Download presentation
Presentation is loading. Please wait.

6
Blood pressure variation in the left ventricle (Blue line) & aorta (Red line) showing the cyclic variations of systolic and diastolic pressure
 & aorta (Red line) showing the cyclic variations of systolic and diastolic pressure")
10
Cushing Syndrome

18
11β-hydroxysteroid dehydrogenase enzyme mineralocorticoid BP & K +

30
vasogenic edema Metabolic Syndrome nephrosclerosis

32
o Sedentary lifestyle o Obesity o Insulin resistance o Metabolic syndrome o Aging o Alcohol o Vitamin-D deficiency

33
o Low birth-weight o Family history o Genetic o Na+ sensitivity o Sympathetic overactivity o Renin overactivity

42
DASH diet: (dietary approaches to stop hypertension) Rich in fruits & vegetables and low-fat or fat-free dairy foods.
 Rich in fruits & vegetables and low-fat or fat-free dairy foods.")
49
Classification of Hypertension Systolic pressure Diastolic pressure mmHg Normal 90–11960–79 Pre-hypertension 120–13980–89 Stage 1 140–15990–99 Stage 2 ≥160≥100 Isolated systolic HT ≥140<90

51
UK Hypertension Guidelines Starting Treatment threshold Group Treatment Target >160/100All those with such persisting readings >160/100.<140/90 >140/90 Have established cardiovascular disease, or Have C.V. Risk (>20% per 10 years), or Have evidence end-organ damage without D.M., or Ch. renal dis., without Macroalbuminuria (or D.M.) <140/90 >130/80Type-2 Diabetes alone.<130/80 >135/85Type-1 Diabetes alone.<130/80 >130/80 Type-1 or 2 Diabetes with microalbuminuria. Type-1 or 2 Diabetes with renal, eye or CV damage. <130/80 >130/80Chronic renal disease with Macroalbuminuria.<125/75
, or Have evidence end-organ damage without D.M., or Ch. renal dis., without Macroalbuminuria (or D.M.) <140/90 >130/80Type-2 Diabetes alone.<130/80 >135/85Type-1 Diabetes alone.<130/80 >130/80 Type-1 or 2 Diabetes with microalbuminuria. Type-1 or 2 Diabetes with renal, eye or CV damage. <130/80 >130/80Chronic renal disease with Macroalbuminuria.<125/75.")
56
DIABETIC HYPERTENSION Diabetic Nephropathy with (Microalbuminuria) ACEIs / ARBs. Diabetic Nephropathy with (Macroalbuminuria) ARBs / ACEIs. Diabetic Hypertension without Nephropathy ACEIs / ARBs +/- Thiazide +/- CCBs.
 ARBs / ACEIs. Diabetic Hypertension without Nephropathy ACEIs / ARBs +/- Thiazide +/- CCBs..")
57
Definition: [ GFR 60 ml / min / 1.73 m 2 (= serum creatinine 1.5 mg / dL or 1.3 mg / dL ) ] [ Albuminuria 300 mg/day (macroalbuminuria) ]. Treatment Goal: Aggressive BP Lowering 125/75 Compelling Drug: ACEIs or ARBs (Diabetic or non-Diabetic Nephropathy). N.B. GFR ( serum creatinine) up to 35% from baseline is acceptable, And is NOT a reason to withhold treatment unless hyperkalemia develops. In Advanced Renal Disease: [ = GFR 30 ml / min / 1.73 m 2 (serum creatinine 2.5 - 3mg / dL) ] : Increasing dose of loop diuretic is usually needed with ARBs or ACEIs) CHRONIC RENAL DISEASE
![Definition: [ GFR 60 ml / min / 1.73 m 2 (= serum creatinine 1.5 mg / dL or 1.3 mg / dL ) ] [ Albuminuria 300 mg/day (macroalbuminuria) ].](http://images.slideplayer.com/8/2367810/slides/slide_57.jpg "Treatment Goal: Aggressive BP Lowering 125/75 Compelling Drug: ACEIs or ARBs (Diabetic or non-Diabetic Nephropathy). N.B. GFR ( serum creatinine) up to 35% from baseline is acceptable, And is NOT a reason to withhold treatment unless hyperkalemia develops. In Advanced Renal Disease: [ = GFR 30 ml / min / 1.73 m 2 (serum creatinine mg / dL) ] : Increasing dose of loop diuretic is usually needed with ARBs or ACEIs) CHRONIC RENAL DISEASE.")
58
HEART FAILURE Asymptomatic HF ACEIs / ARBs + BBs. Advanced HF ACEIs / ARBs + BBs + Diuretic.

59
CEREBRO-VASCULAR STROKE Risks & Benefits of ACUTE Lowering of BP DURING acute CV Stroke are still unclear. Control of BP at intermediate levels (approximately 160/100 mmHg) is appropriate until condition is stabilized or improved. Stroke rates are lowered better by ACEIs / ARBs + Thiazide.
 is appropriate until condition is stabilized or improved. Stroke rates are lowered better by ACEIs / ARBs + Thiazide..")
60
ISCHEMIC HEART DISEASE Asymptomatic Angina: BBs or CCBs Symptomatic Angina: ACE-Is / ARBs (ARBs in Patients can’t tolerate ACE-Is) Acute MI (elevated ST segment) : ACE-Is / ARBs + BBs (ARBs in Patients can’t tolerate ACE-Is) N.B. CCBs if given there should be extreme cautious to avoid heart failure.

61
AA, aldosterone antagonist; ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin II-receptor blocker; βB, ß-blocker; CCB, calcium channel blocker; MI, myocardial infarction; CAD, coronary artery disease. JAMA. 2004;289(19):2560-2572. Compelling Indications Diuretic ßBßBßBßBACEIARBCCBAA Heart failure Post-MI High CAD risk Diabetes Chronic kidney disease Recurrent stroke prevention
: Compelling Indications Diuretic ßBßBßBßBACEIARBCCBAA Heart failure Post-MI High CAD risk Diabetes Chronic kidney disease Recurrent stroke prevention.")
67
The Use of Diuretics Require Electrolyte & Acid-base Balance Monitoring

71
Osmotic mannitol glucose furosemide HCT chlortalidone spironolactone CAI acetazolamide

73
Adverse EffectType of DiureticsExampleClinical Effect HypovolemiaLoop Diuretic Thiazide Lasix HCT 25 mg/day Hypotension Thirst GFR HypokalemiaLoop Diuretic Thiazide Carbonic Anhydrase Inhibitor Lasix HCT 25 mg/day Acetazolamide Muscle weakness Cardiac arrhythmia HyperkalemiaPotassium Sparing DiureticsSpironolactoneMuscle Cramps Cardiac arrhythmia HyponatremiaLoop Diuretic Thiazide Lasix HCT 25 mg/day Neurological manifestations Metabolic AlkalosisLoop Diuretic Thiazide Lasix HCT 25 mg/day CNS manifestations Cardiac arrhythmia Metabolic AcidosisPotassium Sparing Diuretics CAI Amilorides – triamterene Acetazolamide muscle weakness neurological symptoms seizures Decrease Ca++ ExcretionThiazideHCTPrevents Osteoporosis Prevents Renal calculi HyperuricemiaLoop DiureticLasixGout

75
α-adrenergic receptors are present in the smooth muscles e.g. prostate, arteries & veins. α 1 -adrenergic stimulation smooth muscles contraction vasoconstriction. α 1 -adrenergic blockers Relaxing vascular smooth muscles vasodilatation vascular resistance hypotension. α 1 -adrenergic blockers Relaxing prostate & U.B. neck.

80
o β 2 : Bronchodilation. Vasodilatation. Affect Glycogen Breakdown in Liver & Skeletal muscles o β 3 : Lipolysis. Renin Release BP. Stimulation of β -adrenergic Receptors: o β 1 : +ve Chronotropic on heart muscle. +ve Inotropic on heart muscle.

82
o Management of cardiac arrhythmias o Antihypertensive.

84
Other Side Effects of β -blockers : o Hyperkalemia. o Erectile dysfunction. o Bradicardia, heart failure, heart block. o Hypotension, orthostatic hypotension. o Tremors. o Insomnia

87
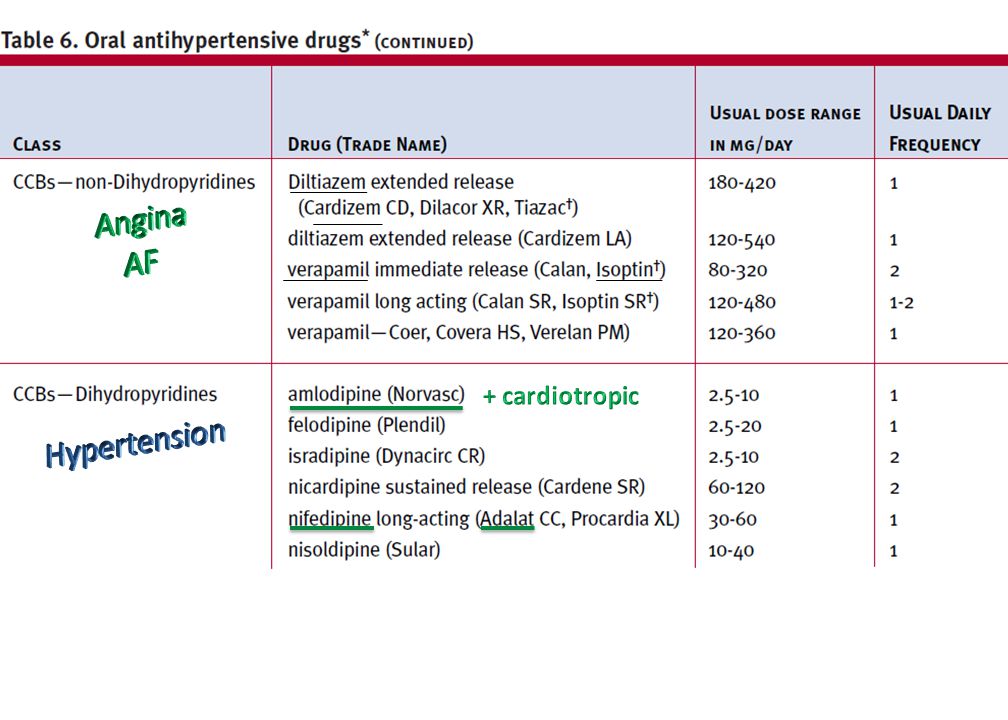
Mode of Action : Disrupt the calcium ions (Ca +2 ) transport at calcium channels: o In vascular smooth muscles o In cardiac muscle INDICATIONS : o Hypertension o Atrial flutter & AF o Angina
 transport at calcium channels: o In vascular smooth muscles o In cardiac muscle INDICATIONS : o Hypertension o Atrial flutter & AF o Angina")
88
o At high doses CCBs block the effect of insulin.

96
Glomerular Corpuscle Juxta glomerular cells macula densa Afferent arteriole Efferent arteriole Distal convoluted tubule Urinary chamber Bowman’s capsule Basement membrane - Podocytes Proximal convoluted tubule Urinary excretion: Fluid & electrolyte filtration from capillary side to urinary side through the basement membrane & podocytes to the urinary chamber of the glomerulus.

97
Direct Na + H 2 O retention water retention Blood

98
Direct Na + H 2 O retention water retention

99
Direct Na + H 2 O retention water retention

102
Direct Na + H 2 O retention water retention Blood water retention

104
Magdi El-ShalakanyMagdi El-Shalakany Mean Arterial Pressure (mm Hg) Intraglomerular Pressure Chronic hypertension with chronic renal disease Chronic hypertension Normal Low High 8012016018014010060 with normal renal function
 Intraglomerular Pressure Chronic hypertension with chronic renal disease Chronic hypertension Normal Low High with normal renal function")
108
smooth muscle cells

109
1.Hypertension 2. IGP 3.Renal Hyperfiltration 4.Renal Tissue injury 5.Structural & Morphological Changes : Mesangial tissue expansion Basement membrane thickening Podocyte pedicles’ detachment Intraglomerular Fibrosis 1. BP 2. IGP 3. Renal t. injury 4. GFR 5.Bradykinin S.E: Persist Dry Cough Inflammation symp Angio-edema 6.Tolerance Degradation

110
1. Hypertension 2. Left Ventricular remodeling (CHF) 3. IGP 4.Renal Hyper-filtration 5.Renal Tissue injury Chronic renal disease 6.Structural & Morphological Changes : o Mesangial tissue expansion o Basement membrane thickening o Podocytes pedicles’ detachment o Intraglomerular Fibrosis

111
1. BP 2. sympathetic tone peripheral resistance 3. Na + & water retention blood volume 4. sympathetic tone HR 5. COP & Heart work load & O 2 consumption 1. Hypertension 2. Heart Failure 3. Angina 4. Post myocardial infarction

112
6. Intra-Glomerular Pressure ( IGP) 7. Renal Hyper-filtration 8. Renal Tissue injury 9.Improve functional & structural renal condition 10. Structural & Morphological Changes 11. micro & macro-albuminuria 5. Diabetic Nephropathy 6. Chronic renal disease

113
1. Bradykinin & inflammatory related S.E: o Persistent Dry Cough o Angio-edema o Rash o Inflammation-related Pain 2. GFR Creatinine Clearance Rate (Ccr or C C ) serum Creatinine GFR ( serum creatinine) up to 35% from baseline is acceptable & is NOT a reason to withhold treatment unless hyperkalemia develops. 3.Hyperkalemia 4.Metallic Taste (sulfhydryl part in Captopril molecule)
 serum Creatinine GFR ( serum creatinine) up to 35% from baseline is acceptable & is NOT a reason to withhold treatment unless hyperkalemia develops. 3.Hyperkalemia 4.Metallic Taste (sulfhydryl part in Captopril molecule).")
114
1.Renal artery stenosis (bilateral) 2.Renal artery stenosis (Unilateral) 3.Impaired renal function (ACE-Is may GFR). 4.Aortic valve stenosis or cardiac outflow obstruction (ACE-I COP). 5.Hypovolemia or dehydration (ACE-Is diuresis ( fluid volume) & BP). 6.Pregnancy (category D)
. 5.Hypovolemia or dehydration (ACE-Is diuresis ( fluid volume) & BP). 6.Pregnancy (category D).")
116
1.Hypertension 2. IGP 3.Renal Hyperfiltration 4.Renal Tissue injury 5.Structural & Morphological Changes : Mesangial tissue expansion Basement membrane thickening Podocyte pedicles’ detachment Intraglomerular Fibrosis 1. BP 2. IGP 3. Renal t. injury 4. GFR C Cr 5.Bradykinin S.E: Persist Dry Cough Inflammatory symptoms Angio-edema 6.Tolerance Degradation

117
1. No Bradykinin & inflammatory related S.E: o Persistent Dry Cough o Angio-edema o Rash o Inflammation-related Pain 2.ARBs prevent excessive GFR Creatinine Clearance Rate which serum creatinine. It Keeps the Drop in GFR & C cr (if occur) 35% from baseline which is acceptable & So No Need to Withhold treatment. 3.No Decline of Anti-Hypertensive Effect 4. No Metallic Taste (sulfhydryl part in Captopril molecule)
 35% from baseline which is acceptable & So No Need to Withhold treatment. 3.No Decline of Anti-Hypertensive Effect 4. No Metallic Taste (sulfhydryl part in Captopril molecule).")
119
Diuretics α-blockers β-blockers CCBs ACE-Is/ARBs

120
-blockers -blockers Calcium antagonists AT 1 -receptor blockers Diuretics ACE inhibitors ESH Guidelines. J Hypertens. 2007;25:1105-1087. ESH= European Society of Hypertension

123
o CRD = Chronic Renal Disease. o GFR = Glomerular Filtration Rate. o BUN = Blood Urea Nitrogen = Uremia = Azotemia. o ESRD = End Stage Renal Disease (= Need for Dialysis or Kidney Transplant)
.")
124
o Plasma concentrations of creatinine and urea ( BUN = Blood Urea Nitrogen) are used to measure renal function. o Creatinine clearance rate ( C Cr or Cr Cl): “A measure for GFR”. o BUN and serum creatinine will not be raised normal Until 60% of total kidney function is lost. o Creatinine clearance ( C Cr or Cr Cl) is then more accurate to measure suspected renal disease.
: A measure for GFR . o BUN and serum creatinine will not be raised normal Until 60% of total kidney function is lost. o Creatinine clearance ( C Cr or Cr Cl) is then more accurate to measure suspected renal disease..")
125
o Proteinuria (elevated level of protein (albumin) in urine) : It is an important Prognostic marker for renal disease. o Albumin level 30 mg/24 hr urine is diagnostic for chronic kidney disease o Microalbuminuria is a level of 30-300 mg/24 hr urine; (can not be detected by usual urine dipstick methods). o Macroalbuminuria is a level 300 mg/24 hr urine.
. o Macroalbuminuria is a level 300 mg/24 hr urine..")
127
1. In patients 50 yr : SBP ( 140 mmHg) is much more important Risk Factor for CVD than DBP. 2. CVD Risk doubles with each increment of 20/10 mmHg (above normal). 3. Pre-hypertensive patients (SBP 120-139 / DBP 80-89) Require Lifestyle modifications to CV Risk.
. 3. Pre-hypertensive patients (SBP / DBP 80-89) Require Lifestyle modifications to CV Risk..")
128
4. Thiazide diuretic is drug of First choice for most patients with uncomplicated hypertension. 5. Certain Risk conditions are Compelling Indications For Other Anti-hypertensive Agents (e.g. ACE-Is, ARBs, CCBs, BBs …. etc) 6. Most hypertensive patients will require 2 or more antihypertensive agents to Achieve Treatment Goals: ( 140/90 mmHg, or 130/80 mmHg for Diabetic or Chronic Renal disease patients ) 7. If BP is 20/10 mmHg above Goal, consider additional agent therapy, one of which should be thiazide.
 6. Most hypertensive patients will require 2 or more antihypertensive agents to Achieve Treatment Goals: ( 140/90 mmHg, or 130/80 mmHg for Diabetic or Chronic Renal disease patients ) 7. If BP is 20/10 mmHg above Goal, consider additional agent therapy, one of which should be thiazide..")
129
8.Empathy & Motivating Patients are very important to reach Treatment Goal. 9.Responsible Physician’s Judgment remains paramount in the presence of these guidelines.

Similar presentations


















































































 Deduct 4 years High blood pressure (hypertension) Deduct 4 years High blood cholesterol (LDL) Deduct 1 year High blood.>")









>")
: Symptoms, Causes and Treatments!!!>")
