open femur – plastics present Dislocated IP joint big toe

7
Additional surgery

10
ARDS / Fat embolus Syndrome
Aeitilogy after major trauma Haemodynamic (Crowel 2000) –occult hypovolaemia Embolic Coagulative Inflammatory Injury Severity Score Associated injuries (e.g. chest)
 –occult hypovolaemia. Embolic. Coagulative. Inflammatory. Injury Severity Score. Associated injuries (e.g. chest)")
11
Over next 2 weeks Recovered from ARDS Began rehab on ortho trauma ward
Repatriation to local DGH near Manchester

13
Transferred to hospital closer to home
As per national guidelines Case discussed with receiving team Good communication Patient spent 1 week in hospital before requesting re-transfer back to RVI

14
Issues Receiving unit critical of care received
No ownership of patient -no consultant review K wires removed from toe deformity recurred Critical of position of wrist plate Critical of missed screw “How old was your treating surgeon?” Worried and confused patient.

17
2 months after surgery – wound infection left anterior knee wound

18
Admitted – wound debridement and exchange nail

19
9 months after injury – femurs healed and doing well apart from toe!!

20
Issues for discussion Importance of repeating the secondary survey
Repatriation of patients In theory everybody agrees with this ? Dealing with complications ? Patients need secondary procedures Ownership of the patient Avoiding criticising treatment of patient ‘I would have managed this differently’

21
Case 2- 35 year old male / MBA / isolated lower limb injury / 22 stone

22
Spanning ex fix applied 2.5 weeks

23
Definitive fixation – 2 incisions

24
Infection / wound necrosis / plastics and salvage / rotational flap to distal tibia / free lat dorsi flap over knee

25
6 weeks later – lifted flap / bone graft / reattached extensor mechanism

27
Discussion points Expect the unexpected
Importance of having allied specialties (plastics/vascular) available on-site Development of a gold standard regional service for open fractures and complex lower limb reconstruction
 available on-site. Development of a gold standard regional service for open fractures and complex lower limb reconstruction.")
28
Thank-You

Similar presentations














Extension of traumatized wound to allow identification of zone of injury 2)Detection & removal of foreign material, especially.>")










