Download presentation
Presentation is loading. Please wait.

1
Using Hematology Instrument Data to Troubleshoot
MEDICAL MYSTERIES Using Hematology Instrument Data to Troubleshoot Typically, when you think of troubleshooting, you assume it means troubleshooting an instrument problem However, troubleshooting can also include using instrument data to “solve” an unusual patient case as well. DR PETER JOHN LOGA, PhD; MS; MSc; BSc; SDMLT; DMLT; FIBMS; FZIMLS

2
OBJECTIVES Review instrument technology; compare & contrast normal vs abnormal Apply this technology / knowledge to a variety of cases “SOLVE” the medical mystery In order to “troubleshoot”, it is extremely important to understand the instrument technology and differentiate normal from abnormal. Next we will apply this technology and newly learned knowledge to a variety of cases to “solve” the medical mystery.

4
PROVEN BECKMAN COULTER TECHNOLOGIES

5
The Coulter Principle Vacuum Aperture Current Pathway
Detail of Aperture Internal Electrode External Electrode Suspension of Cells External Housing (Aperture Bath) Aperture Aperture Housing
 Aperture. Aperture Housing.")
6
Aperture Impedance System System with Sweep Flow
Eliminates recirculation of cells Cells pushed away by diluent More accurate counts

7
Coincidence Correction
Electronic pulse-editing & coincidence correction: Provides accurate histograms and cell sizing for reliable RBC and PLT indices Pulse to be edited Diluent stream

8
Aperture Impedance System
Triplicate Counting Ensures Precision Reduces Repeats

9
The Coulter Principle A red cell passes through RBC aperture
Red Blood Cell Sensing Zone Oscilloscope

10
RBC HISTOGRAM This is an example of a NORMAL RBC histogram. Most RBCs fall between 80 and 100 fl. The histogram should start at the baseline on the left and a small “tail” may be evident on the right. This represents doublets and triplets (cells that go through the aperture in twos and threes). These are excluded from the RBC MCV by algorithms but may be seen on the histogram. NORMAL
. These are excluded from the RBC MCV by algorithms but may be seen on the histogram. NORMAL.")
11
RBC HISTOGRAM MACROCYTIC, TARGET CELLS, DI RBC COLD AGGLUTININ DI RBCs
These are a variety of examples of abnormal RBC histograms but certainly does not represent all the possibilities. Like the WBC histogram, RBCs do not always follow the “textbook” so some of the things represented here may look different with different specimens. DI RBCs Post Transfusion RBC FRAGMENTS, MICROCYTIC RBCs, Giant PLT

12
PLT HISTOGRAMS This is a NORMAL PLT histogram. The PLT histogram has two curves. One is the curve created from the directly measured PLT count and the other is Coulter’s patented curve fitting process which allows an accurate PLT count without interference from microcytic RBC or RBC fragments. NORMAL

13
PLT Curve Fitting The Curve Fitting Process Allows More Accurate Counts When Platelets of Larger Than 20 fL Are Present

14
PLT Counting & Sizing Coulter impedance counting has a PATENTED CURVE FITTING process that is used in conjunction with WBC histogram review for platelet clump and giant platelet flags

15
PLT HISTOGRAMS Giant Platelets Small Platelets
Here are a couple of examples of abnormal PLT histograms. One represents the presence of large or giant PLTs. Note how the directly measured curve (blue line) does not come back down to the baseline at 20 fl. The instrument then extrapolates this curve to eliminate any interference but account for the large or giant PLTs still out on the far right hand edge. The other histogram indicates a patient with small PLTs (small MPV). Note there is no need for the curve fitting process in this case as the PLTs all fall withing the directly measured region. Small Platelets
 does not come back down to the baseline at 20 fl. The instrument then extrapolates this curve to eliminate any interference but account for the large or giant PLTs still out on the far right hand edge. The other histogram indicates a patient with small PLTs (small MPV). Note there is no need for the curve fitting process in this case as the PLTs all fall withing the directly measured region. Small Platelets.")
16
The Coulter Principle A white cell passes through WBC aperture
Neutrophil Sensing Zone Oscilloscope

17
Coulter WBC Histogram Monos 90 -160 fL Neuts Lymphs 160 - 450 fL
Eos Baso What results is a histogram. This is an example of a NORMAL WBC histogram. The lymphocytes, being the smallest cell fall to the far left of the histogram. The lymphocytes are followed by the Basos, Monos Eos and Neutrophils. Have you ever wondered why basophils, which when you look through the microscope appear to be about the same size as a neutrophil or eo appear between the lymphs and monos?? Well…basophilic granules are water soluble and try as hard as we might to create the “perfect” isotonic solution, you still lose some of the granules when the basophils are put in solution. When this happens, the cell cytoplasm shrinks down around the nucleus and the few remaining granules and makes the cell appear smaller than it is in vivo.

18
WBC HISTOGRAMS ImmNE1 & ImmNE2 Lymphocytosis Variant Lymph ImmNE2
These are examples of other WBC histograms and the corresponding suspect flag. Keep in mind, these are examples of the most common scenarios and unfortunately, cells do not always follow the “textbook” so occasionally you may see a certain suspect flag and it may not be exactly the same as the examples noted here depending on what is going on with the patient. ImmNE2 Eosinophilia Blasts

19
WBC Interference Percentage of interference analyzed for statistical significance Flagging based on all three histograms instead of one Histogram positional parameters used for further definition Cellular Interference

20
AccuCount Technology LH700 Series WBC 0 – 400,000 RBC 0 – 8,000,000
HGB PLT 0 – 3,000,000 AccuCount WBC and AccuCount Plt Counts have been “validated” by Reference Flow Cytometry

21
Automated Differential Analysis
VCS TECHNOLOGY Automated Differential Analysis

22
Near Native WBC Analysis
Red Cells Removed From Sample Dilution Using a Lytic Process Second Agent Prevents Alteration of the White Cells Hydrodynamically Focused Flowcell Laminar Flow Ensures Single File Cell Passage Coincidence Effects Are Minimized

23
Flow Cytometry Technique for counting, examining and sorting microscopic particles suspended in a stream of fluid. It allows simultaneous multiparametric analysis of the physical and/or chemical characteristics of single cells flowing through a detection apparatus.

24
BioPhysical Flow Cytometry
SHEATH-FLUID IN SAMPLE IN FLOW CELL SAMPLE DILUTION SHEATH FLUID SENSING AREA Cells are hydrodynamically focused An electro-optical flow cytometer provides concurrent electronic and optical measurements

25
The Triple Transducer Module
RF Detector Pre-Amp Laser Lens Block Flow Cell LS Sensor Light Scatter Pre-Amp A major advance in technology An electro-optical flow cytometer Provides concurrent electronic and optical measurements

26
VCS Technology Volume Light Scatter Conductivity Total Cell Volume
Nuclear Volume Nuc/Cyto Ratio Cell Surface Characteristics Light Scatter Conductivity

27
The 3-D VCS Scatterplot NUCLEAR SHAPE AND COMPOSITION GRANULES
When you were in Med Tech school they taught you to look at certain things to help identify and classify a cell. You were taught to look at cells size, nuclear shape and composition and finally the cytoplasm shape and the presence or absence of granules. You put all of this information together to help identify a cell. Whether or not you realize it, your subconscious still goes through these steps every time you look through the microscope CYTOPLASM CELL SIZE

28
COULTER VCS TECHNOLOGY
VOLUME = SIZE CONDUCTIVITY = INTERNAL COMPOSITION LIGHT SCATTER = CELL SHAPE / SURFACE Like you do at the scope, the instrument uses this same basic concept to identify each cell but in a much more sophisticated and accurate manner.

29
VOLUME DC Measures Total Cell Volume Using the Reference Method of Direct Current Impedance Unaffected by cell orientation

30
CONDUCTIVITY RF Measures Internal Cell Structure Using Radiographic Imaging Similar to Ultrasound Conductivity Is a Proprietary Technology

31
LASER LIGHT SCATTER Light Scatter Measures Cell Surface Granularity Using a Broad Range of Angles. Over 60 angles of light scatter are analyzed.

32
3-D Cellular Analysis - VCS
VOLUME (Y) CONDUCTIVITY (Z) Lymphs Monos Basos Neuts Eos LIGHT SCATTER (X) The 3 probes (DC, RF and Scatter) interrogate each of the 8192 cells simultaneously. Three concurrent measurements are performed on each and every cell as it goes through the flow cell once cell at a time. The VOLUME of each cell is measured using a low radio frequency which surrounds the cell giving an accurate size. A CONDUCTIVITY measurement is performed using a high radiofrequency (RF). This RF penetrates the cell membrane and gives an accurate picture of the internal components. Finally, using LASER LIGHT SCATTER, over 60 angles of light scatter are analyzed for cell surface characteristics. All three of these measurements are being done simultaneously on EACH and EVERY one of the 8192 CELLS as it passes through the flow cell. These three measurements (volume, conductivity and scatter) obtained from each cell are then plotted on the X, Y and Z-axis in a 3 dimensional cube. This type of 3 dimensional diff technology allows for the DIRECT measurement of all five cell types. Not all vendors can make this claim. Every cell is treated in the same manner and each cell is given an X, Y, and Z coordinate on the dataplot; with 16 million points in the matrix. ALL cell populations are DIRECTLY measured
 CONDUCTIVITY (Z) Lymphs. Monos. Basos. Neuts. Eos. LIGHT SCATTER (X) The 3 probes (DC, RF and Scatter) interrogate. each of the 8192 cells simultaneously. Three concurrent measurements are performed on each and every cell as it goes through the flow cell once cell at a time. The VOLUME of each cell is measured using a low radio frequency which surrounds the cell giving an accurate size. A CONDUCTIVITY measurement is performed using a high radiofrequency (RF). This RF penetrates the cell membrane and gives an accurate picture of the internal components. Finally, using LASER LIGHT SCATTER, over 60 angles of light scatter are analyzed for cell surface characteristics. All three of these measurements are being done simultaneously on EACH and EVERY one of the 8192 CELLS as it passes through the flow cell. These three measurements (volume, conductivity and scatter) obtained from each cell are then plotted on the X, Y and Z-axis in a 3 dimensional cube. This type of 3 dimensional diff technology allows for the DIRECT measurement of all five cell types. Not all vendors can make this claim. Every cell is treated in the same manner and. each cell is given an X, Y, and Z coordinate on. the dataplot; with 16 million points in the matrix. ALL cell populations are DIRECTLY. measured.")
33
AccuGate Software Technology
Population Boundaries Curve Around Clusters Overlapping Clusters Are Separated Each Population Is Independently Categorized Rare Event Clusters Are Easily Identified Older samples more accurately evaluated

34
Better Abnormal Cell Detection
1 Mono-Blasts 2 Myelo-Blasts 3 Immature Granulocytes 4 Band Neutrophils 5 Lympho-Blasts 6 Variant Lymphocytes 7 Low Volume Lymphocytes 7a NRBCs 8 PLT Clumps 9 Giant Platelets 10 RBC Parasites (Malaria, etc) 1 2 3 4 5 6 7 7a 8 9 10
 a")
35
DIFF TECHNOLOGY Now that we have discussed normal and abnormal histograms, let’s talk about diff technology.

36
CONFUSED????

37
NORMAL This is an example of a normal CBC….no flags or abnormal histograms.

38
NORMAL Likewise, this is the normal differential results and scatterplot.

39
NRBC, PLT CLUMPS, GIANT PLT, MALARIAL PARASITES, DEBRIS, ETC
NORMAL DATAPLOT MONOCYTES NEUTROPHILS EOSINOPHILS V O L U M E In a normal data plot, these are the positions of the cell populations. BASOPHILS LYMPHOCYTES NRBC, PLT CLUMPS, GIANT PLT, MALARIAL PARASITES, DEBRIS, ETC C O N D U C T I V I T Y S C A T T E R

40
CUBE ROTATION RED = VOLUME = SIZE GREEN = SCATTER = SURFACE
CONDUCTIVITY SCATTER On the LH700 series of instruments, you can actually rotate the cube to look at the populations from different angles. This does prove very helpful at times when looking at unusual cell populations. VOLUME RED = VOLUME = SIZE GREEN = SCATTER = SURFACE BLUE = CONDUCTIVITY = INTERNAL SCATTER CONDUCTIVITY

41
LH 700 Series The “6-Part Diff”
NRBC enumeration automatic with differential Fully automated No reflex or repeat testing required No additional reagent packs required WBC count automatically corrected

42
Automatically Make Slide Message- Action To Be Taken
Decision Rules UNLIMITED RULES! 4 Rule Types And/Or Joins Automatically Make Slide Message- Action To Be Taken

43
Research Population Data (RPD)
When VCS 3D Dataplot is optimized; There is a change in the WBC Research Population Data This appears to correlate with the presence of abnormal cells in previously undiagnosed patients Here is a listing of published case studies that have shown there is a change in the WBC Research Population Data (described in most of the literature as WBC positional parameters) that appears to correlate with the presence of abnormal cells. See Reference List.
 that appears to correlate with the presence of abnormal cells. See Reference List.")
44
Research Population Data
Mean and SD are typically consistent from one normal population to the next

45
Research Population Data
NE1 The increasing SD corresponds to a more immature population of cells

46
Research Population Data (RPD)
WBC Research Population Data has been studied in the following clinical cases: CLL Left Shift Malaria Lymphoproliferative Disorders Myelodysplasia Sepsis

47
CLINICAL APPLICATION Steve Marionneaux Laboratory Manager
The Saint Vincent’s Comprehensive Cancer Center New York, New York

48
MYSTERY #1 Now let’s start putting our information to the test to see if we can use it to help solve some cases.

49
CBC Results 8 Year Old Female
This CBC is from an 8 year old female. Obviously, she has a low WBC and anemic with a slight elevation in her MCV. Her diff parameters appear “normal” for an 8 year old percentage wise but when considering the absolute value are actually elevated.

50
DataPlot Results The instrument gave a LY BLAST suspect flag and the LY% corresponds to the predominant Lymph population seen on the data plot. But WHY does the instrument suspect blasts?

51
MANUAL DIFF RESULTS MANUAL DIFF Seg = 20 Band = 2 Lymph = 51
Upon looking at her peripheral smear, it confirms the blast flag. MANUAL DIFF Seg = 20 Band = 2 Lymph = 51 Blast = 27

52
PRE-B CELL Acute Lymphoblastic Leukemia
Diff Cube Rotation VOLUME VOLUME From this angle, it does appear that there really are TWO different lymph populations which corresponds to the normal lymphs and blast cells. Flow cytometry confirms that this child has Pre B-Cell Acute Lymphoblastic Leukemia. The Lymphoblasts are one of the two populations seen on the dataplot. CONDUCTIVITY SCATTER SCATTER CONDUCTIVITY PRE-B CELL Acute Lymphoblastic Leukemia

53
PRECURSOR B-CELL ALL Low WBC, neutropenia Anemic
Mononuclear population with smooth chromatin CD34+, TdT+ population

54
MYSTERY #2 Now on to the next Mystery.

55
WBC &PLT HISTOGRAMS AUTODIFF RESULTS
With this case the WBC, AutoDiff and Dataplot appear quite normal. The WBC histogram shows a slightly elevated hump in the ImmNE2 region but the PLT histogram is normal.

56
RBC HISTOGRAM Suspect flags show Dimorphic RBCs with an H&H Check Fail but look at the RBC Histogram….does that look normal?

57
CBC / RBC RESULTS When you look at the RBC parameters, it is obviously a Cold Agglutinin with an RBC count that is not even compatible with life, a grossly elevated MCV and for the MCH and MCHC results. The agglutinated red cells are creating the bizarre RBC histogram. A useful key to solving for RBC agglutination is the “Research Button” on the far right hand edge of the patient screen. It is a useful tool in many instances and in this particular case told you it thought the RBCs were agglutinating.

58
MYSTERY #3 Mystery #6 coming up!

59
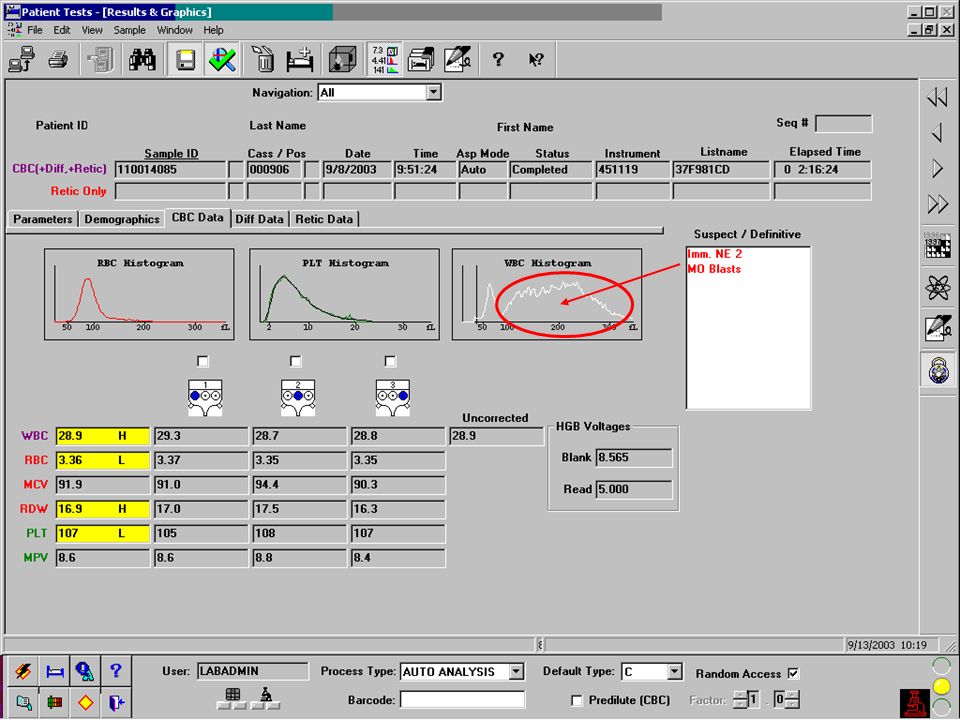
46 Year Old Female Immediately, it is obvious this patient has a serious problem. Her WBC is grossly elevated. She is also anemic, macrocytic and thrombocytopenic.

60
46 / Female When considering the Suspect Flags, the ImmNE2 flag corresponds to the enlarged end of the WBC histogram. Likewise, the Blast flag is being triggered by the large population on the mononuclear region of the histogram. The Verify Diff flag corresponds to the abnormal diff parameters possibly being triggered by the unusually increased monocyte population. The RBC histogram corresponds to the elevated MCV and the PLT histogram appears normal for the most part .

61
Acute Promyelocytic Leukemia (Microgranular)
VOLUME CONDUCTIVITY SCATTER The manual diff results indicate there is indeed a blast population. However, the DataPlot looks odd in that the cell populations are not clearly separated. Even rotating the cube does not help distinguish the individual cell populations. The Verify Diff suspect flag will also appear when the cell populations are not clearly separated as well as in instances when the monocyte population is greater than 20%. Monocyte populations >20% are not always considered normal and are sometimes associated with the beginnings of Myelodysplastic Syndromes or in this particular case, leukemias. Acute Promyelocytic Leukemias are uncommon but even more uncommon are the microgranular variants. This type of leukemia has promyelocytes that lack the “typical” intense azurophilic granulation and by the instrument as well as under the microscope, take on the appearance of unusual monocytes. MANUAL DIFF Lymph = 2 Mono = 1 Blast = 97 CONDUCTIVITY SCATTER

62
MYSTERY #4 Mystery # 8.

63
Medical Mystery #4 In this case, the first thing that generally catches the Technologist’s attention is the elevated WBC. This patient also has a very elevated Lymphocyte percent and a distinct “lymphocyte only” peak on the WBC histogram.

64
Chronic Lymphocytic Leukemia
MANUAL DIFF Seg = 6 Lymph = 92 Mono = 2 The DataPlot also indicates a large population of lymphocytes that also agree with the WBC histogram and manual differential. One interesting thing to note is how the Lymphocyte population appears to spread out with what might be two populations. In the more aggressive phases of CLL, the peripheral smear will show two types of lymphs….small normal lymphs and larger, younger lymphs. Unfortunately in this case, the cube did not get rotated to get a better view of the dual lymph populations. Remember too, that smudge cells do not circulate in the peripheral blood. They are artifact created by fragile lymphs when the smear is made.

65
CLL WITH SMUDGE CELLS

66
CHRONIC LYMPHOCYTIC LEUKEMIA
Typically >60 years of age Initially asymptomatic Increased WBC Increased % of small, normal lymphs (as disease progresses, more ‘immature’ lymphs appear Smudge cells

67
MYSTERY #5 Mystery #7 coming up.

68
12 Month Old Male These results come from a 12 month old male. The extremely low MCV and abnormal RBC morphology are apparent. HGB =

69
12 Month Old Male RBC Morphology 2+ Poik 3+ Aniso 4+ Hypo
The RBC histogram agrees with the very small MCV as the red cell population is almost leaning up against the RBC threshold. The PLTs are also very small as seen from the “shift to the left” on the PLT histogram. The strange “blip” at the end of the PLT histogram is indicative of very microcytic RBCs and RBC fragments that are small enough to get in under the 20fl cutoff. In this instance it would be important to verify the PLT count. RBC Morphology 2+ Poik Aniso Hypo 4+ Micro 1+ Target 2+ Ellipto 1+ Teardrop 1+ Poly

70
MANUAL DIFF Seg = 42 Lymph = 46 Mono = 5 Eo = 5 Baso = 2 NRBC = 1
The automated differential and dataplot indicate NRBCs which correlate with the manual diff. The NRBCs are small enough that they do not interfere with the white count and therefore the WBC is not corrected for these cells.

71
????? Iron Deficiency Thalassemia
It is pretty obvious that iron deficiency is a possiblity but due to the abnormal RBC morphology, the diagnosis of Thalassemia was also entertained.

72
RETIC RESEARCH POPULATIONS
Sickle Thalassemia Low Volume Lymphs =CLL Retic populations have been studied extensively. One of the advantages of studying retic populations is that several distinct patterns emerge with particular diseases. If the “research icon” is clicked and the results fit a distinct pattern, a “research” suspect flag will emerge. The three most commonly seen are Sickle, Thalassemia and Low Volume Lymphs (small lymphs often associated with CLL). These “research” suspect flags cannot be reported but they can be used by the Technologist to “clue” them into particular cells they might see at the scope. In this particular case, they ran a retic but did not “click” the research icon to see if the instrument “suspected” Thalassemia.
. These research suspect flags cannot be reported but they can be used by the Technologist to clue them into particular cells they might see at the scope. In this particular case, they ran a retic but did not click the research icon to see if the instrument suspected Thalassemia.")
73
MYSTERY #6 Mystery #7 coming up.

74
Case Study History 74 year old female 20lb unexplained weight loss
Fever Malaise Sore throat Muscle aches 2 weeks duration

75
HISTOGRAM DATA Blasts or large lymphs

76
Auer rods are defined as a coalescence of the azurophilic granules and are only seen in non-lymphocytic leukemias ??????? AUER ROD

77
Manual Differential Seg = 4 Band = 1 Lymph = 17 Mono = 3
BLAST = 75 w/ occ Auer rod

78
ACUTE MYELOCYTIC LEUKEMIA
Sudden onset Anemic Variable WBC Decreased PLT count >10% Blasts in peripheral blood Special Stains & Flow markers + for myelogenous cell lines

79
FLOW CYTOMETRY DATA PLOTS
CD45 is a generic marker for all cell lines. CD117 is considered a myelocytic marker. If a patient is positive for this marker, they are considered a good candidate for a newer chemotherapeutic drug called GLEVEC.

80
IMMUNOPHENOTYPIC RESULTS
60% population of myeloid blasts CD34 & CD11b (partial) + CD64+, CD33+, CD15+, CD56+ CD117+, MPO+ Negative for: HLA-DR, CD7, CD19, CD20, CD22, CD3, CD8, and TDT
 + CD64+, CD33+, CD15+, CD56+ CD117+, MPO+ Negative for: HLA-DR, CD7, CD19, CD20, CD22, CD3, CD8, and TDT.")
81
MYSTERY #7 Mystery #7 coming up.

82
Case Study History 83 year old male Unexplained weight loss Malaise
Night sweats Slight hepatosplenomegaly

85
LAB RESULTS Manual Diff: Seg = 33 Band = 15 Lymph = 19 Mono = 6
Meta = 11 Myelo = 10 Blast = 6

86
???

87
VCS 3-D Data Plot Neutrophil Series Neutrophils Bands Metas Myelos
Pros Ne Blasts

88
VCS 3-D Data Plot Monocytes Monoblasts

89
FLOW CYTOMETRY DATA PLOT CD14+ CELLS CD14 = Monocytic Cells

90
FLOW CYTOMETRY PATHOLOGIST INTERPRETATION
The immunophenotypic findings reveal increased monocytes (26%) and 52% granulocytes with a shift toward immaturity and diminished side scatter. There is no evidence of increased blasts, a monoclonal B cell or aberrant T cell process. The immunophenotypic findings are suggestive of a myeloproliferative process. Acute monocytic leukemia cannot be entirely excluded. Clinical pathologic correlation is required for final diagnosis.
 and 52% granulocytes with a shift toward immaturity and diminished side scatter. There is no evidence of increased blasts, a monoclonal B cell or aberrant T cell process. The immunophenotypic findings are suggestive of a myeloproliferative process. Acute monocytic leukemia cannot be entirely excluded. Clinical pathologic correlation is required for final diagnosis.")
91
MYELOPROLIFERATIVE DISORDERS
Defined as a hypercellular bone marrow with increased quantities of one or more of the cells lines: erythrocytes, leukocytes or platelets in the peripheral blood. It is thought to be a neoplastic, clonal proliferation of a single multipotential stem cell w/ one cell line predominating and often transforming into another.

92
SUMMARY Look at ALL the information provided by the instrument:
CBC parameters WBC Histograms RBC Histograms PLT Histograms Dataplots Suspect Flags Research Parameter Keep in mind when investigating or troubleshooting to look at ALL of the data: CBC parameters, WBC, RBC and PLT histograms, Differential DataPlots, Suspect Flags and that wonderful “research” icon.

93
SUMMARY Combine this information with what you see at the microscope
Ask for a “second opinion” from a peer Create an “abnormal file” Combine the information gives you with what you see at the microscope. Remember, you, the Technologist, are the expert! However, never hesitate to get a second opinion. Also, create an abnormal file as a reference for the future.l The instrument gives you the capability to save cases in a “saved list folder” for future reference. And if you don’t have one of the instruments with this capability, a notebook serves the same purpose. SAVED LIST FOLDER

94
Questions ???????

95
ANY QUESTIONS

96
Case Study History 14 year old female Hgb SS Asthmatic
Admitted in crisis

97
Lab Results CBC Results WBC = 11.5 corrected for NRBC’s RBC = 2.10
HGB = 6.6 corrected for icterus PLT = 349 RDW = 25.4 Morphology 3+ Aniso 3+ Poik 2+ Poly 3+ Sickle 3+ Pappenheimer Bodies 1+ Target Cells

98
Lab Results Chemistry Glucose = 104 Sodium = 142 Potassium = 3.9
BUN = 3 L Creatinine = 0.5 L CO2 = 28 Chloride = 108 Calcium = 8.3

99
Sickle Cell Pappenheimer bodies

100
Cellular interference with
corrected and uncorrected WBC

101
Manual Differential: 55% Seg 1% Band 36% Lymph 7% Mono 1% Eo 6 NRBC
NRBC’s Giant platelets Platelet clumps RBC fragments Lyse resistant RBCs Malaria very small lymphs Manual Differential: 55% Seg 1% Band 36% Lymph 7% Mono 1% Eo 6 NRBC

102
NRBC Enumeration: Cells must be present in BOTH the signature position of the scatterplot as well as a population of events consistent with NRBCs at 35fl on the WBC threshold. Threshold Interference Signature Position

103
Derivation of NRBCs THE WBC IS ONLY CORRECTED FOR NRBCs >35fl
WBC Histogram Presence of high take-off Standard deviation and shape of lymphocyte population Lymphocyte mean channel THE WBC IS ONLY CORRECTED FOR NRBCs >35fl VCS Dataplot Volume and light scatter mean channels differentiate suspected NRBCs from lyse resistant RBCs Conductivity channel differentiates NRBCs from PLT clumps and giant platelets

104
RETICULOCYTE COUNT WBC’s Retics Mature RBC’s Platelets/Debris
Historically, retics have been used as a tool to monitor erythropoiesis. In the past, manual retics were very time consuming and there was a high degree of imprecision resulting in CV’s from 25-50%. Now with automated retics, results are more standardized and precise. Automation has also introduced the IRF which is useful to monitor stem cell regeneration after bone marrow transplant, monitoring B12 or folate therapy as well as classifying and evaluating anemias. Platelets/Debris

105
Sickle Cell Disease Leukocytosis Howell-Jolly Bodies Increased NRBC’s
Increased bilirubin Numerous Target cells Anemia Numerous sickle cells Pappenheimer bodies Retic = 10-40% Hgb Electrophoresis: Hgb S (>50%) Hgb F (variable)
 Hgb F (variable)")
106
medical technologists

107
Research Population Data
NE2 The increasing SD corresponds to a more immature population of cells

108
Research Population Data
NE BLAST The increasing SD corresponds to a more immature population of cells

109
Bonus - RBC Grading Accurately measure MCV Accurately measure RDW
Detect dimorphic populations Graded RBC morphology Anisocytosis +, ++, +++ Microcytosis +, ++, +++ Macrocytosis +, ++, +++ Hypochromia +, ++, +++ Dimorphic RBC Population Micro RBCs/RBC Fragments RBC Agglutination

Similar presentations











 Stacking allows for passage through narrow blood vessels.>")


. Complete Blood Count ( CBC)>")





>")
