Download presentation
Presentation is loading. Please wait.

1
Robert E. McGrath, Ph.D. Fairleigh Dickinson University
Integrating Psychological Assessment with Pharmacotherapy: A New Direction for Psychologists Robert E. McGrath, Ph.D. Fairleigh Dickinson University

2
Topics Enhancing Adherence Specificity in Problem Identification
The Structure of Clinical States

3
Enhancing Adherence Medication adherence about 50% (Haynes et al., 2002) Research on improving adherence involves multidimensional interventions (McDonald et al., 2002) 25% of non-adherent patients (never got Rx) reported they were adherent (Kobak et al., 2002) Haynes, R. B., McDonald, H. P., & Garg, A. X. (2002). Helping patients follow prescribed treatment: Clinical applications. JAMA, 2002, McDonald, H. P., Garg, A. X., & Haynes, R. B. (2002). Interventions to enhance patient adherence to medication prescriptions: Scientific review. JAMA, 2002, Kobak, K. A., Taylor, L., Katzelnick, D. J., Olson, N., Clagnaz, P., & Henk, H. J. (2002). Antidepressant medication management and Health Plan Employer Data Information Set (HEDIS) criteria: Reasons for nonadherence. Journal of Clinical Psychiatry, 63,
 25% of non-adherent patients (never got Rx) reported they were adherent (Kobak et al., 2002) Haynes, R. B., McDonald, H. P., & Garg, A. X. (2002). Helping patients follow prescribed treatment: Clinical applications. JAMA, 2002, McDonald, H. P., Garg, A. X., & Haynes, R. B. (2002). Interventions to enhance patient adherence to medication prescriptions: Scientific review. JAMA, 2002, Kobak, K. A., Taylor, L., Katzelnick, D. J., Olson, N., Clagnaz, P., & Henk, H. J. (2002). Antidepressant medication management and Health Plan Employer Data Information Set (HEDIS) criteria: Reasons for nonadherence. Journal of Clinical Psychiatry, 63,")
4
Lack of Effectiveness? Antidepressant effectiveness questionable (Kirsch et al., 2002, Prevention & Treatment) Overprescribing for mental disorders PCPs: approx. 100% (National Depressive and Manic Depressive Association, 2000) Psychiatrists: approx. 90% (Pincus et al., 1999) Psychologists: 15%? (John L. Sexton, personal communication, August 4, 2000; Wiggins & Cummings, 1998) Still likely many people do not adhere for whom medication would be effective (anxiety, psychosis) Kirsch, I., Moore, T. J., Scoboria, A., & Nicholls, S. S. (2002, July 15). The emperor's new drugs: An analysis of antidepressant medication data submitted to the U.S. Food and Drug Administration. Prevention & Treatment, 5, Article 23. Retrieved September 25, 2002, from National Depressive and Manic Depressive Association. (2000). Beyond diagnosis: Depression and treatment - A call to action to the primary care community and people with depression. Chicago: Author. Pincus, H. A., Zarin, D. A., Tanielian, T. L., Johnson, J. L., West, J. C., Pettit, A. R., Marcus, S. C., Kessler, R. C., & McIntyre, J. S. (1999). Psychiatric patients and treatments in 1997: Findings from the American Psychiatric Practice Research Network. Archives of General Psychiatry, 56, Wiggins, J. G., & Cummings, N. A. (1998). National study of the experience of psychologists with psychotropic medication and psychotherapy. Professional Psychology: Research and Practice, 29,
 Psychiatrists: approx. 90% (Pincus et al., 1999) Psychologists: 15% (John L. Sexton, personal communication, August 4, 2000; Wiggins & Cummings, 1998) Still likely many people do not adhere for whom medication would be effective (anxiety, psychosis) Kirsch, I., Moore, T. J., Scoboria, A., & Nicholls, S. S. (2002, July 15). The emperor s new drugs: An analysis of antidepressant medication data submitted to the U.S. Food and Drug Administration. Prevention & Treatment, 5, Article 23. Retrieved September 25, 2002, from National Depressive and Manic Depressive Association. (2000). Beyond diagnosis: Depression and treatment - A call to action to the primary care community and people with depression. Chicago: Author. Pincus, H. A., Zarin, D. A., Tanielian, T. L., Johnson, J. L., West, J. C., Pettit, A. R., Marcus, S. C., Kessler, R. C., & McIntyre, J. S. (1999). Psychiatric patients and treatments in 1997: Findings from the American Psychiatric Practice Research Network. Archives of General Psychiatry, 56, Wiggins, J. G., & Cummings, N. A. (1998). National study of the experience of psychologists with psychotropic medication and psychotherapy. Professional Psychology: Research and Practice, 29,")
5
Predicting Non-Adherence: Personality Approach
Do personality factors predict adherence? NEO-PI (Costa & McCrae, 1992): Neuroticism, Extraversion, Openness to Experience, Conscientiousness, Agreeableness Predicts adherence to psychotherapy (Miller, 1991; Muten, 1991), weight loss (Galluccio-Richardson et al., 2003), and kidney medication (Christensen & Smith, 1995): Small but significant effect for Conscientiousness and Rx regimen Costa, P. T. & McCrae, R. R. (1992a). NEO PI-R professional manual: Revised NEO Personality Inventory and NEO Five-Factor Inventory. Odessa, FL: Psychological Assessement Resources. Miller, T. R. (1991). The psychotherapeutic utility of the Five-Factor Model of personality: A clinician’s experience. Journal of Personality Assessment, 57, Muten, E. (1991). Assessment in a behavioral medicine program: An application of the Five-Factor Model. Journal of Personality Assessment, 57, Galluccio-Richardson, R., Capuano, C. A., and McGrath, R. E. (2003, March). The NEO-PI as a predictor of compliance with a weight loss regimen. Poster presented at the Annual Meeting of the Society for Behavioral Medicine, Salt Lake City UT. Christensen, A. J., & Smith, T. W. (1995). Personality and patient adherence: Correlates of the Five-Factor Model in renal dialysis. Journal of Behavioral Medicine, 18,
: Neuroticism, Extraversion, Openness to Experience, Conscientiousness, Agreeableness. Predicts adherence to psychotherapy (Miller, 1991; Muten, 1991), weight loss (Galluccio-Richardson et al., 2003), and kidney medication (Christensen & Smith, 1995): Small but significant effect for Conscientiousness and Rx regimen. Costa, P. T. & McCrae, R. R. (1992a). NEO PI-R professional manual: Revised NEO Personality Inventory and NEO Five-Factor Inventory. Odessa, FL: Psychological Assessement Resources. Miller, T. R. (1991). The psychotherapeutic utility of the Five-Factor Model of personality: A clinician’s experience. Journal of Personality Assessment, 57, Muten, E. (1991). Assessment in a behavioral medicine program: An application of the Five-Factor Model. Journal of Personality Assessment, 57, Galluccio-Richardson, R., Capuano, C. A., and McGrath, R. E. (2003, March). The NEO-PI as a predictor of compliance with a weight loss regimen. Poster presented at the Annual Meeting of the Society for Behavioral Medicine, Salt Lake City UT. Christensen, A. J., & Smith, T. W. (1995). Personality and patient adherence: Correlates of the Five-Factor Model in renal dialysis. Journal of Behavioral Medicine, 18,")
6
Predicting Adherence: Social Approach
Do social factors predict adherence? Theory of Planned Behavior (Ajzen, 1988): Ajzen, I. (1988). Attitudes, personality, and behavior. Milton-Keynes, England: Open University Press & Chicago, IL: Dorsey Press.
: Ajzen, I. (1988). Attitudes, personality, and behavior. Milton-Keynes, England: Open University Press & Chicago, IL: Dorsey Press.")
7
Predicting Adherence: Attitudinal Approach
Predicts adherence to drug abuse treatment (Kleinman et al., 2002), weight loss (Mancini et al., 2002), and psychiatric medications (Conner et al., 1998): Three attitudinal factors accounted for 65% of variability in intention to adhere to meds; two factors accounted for 38% of variability in behavior Kleinman, B. P., Millery, M., & Scimeca, M. (2002) Predicting long-term treatment utilization among addicts entering detoxification: The contribution of help-seeking models. Journal of Drug Issues, 32, Mancini, D. E., Capuano, C. A., & McGrath, R. E. (2002, April). Extension of the theory of planned behavior in the prediction of exercise behavior in obese women: Evaluation of attitude toward sedentary lifestyle, perceived social norms, and past exercise behavior. Presented at the Annual Meeting of the Society for Behavioral Medicine, Washington DC. Conner, M., Black, K., & Stratton, P. (1998). Understanding drug compliance in a psychiatric population: An application of the Theory of Planned Behaviour. Psychology, Health & Medicine, 3,
, weight loss (Mancini et al., 2002), and psychiatric medications (Conner et al., 1998): Three attitudinal factors accounted for 65% of variability in intention to adhere to meds; two factors accounted for 38% of variability in behavior. Kleinman, B. P., Millery, M., & Scimeca, M. (2002) Predicting long-term treatment utilization among addicts entering detoxification: The contribution of help-seeking models. Journal of Drug Issues, 32, Mancini, D. E., Capuano, C. A., & McGrath, R. E. (2002, April). Extension of the theory of planned behavior in the prediction of exercise behavior in obese women: Evaluation of attitude toward sedentary lifestyle, perceived social norms, and past exercise behavior. Presented at the Annual Meeting of the Society for Behavioral Medicine, Washington DC. Conner, M., Black, K., & Stratton, P. (1998). Understanding drug compliance in a psychiatric population: An application of the Theory of Planned Behaviour. Psychology, Health & Medicine, 3,")
8
Factors Affecting Rx Adherence
Ineffectiveness/preference for another medication Personality factors: responsibility/conscientiousness, resistance to authority Attitudinal factors Cost/reimbursement Anxiety about side effects Side effects Inadequate understanding: latency, duration Chaotic life circumstances

9
Therapeutic Assessment
Developed as a model for collaborative assessment consultation (Finn, 1996). RCT found TA reduced general distress (d = .80), and improved self-esteem (1.04) and hopefulness (.84) when compared to attention placebo (Finn & Tonsager, 1992) Finn, S. E. (1996). Manual for using the MMPI-2 as a therapeutic intervention. Minneapolis: University of Minnesota Press. Finn, S. E., & Tonsager, M. E. (1992). Therapeutic effects of providing MMPI-2 test feedback to college students awaiting psychotherapy. Psychological Assessment, 3,
. RCT found TA reduced general distress (d = .80), and improved self-esteem (1.04) and hopefulness (.84) when compared to attention placebo (Finn & Tonsager, 1992) Finn, S. E. (1996). Manual for using the MMPI-2 as a therapeutic intervention. Minneapolis: University of Minnesota Press. Finn, S. E., & Tonsager, M. E. (1992). Therapeutic effects of providing MMPI-2 test feedback to college students awaiting psychotherapy. Psychological Assessment, 3,")
10
Initial Interview Build rapport Frame questions collaboratively
Introduce information-gathering and decision-making as a collaboration Listen attentively Frame questions collaboratively Include whether medication is appropriate Explicitly encourage questions about medications Collect background information Begin with information relevant to questions Ask permission for additional questioning and explain why you need it Explore issues likely to impeded adherence Ask about resistance/incomplete participation

11
Initial Interview Ask about past medication experiences
Show genuine interest Empathize with previous experiences/hurts State shortcomings of previous experiences Offer contract that addresses previous hurts Ask to be alerted if patient feels mistreated Offer tentative answers Invite modification Invite questions Encourage future questioning Complete the prescription Initiate treatment Monitoring Contract about contact

12
Conclusions Prescriptions are a medical issue; prescribing is an interpersonal one Psychologists’ use of assessment can potentially improve adherence (and therefore, it is hoped, outcomes) Psychologists’ understanding of humanistic and interpersonal principles can potentially improve adherence and outcomes
 Psychologists’ understanding of humanistic and interpersonal principles can potentially improve adherence and outcomes.")
13
Specificity in Problem Identification
Actuarial versus clinical prediction and description Meehl (1954, 1956) Superiority of actuarial methods (Grove et al., 2000) Cognitive errors (Arkes, 1981) Covariance misestimation Hindsight bias Arkes, H. R. (1981). Impediments to accurate clinical judgment and possible ways to minimize their impact. Journal of Consulting and Clinical Psychology, 49, Grove, W. M., Zald, D. H., Lebow, B. S., Snitz, B. E., & Nelson, C. (2000). Clinical versus mechanical prediction: A meta-analysis. Psychological Assessment, 12, Meehl, P. E. (1954). Clinical versus statistical prediction: A theoretical analysis and a review of the evidence. Minneapolis: University of Minnesota Press. Meehl, P. E. (1956). Wanted ‑- A good cookbook. American Psychologist, 11,
 Superiority of actuarial methods (Grove et al., 2000) Cognitive errors (Arkes, 1981) Covariance misestimation. Hindsight bias. Arkes, H. R. (1981). Impediments to accurate clinical judgment and possible ways to minimize their impact. Journal of Consulting and Clinical Psychology, 49, Grove, W. M., Zald, D. H., Lebow, B. S., Snitz, B. E., & Nelson, C. (2000). Clinical versus mechanical prediction: A meta-analysis. Psychological Assessment, 12, Meehl, P. E. (1954). Clinical versus statistical prediction: A theoretical analysis and a review of the evidence. Minneapolis: University of Minnesota Press. Meehl, P. E. (1956). Wanted ‑- A good cookbook. American Psychologist, 11,")
14
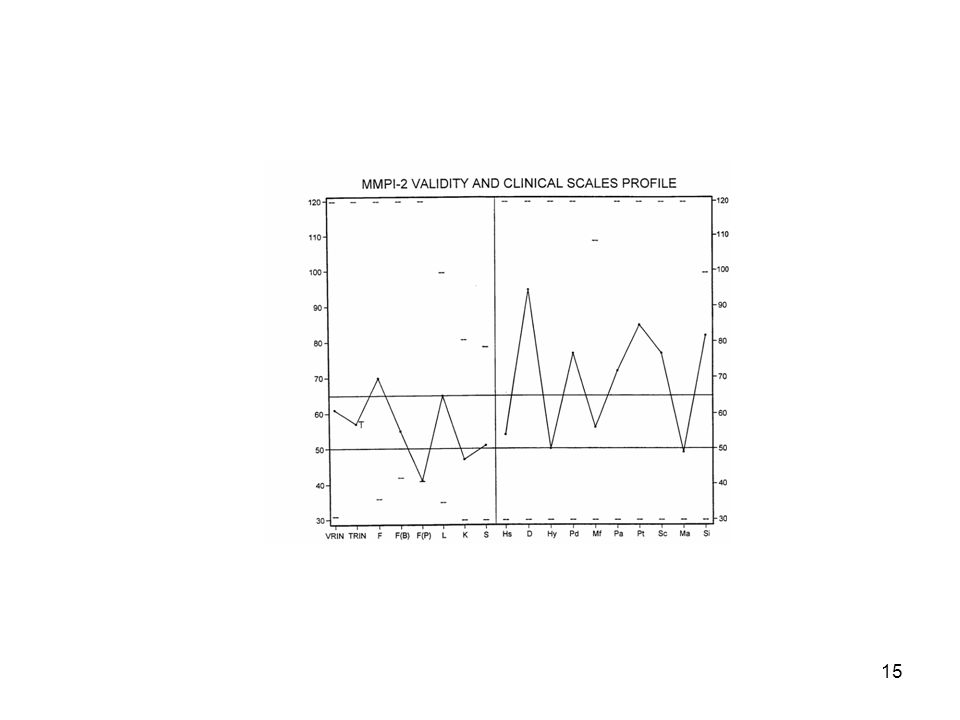
Restructured Clinical Scales
Affect research suggests that the discrimination of clinical states is muddied by the common Demoralization factor (Tellegen, 1985) RCSs consist of a measure of Demoralization, and scale-relevant items that are relatively independent of demoralization Tellegen, A. (1985). Structures of mood and personality and their relevance to assessing anxiety, with an emphasis on self-report. In A. H. Tuma & J. D. Maser (Eds.), Anxiety and the anxiety disorders (pp ). Hillsdale NJ: Lawrence Erlbaum.
 RCSs consist of a measure of Demoralization, and scale-relevant items that are relatively independent of demoralization. Tellegen, A. (1985). Structures of mood and personality and their relevance to assessing anxiety, with an emphasis on self-report. In A. H. Tuma & J. D. Maser (Eds.), Anxiety and the anxiety disorders (pp ). Hillsdale NJ: Lawrence Erlbaum.")
17
Conclusions Assessment can improve the accuracy of diagnosis and therefore treatment Increasing specificity in assessment instruments can enhance decision-making Functional components of clinical state may be more useful than diagnosis

18
The Structure of Clinical States
DSM assumes a categorical (biological) model Comorbidity NOS and mixed categories Subclinical categories Assessors often assume dimensionality based on psychometric considerations Neither is universally correct
 model. Comorbidity. NOS and mixed categories. Subclinical categories. Assessors often assume dimensionality based on psychometric considerations. Neither is universally correct.")
19
Taxometric Analysis Developed by Meehl and associates (Meehl & Yonce, 1994; Waller & Meehl, 1998) Identified several patterns that would emerge in relationships between measures only if their shared latent construct is categorical Meehl, P. E., & Yonce, L. J. (1994). Taxometric analysis: I. Detecting taxonicity with two quantitative indictors using means above and below a sliding cut (MAMBAC procedure). Psychological Reports, 74, Waller, N. G., & Meehl, P. E. (1998). Multivariate taxometric procedures: Distinguishing types from continua. Thousand Oaks CA: Sage.
. Taxometric analysis: I. Detecting taxonicity with two quantitative indictors using means above and below a sliding cut (MAMBAC procedure). Psychological Reports, 74, Waller, N. G., & Meehl, P. E. (1998). Multivariate taxometric procedures: Distinguishing types from continua. Thousand Oaks CA: Sage.")
20
MAXCOV (Maximum Covariance)
Three measures of latent variable η Sample divided into sequential subsets on X Covariance of Y and Z computed within each subset A graph of covariances should make an inverted U only if η is categorical

22
Findings for Diagnosis
Schizoid spectrum disorders seem categorical (Blanchard, Gangestad, Brown, & Horan, 2000; Erlenmeyer-Kimling, Golden, & Cornblatt, 1989) Melancholia appears categorical (Ambrosini, Bennett, Cleland, & Haslam, 2002; Haslam & Beck, 1994) Unipolar, non-melancholic depression consistently dimensional (Franklin, Strong, & Greene, 2002; Ruscio & Ruscio, 2000, 2002) Blanchard, J. J., Gangestad, S. W., & Brown, S. A. (2000). Hedonic capacity and schizotypy revisited: A taxometric analysis of social anhedonia. Journal of Abnormal Psychology, 109, Erlenmeyer-Kimling, L., Golden, R. R., & Cornblatt, B. A. (1989). A taxometric analysis of cognitive and neuromotor variables in children at risk for schizophrenia. Journal of Abnormal Psychology, 98, Ambrosini, P., Bennett, D. S., & Cleland, C. M. (2002). Taxonicity of adolescent melancholia: A categorical or dimensional construct? Journal of Psychiatric Research, 36, Haslam, N., & Beck, A. T. (1994). Subtyping major depression: A taxometric analysis. Journal of Abnormal Psychology, 103, Franklin, C. L., Strong, D. R., & Greene, R. L. (2002). A taxometric analysis of the MMPI-2 Depression Scales. Journal of Personality Assessment, 79, Ruscio, A. M., & Ruscio, J. (2002). The latent structure of analogue depression: Should the Beck Depression Inventory be used to classify groups? Psychological Assessment, 14, Ruscio, J., & Ruscio, A. M. (2000). Informing the continuity controversy: A taxometric analysis of depression. Journal of Abnormal Psychology, 109,
 Melancholia appears categorical (Ambrosini, Bennett, Cleland, & Haslam, 2002; Haslam & Beck, 1994) Unipolar, non-melancholic depression consistently dimensional (Franklin, Strong, & Greene, 2002; Ruscio & Ruscio, 2000, 2002) Blanchard, J. J., Gangestad, S. W., & Brown, S. A. (2000). Hedonic capacity and schizotypy revisited: A taxometric analysis of social anhedonia. Journal of Abnormal Psychology, 109, Erlenmeyer-Kimling, L., Golden, R. R., & Cornblatt, B. A. (1989). A taxometric analysis of cognitive and neuromotor variables in children at risk for schizophrenia. Journal of Abnormal Psychology, 98, Ambrosini, P., Bennett, D. S., & Cleland, C. M. (2002). Taxonicity of adolescent melancholia: A categorical or dimensional construct Journal of Psychiatric Research, 36, Haslam, N., & Beck, A. T. (1994). Subtyping major depression: A taxometric analysis. Journal of Abnormal Psychology, 103, Franklin, C. L., Strong, D. R., & Greene, R. L. (2002). A taxometric analysis of the MMPI-2 Depression Scales. Journal of Personality Assessment, 79, Ruscio, A. M., & Ruscio, J. (2002). The latent structure of analogue depression: Should the Beck Depression Inventory be used to classify groups Psychological Assessment, 14, Ruscio, J., & Ruscio, A. M. (2000). Informing the continuity controversy: A taxometric analysis of depression. Journal of Abnormal Psychology, 109,")
23
Implications Categorical status implies tight etiological net (biological?), dimensional a looser etiology (multidetermined?) Dimensional disorders unlikely to respond well to any one treatment

24
Discussion Prescribing is a complex interpersonal act
Case formulation and analysis of treatment outcomes may be enhanced by specificity in characterization of clinical states A greater understanding of clinical states may overcome biological assumptions suggesting unimodal treatments Opportunities for scientist-practitioners

Similar presentations










 Date.>")










