Download presentation
Presentation is loading. Please wait.

1
Asthma & Acute Breathlessness
Jenny Till Respiratory Nurse Specialist Cumbria PCT

4
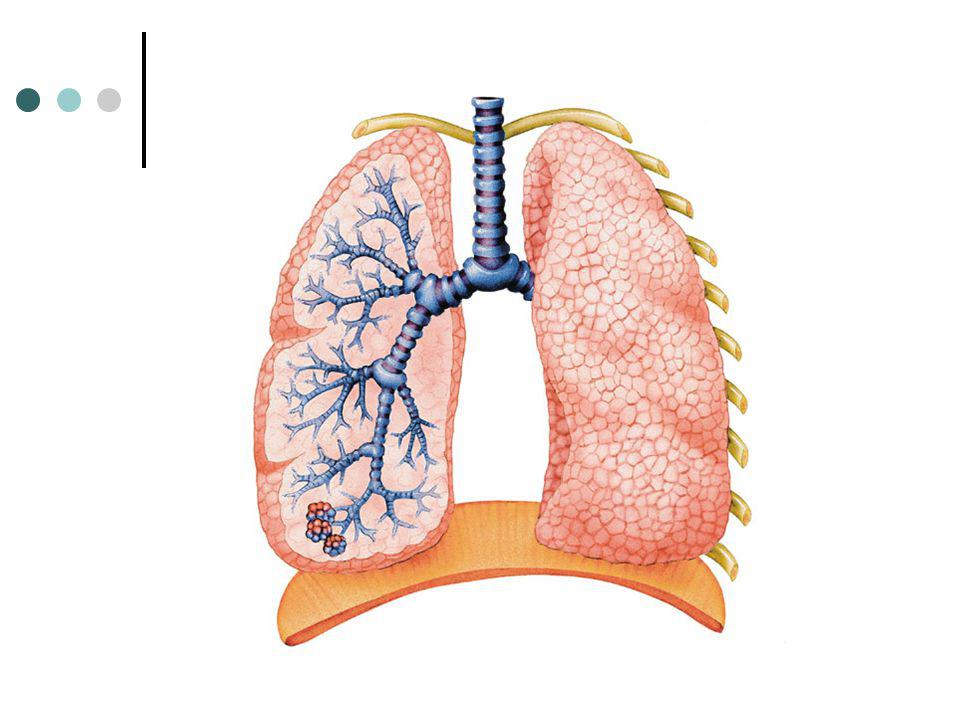
Airways and lungs

5
Alveolar capillary bed
Obscure the title of this slide and get the group to guess what this is. Emphasise that this is an intricate and delicate structure that is blown apart by cigarette smoke!

6
Asthma “A disease characterised by variable dyspnoea due to widespread narrowing of the peripheral airways, varying in severity over short periods of time, either spontaneously or as a result of treatment.” This is the easy bit! Get the students to volunteer the definition. Look for the key words – variable - reversible They will also come up with inflammatory. You can mention that COPD also involves inflammation, but that the processes and cells involved are different in asthma and COPD

7
Asthma Triggers

8
Worsening Asthma Increased symptoms Reliever medication less effective
Especially nocturnal symptoms Reliever medication less effective Tend to use more frequently Exercise restrictions Very vulnerable to severe “attack” At risk of death: previous admission with asthma or ongoing poorly controlled New presentation: consider inhaled FB

9
Signs of Severe Asthma Difficulty speaking
Dyspnoea at rest > 25 breaths per min Possible wheeze Possible cough Tachycardia at rest > 110 beats per min Pulse oximetry < 96% at rest on air (PEFR < 50% of best / predicted)
")
10
Life Threatening Asthma
Poor respiratory effort / silent chest May not appear distressed Fatigue / exhaustion Agitation / reduced level of consciousness Confusion Cyanosis Pulse oximetry < 92% at rest on air

11
Treatment of Acute Asthma
High dose bronchodilators 2.5mg neb salbutamol or Spacer (up to 10 puffs salb) Oral steroids 40 – 50mg for 5 days Oxygen If O2Sats <92% Aim to raise to at least 95% Call for medical assessment
 Oral steroids. 40 – 50mg for 5 days. Oxygen. If O2Sats <92% Aim to raise to at least 95% Call for medical assessment.")
12
Treatment of Acute Asthma
Review every 15 mins Repeat bronchodilators if poor response (PEFR 50-75% pred) Salb 5mg & add ipratropium 500mcg (spacer 8 puffs ipratropium) Referral to hospital Consider if PEFR < 75%, late in the day, previous severe attack General concern or poor response to treatment
 Salb 5mg & add ipratropium 500mcg (spacer 8 puffs ipratropium) Referral to hospital. Consider if PEFR < 75%, late in the day, previous severe attack. General concern or poor response to treatment.")
13
Follow up of patients All should be followed up within 48 hours
Ensure patients not admitted have clear instructions about when to call for help Bronchodilator not lasting 4 hours, increased symptoms again, PEFR 50-70%

14
COPD “Chronic obstructive pulmonary disease (COPD) is characterised by airflow obstruction. The airflow obstruction is usually progressive, not fully reversible and does not change markedly over several months. The disease is predominantly caused by smoking.”(NICE 2004) Start the session by pointing out the main features: Chronic Progressive Non-variable Non-reversible
 is characterised by airflow obstruction. The airflow obstruction is usually progressive, not fully reversible and does not change markedly over several months. The disease is predominantly caused by smoking. (NICE 2004) Start the session by pointing out the main features: Chronic. Progressive. Non-variable. Non-reversible.")
15
Airways and lungs

16
Alveoli Emphysema: a result of the air sacs being “dissolved away”
and also less Support for the airways Alveoli

17
Alveolar capillary bed
Obscure the title of this slide and get the group to guess what this is. Emphasise that this is an intricate and delicate structure that is blown apart by cigarette smoke!

18
Persistent and progressive
Is it asthma or COPD? Asthma COPD Smoker or ex-smoker Possible Nearly always Symptoms under 45 yrs Often Rare Chronic productive cough Uncommon Common Persistent and progressive Breathlessness Variable This is the table from the NICE guidelines It is not exhaustive. Talk about FH and PH asthma and atopy Mention undiagnosed childhood asthma Occupation Variability of symptoms – Asthma has ‘good and bad days’, COPD has ‘bad days and worse days’ Night time waking with breathlessness and / or wheeze Common Uncommon Significant diurnal or day to day variation in symptoms Common Uncommon

19
Assessment of acute COPD
Breathlessness at rest? Rapid deterioration / exhaustion? Cyanosis? Acute confusion? Worsening swollen ankles? Significant comorbidity? Cardiac or diabetes Ability to cope at home? Pulse oximetry (< 90% usually admit)
")
20
Management of COPD exacerbation
Salbutamol 2.5mg neb (4 – 8 puffs spacer) Oxygen (usually 24% – 28% - 40%) Maintain sats between 90 – 93% Consider prednisolone (30mg 7-14 days) Consider antibiotics (usually amoxycillin) Consider an ECG if suspecting cardiac comorbidity New home care service next year?
 Oxygen (usually 24% – 28% - 40%) Maintain sats between 90 – 93% Consider prednisolone (30mg 7-14 days) Consider antibiotics (usually amoxycillin) Consider an ECG. if suspecting cardiac comorbidity. New home care service next year")
22
Acute Breathlessness Acute asthma Anaphylaxis Acute COPD Pneumonia
Anxiety – hyperventilation Heart disease Angina, MI, LVF / pulmonary oedema Pulmonary Embolism Pneumothorax Spontaneous & post injury Inhaled foreign body / bronchial cancer Diabetic Ketoacidosis

23
SOS Admit to hospital Severe chest pain Cyanosis Acute confusion
Loss of consciousness Abnormal vital signs Particularly severe breathlessness Or exhaustion as a result

24
Information gathering
Precipitating factors Time course Presenting symptoms / signs Associated symptoms Allergies Medications Chemist / herbal / illicit drugs General health

25
Presenting signs / symtoms
Onset & timing? Anything make it worse / better? Intermittent / persistent? Exercise tolerance Normal & now Worse at night? Worse lying flat?

26
Equipment Pulse Oximeter MDI & Spacer Oxygen

27
Oxygen Saturation (SaO2)
Oxygen carried in bloodstream bound to haemoglobin (& small amount in plasma) 1 Hb can carry 4 O2 = 100% saturated Pulse oximeter measures the average % saturation of haemoglobin in sample
 1 Hb can carry 4 O2 = 100% saturated. Pulse oximeter measures the average % saturation of haemoglobin in sample.")
28
Pulse Oximetry Measures light absorbed by haemoglobin in blood
When oxygenated – red frequency When deoxygenated – blue frequency Needs to record pulsatile blood flow to ensure arterial blood Normal values = or > 97% Hypoxia = or < 96% Significant hypoxia < 92%

29
Pulse Oximetry – problems / limitations
Poor perfusion Vascular disease, vasoconstriction, (cold hands), irregular heart rhythms, severe shock –may give falsely low readings Nail varnish – falsely low readings Carboxyhaemoglobin – very bright red – SpO2 readings will be falsely higher Anaemia – will give falsely high readings Less haemoglobin, less O2 carried SpO2 cannot determine CO2 Levels or actual O2 levels
, irregular heart rhythms, severe shock –may give falsely low readings. Nail varnish – falsely low readings. Carboxyhaemoglobin – very bright red – SpO2 readings will be falsely higher. Anaemia – will give falsely high readings. Less haemoglobin, less O2 carried. SpO2 cannot determine CO2 Levels or actual O2 levels.")
Similar presentations



 Airway.>")


 in the lungs and in the.>")


: i1-i92.>")


: i1-i92.>")








 Diagnosis and management of chronic asthma in line with current BTS guidelines (Dr Lowery) 3 x Case.>")