Download presentation
Presentation is loading. Please wait.

1
Welcome Altrus Home Providers
Training Spring 2013 Atlanta, GA

2
Welcome and Legislative Update
Jessie Petrea, CEO

3
Medication Training and Infection Control

4
MEDICATION TRAINING FOR THE PCH 111-8-62-.20
Staff assisting with or supervising self administration of medications must be proficient in ENGLISH and able to read, write, and follow instructions in ENGLISH Objectives At the conclusion of this lesson, participants will be able to: 1. Correctly assist with medication administration in different forms 2. Accurately document medications with appropriate abbreviations 3. Explain the Six Rights of medication administration 4. Respond correctly to a medication error Whether you are just reminding residents to take medication or assisting residents in taking medication, training is necessary. Lack of knowledge is one of the main causes of medication errors. The purpose of medication management/training is to prevent errors.

5
Most common medication errors:
1. Human factors (65%): lack of knowledge, not paying careful attention, not following procedures correctly, or not being aware of a resident’s allergies. 2. Communication (15.8%): oral and written miscommunication, transcription errors, handwriting errors, misuse of zeroes, and decimal points, confusion of metric and other dosing units, confusing drugs with similar names, and incorrectly or misread abbreviations. 3. Environmental factor: poor lighting, heat, noise, and interruptions that distract workers. 4. Medication management is a process that involves: prescribing (physician, PA, or NP), transcribing (nurse or pharmacist interprets the physician order), dispensing (the medicine is prepared), and administering (the medicine is delivered to the resident). A medication error is when a medication is not administered as prescribed. Examples of medication errors include: omissions; administration of a medication not prescribed; wrong dosage; wrong time; wrong route; and documentation errors. A resident’s mistake in taking medications should also be reported. Not all medication mistakes will cause harm, but only the resident’s healthcare provider can decide whether an error is, or will be, harmful or not. EVERY MEDICATION ERROR MUST BE REPORTED IMMEDIATELY SO APPROPRIATE ACTION CAN BE TAKEN TO PREVENT HARM.
: lack of knowledge, not paying careful attention, not following procedures correctly, or not being aware of a resident’s allergies. 2. Communication (15.8%): oral and written miscommunication, transcription errors, handwriting errors, misuse of zeroes, and decimal points, confusion of metric and other dosing units, confusing drugs with similar names, and incorrectly or misread abbreviations. 3. Environmental factor: poor lighting, heat, noise, and interruptions that distract workers. 4. Medication management is a process that involves: prescribing (physician, PA, or NP), transcribing (nurse or pharmacist interprets the physician order), dispensing (the medicine is prepared), and administering (the medicine is delivered to the resident). A medication error is when a medication is not administered as prescribed. Examples of medication errors include: omissions; administration of a medication not prescribed; wrong dosage; wrong time; wrong route; and documentation errors. A resident’s mistake in taking medications should also be reported. Not all medication mistakes will cause harm, but only the resident’s healthcare provider can decide whether an error is, or will be, harmful or not. EVERY MEDICATION ERROR MUST BE REPORTED IMMEDIATELY SO APPROPRIATE ACTION CAN BE TAKEN TO PREVENT HARM.")
6
What to do when a medication error is made:
1. Once a medication error is discovered, report it immediately to the Home Provider and the resident’s primary care physician. 2. Complete an incident report and fax to Altrus, Inc and call Altrus, Inc. to report Fax a copy of the incident report to Healthcare Facility Regulation Division of Georgia Dept of Community Health at 3. Observe the resident for any side effects of the error, for example: changes in behavior (drowsiness or lethargy or hyperness), a rash, difficulty in swallowing or in walking. 4. Call 911 if necessary.
, a rash, difficulty in swallowing or in walking. 4. Call 911 if necessary.")
7
Basic Techniques for Handling Medication
1. Before handling any medications, gather all needed supplies. Wash your hands. Wash hands before any contact with each client. 2. Always, check drug expiration dates before using. Do not give expired drugs. 3. Details matter. Every letter, dot, and number is important when working with medications. 4. Work with good light and a minimum of distractions. Interruptions and haste cause errors. 5. Check to see if medications are to be given with food or on an empty stomach. Provide food if needed. 6. Always listen to the residents when they tell you something about their medicines. Relay any complaints, changes, or indications that something is wrong about a resident’s medicines or health to their health care provider or PCP (primary care physician).
.")
8
7. Store medications in the proper place locked at all times out of sight of residents and visitors. Store refrigerated meds in a locked box at all times. Medications kept in the resident’s room must be stored in a locked container with a key for the HP and the resident. Keep external or topical medications separate from the oral or internal medications for safety reasons. DO NOT ALLOW MEDICATIONS TO LIE AROUND IN THE OPEN, AT THE TABLE, BEDSIDE, OR COUNTER. 8. When administering medications, you are to observe the resident actually taking the medication. 9. A resident has the right to refuse medications. A resident is never forced to take medications. The resident’s physician should be contacted when medication is refused. 10. Staff is prohibited from repackaging more than one dose of a medication for subsequent administration. ONE DOSE ONLY is allowed. Remember anytime MORE than one dose of medication from a supply is placed in another container and labeled, it is considered DISPENSING – ONLY A PHARMACIST can dispense.

9
Medication Disposal Unused or expired medications must be properly disposed of using the current U.S. Food and Drug Administration (FDA) or U.S. Environmental Protection Agency (EPA) guidelines for the specific medications. ORDERS REQUIRED FOR ALL MEDICATIONS A home must not allow its staff to assist with, provide supervision of self-administered medications, including over-the counter medication, unless there a physician, advance practice registered nurse or physician assistant’s order or individualized prescription bottle, specifying clear instructions for its use on file for the resident. ALL MEDICATION ORDERS ARE TO BE MAINTAINED IN THE RESIDENT’S RECORD in the facility. Refill of prescribed medications must be obtained timely so that there is no interruption in the routine dosing. Where the home is provided with a new medication for the resident, the MAR (Medication Assistance Record) must be modified to reflect the addition of the new medication within 48 hours or sooner if the prescribing healthcare practitioner indicates that the medication change must be made immediately. THE HOME MUST OBTAIN NEW PRESCRIPTIONS WITHIN 48 HOURS OF RECEIPT OF NOTICE OF THE PRESCRIPTION OR SOONER IF THE PRESCRIBING PHYSICIAN INDICATES THAT A MEDICATION CHANGE MUST BE MADE IMMEDIATELY ( ). If the pharmacy does not have the medication needed for the immediate change, available and has not obtained further directions from the physician, the home must notify the physician of the unavailability of the prescription and request direction. When family members or residents bring in medication to be administered and there is no order, the physician should be contacted regarding administration and to obtain orders for the resident’s chart.
 or U.S. Environmental Protection Agency (EPA) guidelines for the specific medications. ORDERS REQUIRED FOR ALL MEDICATIONS. A home must not allow its staff to assist with, provide supervision of self-administered medications, including over-the counter medication, unless there a physician, advance practice registered nurse or physician assistant’s order or individualized prescription bottle, specifying clear instructions for its use on file for the resident. ALL MEDICATION ORDERS ARE TO BE MAINTAINED IN THE RESIDENT’S RECORD in the facility. Refill of prescribed medications must be obtained timely so that there is no interruption in the routine dosing. Where the home is provided with a new medication for the resident, the MAR (Medication Assistance Record) must be modified to reflect the addition of the new medication within 48 hours or sooner if the prescribing healthcare practitioner indicates that the medication change must be made immediately. THE HOME MUST OBTAIN NEW PRESCRIPTIONS WITHIN 48 HOURS OF RECEIPT OF NOTICE OF THE PRESCRIPTION OR SOONER IF THE PRESCRIBING PHYSICIAN INDICATES THAT A MEDICATION CHANGE MUST BE MADE IMMEDIATELY ( ). If the pharmacy does not have the medication needed for the immediate change, available and has not obtained further directions from the physician, the home must notify the physician of the unavailability of the prescription and request direction. When family members or residents bring in medication to be administered and there is no order, the physician should be contacted regarding administration and to obtain orders for the resident’s chart.")
10
UNDERSTANDING A WRITTEN PRESCRIPTION AND PRESCRIPTION BOTTLE LABELS
Using the above prescription label, note the following: 1. Clear instructions on the bottle as to dosing times 2. Name of drug (Brand/generic) 3. Name of Pharmacist filling Rx 4. How many pills in bottle and if any refills 5. Name of resident clearly on bottle 6. Expiration of the Rx 7. Prescribing physician 8. Date Rx filled Any questions regarding the written prescription or written physician orders, call the prescribing physician. M assey Pharmacy 1014 State Street Lincoln, GA 30128 709 - 554 3456 _____ ___________________________________________________ Rx /08/13 Jane Jones Take 2 pills by mouth three (3) times daily with food and at bedtime. Neurontin 300mg (Gabapentin) #120 pills D sp: J. J. Yost, RPh Dr. David Young Refills 0 Expired 1/08/14
 3. Name of Pharmacist filling Rx. 4. How many pills in bottle and if any refills. 5. Name of resident clearly on bottle. 6. Expiration of the Rx. 7. Prescribing physician. 8. Date Rx filled. Any questions regarding the written prescription or written physician orders, call the prescribing physician. M. assey Pharmacy State Street. Lincoln, GA _____. ___________________________________________________. Rx /08/13. Jane Jones. Take 2 pills by mouth three (3) times daily with food and at bedtime. Neurontin 300mg (Gabapentin) #120 pills. D. sp: J. J. Yost, RPh. Dr. David Young Refills 0. Expired 1/08/14.")
11
ASSISTANCE WITH SELF-ADMINISTRATION (111-8-62-.20)
A resident who is not capable of independent self-administration of medications may be assisted and supervised in self-administration by staff to following extent: 1. Staff providing such assistance or supervision may perform the following: a. Take the medication, in its previously dispensed, properly labeled container, from where it is stored, and bring the medication to the resident. b. Read the label, open the container, remove a prescribed amount of medication from the container, and close the container, in the presence of the resident. c. Place an oral dosage in the resident’s hand or in another container where the resident requests assistance. d. Apply topical medications. e. Assist with self-administration of drops, inhalers, nasal sprays, and patches. f. Return the medication container to proper secured storage. g. Assist the resident’s use of EPI PEN where the resident has known severe allergies for which an EPI PEN has been prescribed on condition that there is an established written protocol detailing how it is to be used and when. The protocol must include immediately calling Emergency Services, 911, after use of the EPI PEN. h. STAFF MAY NOT ADMINISTER INSULIN EVEN WHEN A CERTIFICATION OF NON-PROFESSIONAL HAS BEEN SIGNED. i. Staff assisting with or supervising self-administration of medications must be proficient in ENGLISH. Staff must be able to READ, WRITE, and FOLLOW written instructions in ENGLISH.

12
DOCUMENTATION OF MEDICATION ASSISTANCE
Staff is required to document on the MAR when a medication is administered, omitted, or refused. The MAR is a LEGAL document on how medications are administered in the facility (home). It is IMPORTANT that the documentation on the MAR is accurate. Medication must have an order and if none found and a new med is received, call pharmacy for a copy of the prescription or call the ordering physician for a copy of the prescription. If medication is omitted, you must document the reason, such as the resident was out of the home or the medication was not available on the MAR. Document immediately after you administer the medication to a resident and after you observe the resident actually take the medications and prior to administering to another resident’s medications. Documentation on the MAR is to be ACCURATE. Documenting immediately after administer a medication helps to ensure accurate documentation. PRECHARTING or documenting the administration of a medication BEFORE the medication is administered is PROHIBITED. Once the medication has been removed from the labeled package or container and prepared for administration, the medication is not put or placed back in the package or container. Medications are not transferred from one container to another except when preparation for administration.
. It is IMPORTANT that the documentation on the MAR is accurate. Medication must have an order and if none found and a new med is received, call pharmacy for a copy of the prescription or call the ordering physician for a copy of the prescription. If medication is omitted, you must document the reason, such as the resident was out of the home or the medication was not available on the MAR. Document immediately after you administer the medication to a resident and after you observe the resident actually take the medications and prior to administering to another resident’s medications. Documentation on the MAR is to be ACCURATE. Documenting immediately after administer a medication helps to ensure accurate documentation. PRECHARTING or documenting the administration of a medication BEFORE the medication is administered is PROHIBITED. Once the medication has been removed from the labeled package or container and prepared for administration, the medication is not put or placed back in the package or container. Medications are not transferred from one container to another except when preparation for administration.")
13
The MAR must contain the following:
Name of resident Any known allergies Name and telephone number of resident’s healthcare provider Name, strength, specific directions, and list of severe side effects & adverse reactions of each medication listed A place for staff who assist to record initials Time and date Indicator for med refusal, out of home, hospital, or medication error Document in progress notes any unusual reactions Document if PRN med has helped relieve pain or other symptoms The MAR is always changed to reflect new orders. Remember the MAR is a LEGAL document and must be kept updated. Once the medication has been removed from the labeled package or container and prepared for administration, the medication is not put or placed back in the package or container. Medications are not transferred from one container to another except when preparation for administration.

16
Residents have the right to administer their own medications
Residents have the right to administer their own medications. A physician’s order is necessary for the resident to self-administer. If there is a physician’s order for a medication to be self-administered, there is no requirement for the staff to observe the resident take each dose of the medication. This should not be necessary if the resident is capable of self-administering. It is helpful to have the medications that are self-administered on the MAR. Staff should NOT DOCUMENT on the MAR that they are administering the medications. When a PRN is ordered 1 or 2 pills, document if 1 or 2 were given. If a medication is not prescribed for administration every day, mark out the days the medication is not to be administered. This helps to prevent medication error. When a medication dosage is changed, the correct way to add to the MAR is to discontinue the present order and rewrite the order. Mark the date to start the new order.

17
THE SIX RIGHTS 1. RIGHT Person. Call the resident by name. Read the resident’s name on the MAR. Match the name on the medication with the resident. 2. RIGHT Drug. Compare the name of the drug on the MAR with the container. Brand/generic must appear the same. Which ever name should be same name on the MAR. If not contact HP, physician and/or pharmacy for clarification. 3. RIGHT Dose. Check the dosage on the medication container and be sure it is identical to the dosage written on the medication paperwork. The resident must take precisely the right number of pills and correct amount of liquid medication. 4. RIGHT Dosage form. Medications come in many forms. Make sure if the medication is pill form that it is pill form not liquid or some other form. EVERY LETTER AND NUMBER ON THE MEDICATION ORDERS MUST MATCH THE MEDICATION PACKAGE. If the orders say “SR” for sustained release, the medication package must say “SR”. 5. RIGHT Time. Check and double check the date, the day of the week, and the time of day. All three must be the same on the medication paperwork and the medication container, and must match the current date, day and time. Most organizations require that residents take medications within one hour before or after the scheduled time. 6. RIGHT Route. This means that the way a drug is taken, such as by mouth, under the tongue, inhaled, or applied to the skin. Be sure the residents takes the medicine in the manner written on the medication container and paperwork.

18
MEDICATION ALERT BOOK MUST BE MAINTAINED
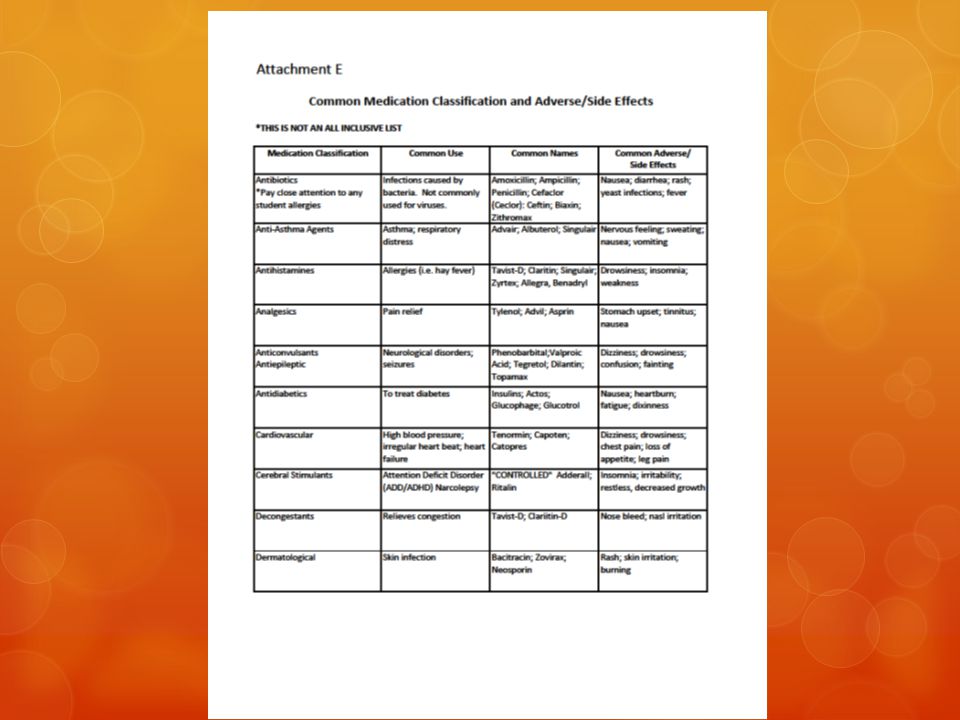
MEDICATION ALERT BOOK MUST BE MAINTAINED. The home must make medication information concerning descriptions of medication, dosing, side effects, adverse reactions and contraindications for each medication being administered to the residents immediately available for reference by staff providing medication assistance or administration. Recognition of Common Medication Classifications and Side Effects and Adverse Reactions for specific medications is important for staff to document and call immediately the resident’s healthcare provider as needed. MEDICATIONS MUST BE KEPT IN ORIGINAL CONTAINERS WITH ORIGINAL LABELS. All inhaler boxes and topical/externals must have original boxes maintained. See Common Medication Classifications and Adverse/Side effects – ATTACHMENT E

20
A HOME MAY STOCK OVER-THE-COUNTER (OTC) MEDICATIONS such as aspirin, advil, or acetaminophen for the convenience of residents who have PRN (as needed) orders for the specific medications and dosage. However, where the resident takes a OTC medication daily as prescribed in a written order by a licensed physician, nurse practitioner, or physician assistant, such as vitamins, low-dose aspirin, the resident must have an individual bottle of the prescribed medication that is kept for the resident’s individual usage. When assisting with administration of two or more different eye drops at the same time, you should wait 3 to 5 minutes between the each medication. If given one right after another, the solution will just run out of the resident’s eye. Wash hands before and after the eye drops. Never use household utensils such as a teaspoon or tablespoon to measure liquids. Teaspoons and tablespoons are not calibrated for measuring medications. Only devices that can be obtained from the pharmacy are calibrated for measuring medications used to administer medications. Never guess or approximate the amount of a medication to administer. See Conversion Table – See ATTACHMENT C

22
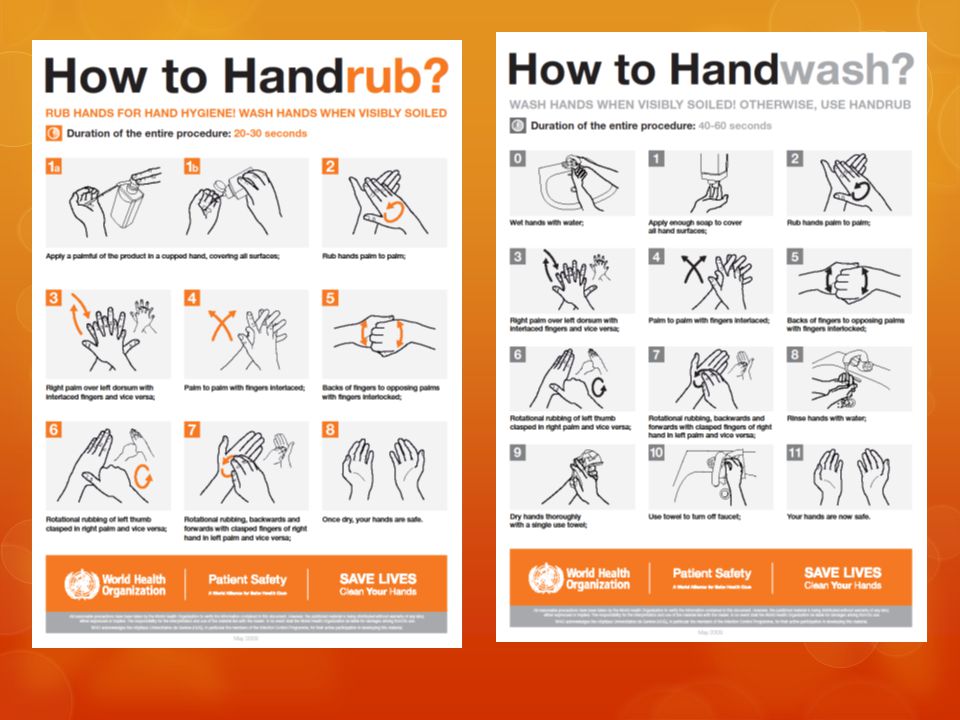
INFECTION CONTROL Infection control is one of your most important responsibilities. It is important to control the spread of germs and infection in a facility. The precautions you take to control the spread of infection are referred to as universal precautions. With universal precautions you treat blood and bodily fluids as infected with germs that cause disease. Universal precautions include: washing hands before and after resident contact, such as eye drops, wearing gloves when you may be exposed to blood or body fluids; disposing of used gloves properly; disposing of needles, syringes and lancets in leak proof, puncture resistant containers after use; never bending, recapping, or breaking needles after use and cleaning and disinfecting medication storage areas according to the homes policy. Handwashing is the single most important step you can take to protect yourself and residents from the spread of germs. When soap and water is not readily available, an antiseptic gel or product is used. Make sure no cross contamination of pills when cutting in half. The pill cutter has to be cleaned thoroughly before using to cut another resident’s pills. Gloves should be worn when applying topicals. Gloves should be worn with assisting with eye drops when an eye is red and irritated. Make sure to change gloves between residents to prevent the spread of germs.

24
MEDICATION SKILLS COMPETENCY DETERMINATIONS
Unlicensed staff in homes providing assistance with or supervision of self-administered medications must demonstrate to a qualified supervisor when hired and at least, annually thereafter, the necessary skills to perform the medication tasks assigned competently.

25
DISEASE OUTBREAK RESPONSE

26
TWO LEVELS OF PRECAUTION IN INFECTION PREVENTION
The CDC – Centers for Disease Control and Prevention is a federal government agency that is charged with the control and prevention of disease, in our country. They work to protect the public, by helping keep them healthy and safe, by education. The agency has developed a two-tiered (two level) way to prevent and control infection in health care: Standard Precautions and Transmission-Based (Isolation) Precautions. First Level – Standard Precautions Standard Precautions is the first level of precaution used to prevent and control infections in adult care homes. Standard Precautions are the basic tasks that health care workers must do when caring for each and every resident, in order to prevent and control the spread of infection. Why must Standard Precautions be used with each and every resident? Because there are residents you care for in adult care homes who have infections and you do not know they are infected. A resident may be infected who is not showing any signs or symptoms of being sick. Without using standard precautions, you can get the infection and pass it along to others. Standard Precautions means that you must treat ALL body fluids, non-contact skin, and mucus membranes, as if they were infected. • Body fluids can carry harmful germs. These include: blood, pus, liquid from sores, urine, stool, spit, droplets from sneezes and coughs, & sputum. • Non-contact skin includes: cuts, scratches, and sores that might ooze fluids which are infected with harmful germs. Non-contact skin which is not infected can also be a portal of entry for infections to enter the body. • Mucus membranes are the linings of natural body openings, such as the mouth, nose, rectum, genitals, and eyes.
 way to prevent and control infection in health care: Standard Precautions and Transmission-Based (Isolation) Precautions. First Level – Standard Precautions. Standard Precautions is the first level of precaution used to prevent and control infections in adult care homes. Standard Precautions are the basic tasks that health care workers must do when caring for each and every resident, in order to prevent and control the spread of infection. Why must Standard Precautions be used with each and every resident Because there are residents you care for in adult care homes who have infections and you do not know they are infected. A resident may be infected who is not showing any signs or symptoms of being sick. Without using standard precautions, you can get the infection and pass it along to others. Standard Precautions means that you must treat ALL body fluids, non-contact skin, and mucus membranes, as if they were infected. • Body fluids can carry harmful germs. These include: blood, pus, liquid from sores, urine, stool, spit, droplets from sneezes and coughs, & sputum. • Non-contact skin includes: cuts, scratches, and sores that might ooze fluids which are infected with harmful germs. Non-contact skin which is not infected can also be a portal of entry for infections to enter the body. • Mucus membranes are the linings of natural body openings, such as the mouth, nose, rectum, genitals, and eyes.")
27
Standard precaution rules that you should follow in the Adult Care Home:
•Wash your hands oWash, wash, wash your hands. Because hand washing is SO VERY important in the prevention and control of infections in the adult care homes. oImportant Points – Hands in the prevention of the spread of infection. Fingernails should be kept short and clean and no fake nails, gel nails, or nail extensions, because they can hide harmful germs. Jewelry should be left at home because germs can stick to them. Lotions should be used to keep hands soft and skin intact (not chapped or cracked). Use unscented type. Some lotions make medicated soaps less effective and breakdown latex. •
. Use unscented type. Some lotions make medicated soaps less effective and breakdown latex. •")
28
Wear gloves Any time you will or think you will come into contact with blood, body fluids, non-contact skin, or mucus membranes wear gloves. If you get blood or body fluids on you, IMMEDIATELY wash all of the areas of your skin that got contaminated. Open Sores on hands should be covered with bandage. Wear gloves and change after contact with residents or sooner if they become torn. Wear Gloves when HANDLING SHARPS. Wear gloves and be careful when using or handling anything that is sharp such as: razors, needles from injections, diabetic testing equipment, anything else that is sharp that could have touched blood or body fluids. Be careful not to cut yourself or your resident during shaves. Be careful not to stick yourself with diabetic testing supplies. ALWAYS put anything sharp that has been used on a resident in a biohazard container (needle disposal or “sharps” box) which is: only used just for sharps, hard and leak –proof, and labeled with a warning that the contents of the container are harmful. Never try to stick your hand in a sharps container or try to cram “one more” needle in the sharps container. Never over fill a needle disposal box. Never re-cap a needle or other sharp object because you may jab yourself. Never put anything sharp in a regular trash can.
 which is: only used just for sharps, hard and leak –proof, and labeled with a warning that the contents of the container are harmful. Never try to stick your hand in a sharps container or try to cram one more needle in the sharps container. Never over fill a needle disposal box. Never re-cap a needle or other sharp object because you may jab yourself. Never put anything sharp in a regular trash can.")
29
Clean all surfaces Clean all surfaces anytime blood or body fluids get on any surface in adult care homes: You must clean the surface with whatever product is provided where you work You must follow facility procedures and product instructions closely. Trash storage & disposal Know the proper way to get rid of trash. If it is plain trash that does not have any blood or body fluids on it, then throw it away in the regular trash can. BUT, if that piece of trash has blood, body fluids, then throw it away in a special biohazard waste bag. The best place to throw away contaminated trash is where the waste happened, biohazard waste may be placed in the regular trash can with a liner, then replace the liner and take the used liner to a utility room where it can be thrown in a biohazard container. Storage and disposal of bio-medical and hazardous wastes must comply with applicable federal, state, and local rules and/or standards.

30
•Handling linen Wear gloves when you change, carry, and discard in correct container. Roll linens up during change so that the dirty side is inside. Carry soiled linen away from your clothes. Do not shake dirty linen. •Spills Spills that involve body fluids are a safety threat in the adult care homes because of falls and risk of infection. Clean up spills wearing gloves. Absorb the spill and clean the area with the correct product, following the direction of the product. Discard waste in the appropriate container. Apply disinfectant to the area, following directions of the product. Place a warning cone or sign to warn others if there is a wet surface/fall risk.

31
Second Level – Transmission based precautions
Transmission Based Precautions are the second level of precautions used to prevent and control infections. Transmission Based Precautions are for residents who are infected or may be infected with specific types of infections. The three types of transmissions based precautions are: • Airborne Precautions: Prevent the spread of harmful germs that travel in the air at a distance. Harmful germs can float around for a while and can be carried by dust, moisture, and air currents. • Droplet Precautions: Prevent the spread of harmful germs that travel by droplets in the air. Droplets usually do no go farther than three feet, but could travel farther. Droplets are spread when an infected resident coughs, sings, sneezes, or laughs. • Contact Precautions: Prevent the spread of harmful germs spread by direct contact (norovirus).
.")
32
Housekeeping •Surfaces:
Clean surfaces (floors, walls, tabletops) regularly and per policy of your adult care home. For resident areas, use the type of detergent/disinfectant, per direction of the product. Clean and disinfect high-touch surfaces more often. These include door knobs, hand rails, light switches, and surfaces in and around resident toilets. Use detergent and water for cleaning surfaces in non-resident areas. Clean walls, blinds, and window curtains, in resident areas, when they are visibly dusty or dirty. •Mops, Cloths, & Solutions: Prepare cleaning solutions daily or as needed, and replace with fresh solution. Change the mop head at the beginning of each day. Clean mops and cloths after use and allow to dry before re-use; or use single-use, disposable mop heads and cloths. •Carpeting: Vacuum carpeting in public areas and in general resident areas regularly, with equipment that is working well and designed to not stir up dust, but rid the area of dust. Routinely perform a good, deep cleaning of carpeting. Follow appropriate procedures for dealing with spills on carpeting. Spot-clean blood or body fluid spills, using appropriate cleaner and disinfectant.
 regularly and per policy of your adult care home. For resident areas, use the type of detergent/disinfectant, per direction of the product. Clean and disinfect high-touch surfaces more often. These include door knobs, hand rails, light switches, and surfaces in and around resident toilets. Use detergent and water for cleaning surfaces in non-resident areas. Clean walls, blinds, and window curtains, in resident areas, when they are visibly dusty or dirty. •Mops, Cloths, & Solutions: Prepare cleaning solutions daily or as needed, and replace with fresh solution. Change the mop head at the beginning of each day. Clean mops and cloths after use and allow to dry before re-use; or use single-use, disposable mop heads and cloths. •Carpeting: Vacuum carpeting in public areas and in general resident areas regularly, with equipment that is working well and designed to not stir up dust, but rid the area of dust. Routinely perform a good, deep cleaning of carpeting. Follow appropriate procedures for dealing with spills on carpeting. Spot-clean blood or body fluid spills, using appropriate cleaner and disinfectant.")
33
Medical Waste Disposal
Disposable syringes, needles, finger stick devices and other sharps, as well as blood of 20ml or more shall be treated as Medical Waste and disposed of as mandated by Georgia Law. Storage and disposal of bio-medical and hazardous wastes must comply with applicable federal, state, and local rules and/or standards.

34
FOODBORNE ILLNESS (food poisoning) is a common, costly, yet preventable, public health problem. Each year 1 in 6 Americans gets sick by consuming contaminated foods or beverages. Many different disease causing microbes, or pathogens, can contaminate foods, so there are many different foodborne infections. In addition, poisonous chemicals, or other harmful substances can cause foodborne diseases if they are present in food. These pathogens enter the body thru the gastrointestinal tract and the most common symptoms are nausea, vomiting, abdominal cramping, and diarrhea. The top five pathogens contributing to acquired foodborne illnesses: o Norovirus – it is the most common cause of foodborne illness, though it is rarely diagnosed, because the lab test is not widely available. Generally, causes more vomiting than diarrhea and may last for up to 3 days. It passes from one infected person to another, often through contaminated food, water, or environmental surfaces. Infected person can contaminate food as they prepare it, if they have the virus on their hands. o Salmonella – it is spread to humans via a variety of different foods of animal origins. It typically, includes fever, diarrhea, and abdominal cramps. In the immune weakened resident, it can invade the bloodstream and cause life-threatening infections o Clostridium perfringens – is commonly found on raw meat and poultry. It produces a toxin that causes illness. o Campylobacter – causes fever, diarrhea, and abdominal cramping. Mostly acquired from eating undercooked chicken or other food that has been contaminated with juices dripping from raw chicken. o Staphylococcus aureus – can grow in some foods and produce a toxin that causes intense vomiting.

35
•Foodborne Illness Safety
COOK - Use a food thermometer to measure the internal temperature of meat is a good way to be that it is cooked sufficiently to kill bacteria. Eggs should be cooked until the yolk is firm Separate - Avoid cross-contaminating foods by washing hands, utensils, and cutting boards after they have been in contact with raw meat or poultry and before they touch another food. Put cooked meat on a clean platter, rather back on one that held the raw meat. Chill – Refrigerate leftovers promptly. Bacteria can grow quickly at room temperature, so refrigerate leftover foods if they are not going to be eaten within 4 hours. Large volumes of food will cool more quickly if they are divided into several shallow containers for refrigeration. Clean – Wash produce. Wash hands. Rinse fresh fruits and vegetables in running tap water to remove visible dirt and grime. Remove and discard the outermost leaves of a head of lettuce or cabbage. Because bacteria can grow well on the cut surface of fruit or vegetables, be careful not to contaminate these foods while slicing them up on the cutting board, and avoid leaving cut produce at room temperature for many hours. Don’t be a source of foodborne illness yourself. Wash your hands with soap and water before preparing food. Avoid preparing food for others if you yourself have a diarrhea illness. Changing a baby’s diaper while preparing food is a bad idea that can easily spread illness. Report– Report suspected foodborne illnesses to your LOCAL HEALTH DEPT.

36
Presented by Sara Coleman
Personal Care Home Rules and Regs Changes Presented by Sara Coleman ALS Director

37
Changes Abuse Assisted living care Disabled individual Exploitation
Health Services Injury Licensed Residential Care Profile Proxy Caregiver Self-Administration of Medications Self Preservation

38
Application 111-8-63.05 Adds Requirement:
No application for licensure will be acted upon unless complete with all required attachments and fees. Application must truthfully and accurately disclose required information. The filing of an application for licensure constitutes a representation that the application is or will be in complete control of the home as of a specified date.

39
Permits 111-8-62.06 Restates existing requirements and adds:
Personal care home must not operate or allow another business to operate on the premises of the licensed personal care home where the business intrudes on the residents’ quiet enjoyment and use of the home.

40
Governing Body Renumbers and restates existing requirements and deletes requirements for provisional permits and adds: Facility must maintain correct contact informatin New policies and procedures requirements to include: Ongoing training of staff Health and hygiene issues/infection control Discipline procedures for staff who commit acts inconsistent with the policies of the home Quality assurance and peer review Medication management Specific use of proxy caregiver Volunteers Safety and security precautions Staffing plans If member of governing body serves as rep payee, funds must be used exclusively for the benefit and best interest of resident Certified mail must be accepted

41
Administration For homes first licensed after the effective date of rules, administrator must have either an: Associates degree GED or high school diploma and two years experience in health care setting. Administration must: Ensure P&P are effective and enforced Designate qualified staff as responsible staff Investigate serious incidents which result in injury or death Identify and implement opportunities for improvements in care Monitor and document staff performance Provide timely notification of the relocation address to the resident and family representatives and the Department if residents must be relocated due to an emergency situation.

42
Workforce Qualifications and Training
Additional training requirements: Identification of conduct constituting abuse, neglect or exploitation and reporting requirements along with the receipt of the copy of the LTCA Reporting Act. General infection control principles Secure unit must have at least one person present in the unit who has completed all as required by these rules and rules for Proxy Caregivers, if applicable. Written evidence of initial and annual work performance reviews - can be skills competency checklists. Must ensure private sitters, PCG are familiar with emergecy evacuation routes.

43
Staffing Ratios 1:15 during day and 1:25 during non-waking hours but ALSO: Must staff above the minimum ratios to meet specific residents’ needs Must develop and maintain staff plans Must maintain monthly work schedules with planned and actual coverage Must retain schedules for one year Home licensed for greater than 24 – staff must wear id badges clearly visible

44
Home Accountability and Inspections
Inspection report and POC must be visibly displayed Must file POC electronically within 10 days (when web site available and homes are notified) or in writing Must monitor the effectiveness of the POC Must complete and maintain an accurate and residential profile made available upon request Prohibit use of ‘assisted living’ , ‘assisted living care’ or ‘assisted living community’ to describe a licensed PCH.
 or in writing. Must monitor the effectiveness of the POC. Must complete and maintain an accurate and residential profile made available upon request. Prohibit use of ‘assisted living’ , ‘assisted living care’ or ‘assisted living community’ to describe a licensed PCH.")
45
Home Design Requirements
Must be constructed, arranged and maintained to provide for the independence, privacy and dignity of the residents with safe access. Laundry facilities must prevent cross-contamination of clean and dirty laundry. Temperature Requirements: Winter - can’t fall below 62 degrees during sleeping hours and 68 during waking hours Summer – start cooling at 80 degrees and if temperature reaches 85 degrees

46
Physical Plant Health and Safety Standards
Exterior of the homes must be kept clean, safe and in good repair. Space heaters must NOT be in use, except during emergencies after obtaining specific written approval of the fire safety authority within the jurisdiction.

47
Furnishings and Fixtures
The home must provide an extra long mattress upon request for residents whose height requires such. Bedding includes two sheets, a pillow, pillowcase, blanket and bedspread. Linen supply for twice the bed capacity if residents don’t supply their own linens. Must maintain an adequate supply of spare linens on hand to accommodate residents’ needs.

48
Admission A home is permitted to admit a resident without the required physical exam pursuant to a specific request for an emergency placement made by a governmental agency responsible for APS, law enforcement or case manager. The home must retain documentation of the need for emergency placement and obtain a copy of a physical exam within 14 days following the admission and it must be completed in its entirety.

49
Admission Agreement 111-8-62.16
Residents admitted after the effective date must have a statement in the admission agreement disclosing whether the home permits independent PCG, sitters or requires the purchase of such from the home or approved providers. Must disclose how and by what level of staff medications are handled in the home. Must specify whether unit or multi-dose packaging is required. Must provide an explanation of how social media, photos and other media are handled.

50
Services Home must complete an assessment of the resident upon admission and update as changes occur Family supports Functional capacity relative to ADL Physical care needs Medical information provided Cognitive and behavioral impairments Personal preferences For homes which provide proxy caregivers or specialized memory care: Must develop the resident’s individual written care plan within 14 days of admission and require staff to use the care plan as a guide for the delivery of care and services

51
Infection Control Sanitation and Supplies
Must have effective infection control program to minimize the spread of infection and food borne illnesses. Must include training, responding to disease outbreaks. Must use disposable gloves when working with residents.

52
Resident files A copy of the search results obtained from the National Sex Offender Registry and any resulting safety plan for residents, staff and visitors. Resident files must be maintained for three years.

53
Reporting Any accidental or unanticipated death of a resident not directly related to the natural course of the resident’s underlying medical condition. Any serious injury that results in medical treatment Disclose any subsequent remedial and quality measures taken by the home to make such injury or harm arising from the incident less likely to occur.

54
Proxy Caregiver Rules The proxy caregiver rules are ALL about:
Creating ACCESS to affordable quailty healthcare in our communities Using limited healthcare resources responsibly AND Improving health outcomes by allowing people with disabilities to live in community settings wisely

55
Guiding Principles for Rules
Individuals with disabilities MUST choose Licensed facilities MAY allow proxy caregivers ONLY ‘health maintenance activities’ may be performed Written informed consent Written plan of care must be done by licensed healthcare professional (typically an RN, but can also be done by a Physicians Assistant, pharmacist or Nurse Practicioner) to implement medical orders
 to implement medical orders.")
56
Some Key Features of the Rules:
Individual may hire or licensed facility may hire Regardless of who hires, there must be Signed informed consent Written plan of care by licensed healthcare professional w/medical orders Competency determination that proxy caregiver has knowledge and skills to do health maintenance activities

57
Features, continued Where facility provides proxy caregivers, there must be: Established written curriculum for training Satisfactory completion of skills competency checklist before licensed healthcare professional Satisfactory evidence of routine evaluations of skills competencies, at least annually if not more often Successful completion of Test of Functional Health Literacy for Adults if medication assistance provided

58
What Proxy Caregivers Can’t Do
Tasks that require the assessment and judgment of an RN to do, i.e. ‘nursing tasks’ Medication assistance where nursing skill is required, e.g. intravenous injections, open-ended PRN orders, mixing or calculating med doses, OTC medications without order Applying debriding agents New health maintenance activities without required training by licensed healthcare professional

59
What Proxy Caregivers CAN do:
Can continue to assist with insulin Can do bandage changes for MINOR skin abrasions

60
Proxy Caregiver Forms Informed Consent Plan of Care
Skills Competency Checklist Instructions for Skills Competency Checklist Skills Competency Checklist – insulin by syringe FAQ’s

61
If you know of caregivers who would like to go into the homes of clients and care for them, take them to appointments and help them with ADL’s, please have them call Kim Dulek at Our sister company, Coastal HomeCare, is in need in the coastal areas from Florida line to South Carolina as well as Hinesville, Statesboro, Millen, Springfield and Sylania. Largest current need in Chatham county.

62
Love Shines Daily in Altrus Homes!

Similar presentations













 has developed standardized medication training, each district.>")








