Download presentation
Presentation is loading. Please wait.

1
A.D.D

2
Tri State Neuro-Psych inc.
Daniel Kelleher MD Tri State Neuro-Psych inc.

3
What is ADD? A neurobehavioral disorder that begins in early childhood and can continue into adulthood ADHD may be associated with long-term adverse outcomes: Deficits in academic skills Deficits in family/social skills Learning disabilities May be accompanied by internalizing disorders (sadness, anxiety) as well as aggressive and oppositional disorders and learning disabilities Slide 4: What is ADHD? Attention-deficit/hyperactivity disorder (ADHD) is a neurobehavioral disorder that begins in early childhood and can continue into adulthood.1-5 It is the most common neurobehavioral disorder in children.1, 2 ADHD is characterized by 2 sets of core symptoms: inattention and a combination of hyperactive and impulsive behaviors.6 However, ADHD is a syndrome that affects a wide range of behaviors beyond the core symptoms. ADHD may be associated with deficits in academic, social, and family settings.6 Significant academic deficits may include poor organizational and study skills, as well as poor retention secondary to inattention. Associated learning disabilities may also be present.1 Patients should be evaluated for such disabilities. With regard to the family, the unrelenting challenge posed by a child with ADHD can cause ongoing parental and sibling frustration that can undermine family stability. Marital discord and divorce are common.2 There may also be long-term adverse outcomes associated with ADHD. Affected individuals have increased rates of accidents and physical injury.6 Adolescents with ADHD may be at significant risk for substance abuse, as well as conduct and antisocial personality disorders. Adults with ADHD are often underachievers, manifesting lower academic levels and socioeconomic status compared with those without this disorder.4 It is not uncommon for ADHD adults to have a long track record of vocational and relationship instability.4 ADHD may be accompanied by internalizing disorders such as sadness and anxiety, as well as aggressive and oppositional disorders.3 In addition, the core symptoms often lead to repeated failures which, in turn, can lead to low self-esteem.3 The combined effect of this constellation of symptoms can have serious long-term consequences if left untreated.3 1NIH. J Am Acad Child Adolesc Psychiatry ;39: 2NIH Consensus Development Panel. 1998;16(2):1-37. 3AACAP. J Am Acad Child Adolesc Psychiatry. 1997;36(10 suppl):85S-121S. 4Mannuzza S et al. Arch Gen Psychiatry. 1993;50: 5Mannuzza S et al. Arch Gen Psychiatry ;48:77-83. 6APA. DSM-IV
 as well as aggressive and oppositional disorders and learning disabilities. Slide 4: What is ADHD Attention-deficit/hyperactivity disorder (ADHD) is a neurobehavioral disorder that begins in early childhood and can continue into adulthood.1-5 It is the most common neurobehavioral disorder in children.1, 2 ADHD is characterized by 2 sets of core symptoms: inattention and a combination of hyperactive and impulsive behaviors.6 However, ADHD is a syndrome that affects a wide range of behaviors beyond the core symptoms. ADHD may be associated with deficits in academic, social, and family settings.6 Significant academic deficits may include poor organizational and study skills, as well as poor retention secondary to inattention. Associated learning disabilities may also be present.1 Patients should be evaluated for such disabilities. With regard to the family, the unrelenting challenge posed by a child with ADHD can cause ongoing parental and sibling frustration that can undermine family stability. Marital discord and divorce are common.2. There may also be long-term adverse outcomes associated with ADHD. Affected individuals have increased rates of accidents and physical injury.6 Adolescents with ADHD may be at significant risk for substance abuse, as well as conduct and antisocial personality disorders. Adults with ADHD are often underachievers, manifesting lower academic levels and socioeconomic status compared with those without this disorder.4 It is not uncommon for ADHD adults to have a long track record of vocational and relationship instability.4. ADHD may be accompanied by internalizing disorders such as sadness and anxiety, as well as aggressive and oppositional disorders.3 In addition, the core symptoms often lead to repeated failures which, in turn, can lead to low self-esteem.3 The combined effect of this constellation of symptoms can have serious long-term consequences if left untreated.3. 1NIH. J Am Acad Child Adolesc Psychiatry. 2000;39: NIH Consensus Development Panel. 1998;16(2): AACAP. J Am Acad Child Adolesc Psychiatry. 1997;36(10 suppl):85S-121S. 4Mannuzza S et al. Arch Gen Psychiatry. 1993;50: Mannuzza S et al. Arch Gen Psychiatry. 1991;48: APA. DSM-IV")
4
ADHD Attention deficit hyperactivity disorder as a diagnosis generates controversy. It is both under & over diagnosed-some believe it does not exist. Epidemiological studies show 5-10% of school age children may be classified with the disorder. It is a complex neuro-developmental constellation of problems rather than a single disorder. Often associated with co-morbid conditions. No diagnostic test to confirm clinical diagnosis

5
Historical background
1897 Kerr- Word blindness in smart children 1937 Bradley- Benzedrine & Brain activity 1941 Bender -Minimal Brain & Hyperkinesis 1947 Strauss-Brain damaged child syndrome 1963 Connors/Eisenberg-Ritalin&Hyperkinesis 1968 DSM II Hyperactivity 1971 Wender -Minimal Brain Dysfunction 1987 DSM III Attention Deficit Disorder 1994 DSM IV Attention Deficit Hyperactivity

6
Published in 2001, an updated DSM-IV (DSM-IV-TR) remained essentially the same. In summary, the diagnostic criteria for ADHD include: EITHER -- at least 6 symptoms of inattentiveness that have persisted for 6 months and are maladaptive (eg, "difficulty sustaining attention," "does not seem to listen," "easily distracted," "loses...toys, school assignments") OR -- at least 6 symptoms of hyperactivity (eg, "leaves seat in classroom", "runs about or climbs excessively", "talks excessively") and/or impulsivity (eg, "blurts out answers," "difficulty waiting turn," "interrupts or intrudes on others") that have persisted for 6 months and are maladaptive In addition, the symptoms needed to have been present before age 7, be expressed in at least two settings (DSM-III and DSM-IV mention work here), and demonstrate clear evidence of impairment.
 OR -- at least 6 symptoms of hyperactivity (eg, leaves seat in classroom , runs about or climbs excessively , talks excessively ) and/or impulsivity (eg, blurts out answers, difficulty waiting turn, interrupts or intrudes on others ) that have persisted for 6 months and are maladaptive. In addition, the symptoms needed to have been present before age 7, be expressed in at least two settings (DSM-III and DSM-IV mention work here), and demonstrate clear evidence of impairment.")
7
ADHD Legal Status Americans with Disabilities Act (ADA)
Rehabilitation Act of 1973

8
ADHD Epidemiology Most commonly diagnosed neurobehavioral disorder in children1, 2 Symptoms typically appear between the ages of 3 and 7 5%-10% of school-aged children may have ADHD; may bigher Boys are diagnosed 4 to 9 times more often than girls4 In up to 60% of children, symptoms of ADHD continue into adulthood5-7 Slide 5: ADHD Epidemiology Attention-deficit/hyperactivity disorder (ADHD) is the most commonly diagnosed neurobehavioral disorder of childhood and represents a major public health problem.1,2 ADHD affects 3% to 5% of school-aged children, with some estimates as high as 12%.1-3 ADHD is a disorder that occurs early in life, with symptoms typically appearing between the ages of 3 and 7. Boys are diagnosed more frequently than girls. Among children referred to child psychiatrists or psychologists, the boy-to-girl ratio varies from 4:1 to 9:1.4 The greater rate of referrals to clinics for ADHD among boys than girls may reflect the greater frequency of coexisting conditions, such as oppositional, defiant, or aggressive behavior occurring in boys.5 The ratios equilibrate in adolescents, with the boy-to-girl ratio being approximately 1:1.6 In a significant proportion of children (up to 60%), symptoms of ADHD may continue into adulthood.7-9 1NIH. J Am Acad Child Adolesc Psychiatry. 2000;39: 2NIH Consensus Development Panel. 1998;16(2):1-37. 3AAP. Pediatrics. 2000;105: 4APA. DSM-IV® 5Zametkin AJ et al. N Engl J Med. 1999;340:40-46. 6Cohen P et al. J Child Psychol Psychiatry. 1993;34: 7AACAP. J Am Acad Child Adolesc Psychiatry ;36(10 suppl):85S-121S. 8Mannuzza S et al. Arch Gen Psychiatry ;50: 9Mannuzza S et al. Arch Gen Psychiatry ;48:77-83.
 is the most commonly diagnosed neurobehavioral disorder of childhood and represents a major public health problem.1,2. ADHD affects 3% to 5% of school-aged children, with some estimates as high as 12%.1-3 ADHD is a disorder that occurs early in life, with symptoms typically appearing between the ages of 3 and 7. Boys are diagnosed more frequently than girls. Among children referred to child psychiatrists or psychologists, the boy-to-girl ratio varies from 4:1 to 9:1.4 The greater rate of referrals to clinics for ADHD among boys than girls may reflect the greater frequency of coexisting conditions, such as oppositional, defiant, or aggressive behavior occurring in boys.5 The ratios equilibrate in adolescents, with the boy-to-girl ratio being approximately 1:1.6 In a significant proportion of children (up to 60%), symptoms of ADHD may continue into adulthood NIH. J Am Acad Child Adolesc Psychiatry. 2000;39: NIH Consensus Development Panel. 1998;16(2): AAP. Pediatrics. 2000;105: APA. DSM-IV® Zametkin AJ et al. N Engl J Med. 1999;340: Cohen P et al. J Child Psychol Psychiatry. 1993;34: AACAP. J Am Acad Child Adolesc Psychiatry. 1997;36(10 suppl):85S-121S. 8Mannuzza S et al. Arch Gen Psychiatry. 1993;50: Mannuzza S et al. Arch Gen Psychiatry. 1991;48:")
9
ADHD Genetic Studies Strong familial association with increase first degree relatives Monozygotic twin studies show 60-90% concordance rate- Adoption/Consanguinity -positive correlation Specific Genes Polygenetic disorder involving multiple genes Dopamine transporter gene DAT 1 Dopamine receptor D4/Chromosome 3 ,5 ,11 ADHD/HKD polymorphisms on dopamine genes

10
ADHD Laboratory Test No specific blood test However
Lead level, CBC, EKG, Liver function may be indicated in certain cases. Blood level of certain medication required Toxicology screen in suspected cases of drug use EEG indicated for seizure

11
Recent Findings Low birth weight, Fetal Alcohol syndrome
Smoking during pregnancy + Alcohol,cocaine Higher rates injury medical bills. Untreated leads to sociopathy -increase driving offenses, delinquency, school& work failure_ Increased smoking & substance abuse Multimodal Treatment study (MTA) 2001 Closely monitored med. management more beneficial than intensive behavioral treatment Cross cultural validity- Dr..Bird-2000
 2001 Closely monitored med. management more beneficial than intensive behavioral treatment. Cross cultural validity- Dr..Bird")
12
ADHD Girls Girls show less hyperactivity than boys
Often Overwhelmed, disorganized & scattered Depression often coexists with ADHD Less potential for antisocial personality & substance abuse Tend to have higher rate of adolescent pregnancy and substance abuse compared to other females. Similar neuro- anatomical substrate

13
Adolescents face increasing demands for planning, organizing, self control, and time management, thus requiring increased executive function. What appeared as hyperactivity in the younger child emerges as restlessness In the adolescent. Poor organizational skills make high school and college years difficult for the adolescent and young adult with ADHD. Impairment follows and manifests as lower grades, more school suspensions, and higher college drop-out rates. Furthermore, higher rates of illegal substance and alcohol use in adults with ADHD appear to have their beginnings in the adolescent years.

14
TESTING Tri –State AFF Rating Scale.

15
Psychological Testing
Wechsler Intelligence Scale for Children (WISC-III) Wechsler Intelligence Scale for Children(WISC-R) Woodcock-Johnson Reading Mastery Test Peabody Individual Achievement Test Peabody Picture Vocabulary Test Vineland Adaptive Behavior Scales Thematic Apperception Test (TAT). Connors’ Parent &Teacher Rating Scale.
 Wechsler Intelligence Scale for Children(WISC-R) Woodcock-Johnson Reading Mastery Test. Peabody Individual Achievement Test. Peabody Picture Vocabulary Test. Vineland Adaptive Behavior Scales. Thematic Apperception Test (TAT). Connors’ Parent &Teacher Rating Scale.")
16
For children with ADHD, academic difficulties are common
For children with ADHD, academic difficulties are common. Among children with ADHD, prevalence of learning disabilities has not been well determined, with a wide range of reported levels from 9% to 94%. It is clear, that adults with ADHD have adaptive impairments relating to schooling in general. However, whether or not true learning disabilities remain an issue for adults with ADHD has not been determined. Conduct (20%) and oppositional-defiant (40%) disorders are commonly identified among children with ADHD. The prevalence of the disruptive behavior disorders decreases significantly beginning in adolescence and extending into adulthood; however, in adulthood, antisocial disorder is one of the comorbidities that can persist independently of continued ADHD symptoms.
 and oppositional-defiant (40%) disorders are commonly identified among children with ADHD. The prevalence of the disruptive behavior disorders decreases significantly beginning in adolescence and extending into adulthood; however, in adulthood, antisocial disorder is one of the comorbidities that can persist independently of continued ADHD symptoms.")
17
DSM-V® Defines 3 ADHD Subtypes
3 categories of ADHD (DSM-IV® criteria)1 Predominantly inattentive type Predominantly hyperactive-impulsive type Combined type Slide 6: DSM-IV® Defines 3 ADHD Subtypes The DSM-IV® defines specific subtypes of ADHD.1 The first is the predominantly inattentive type, which is diagnosed when only the criteria for inattention are met. The predominantly hyperactive-impulsive type is diagnosed when only the criteria for hyperactive and/or impulsive behavior are met. The combined type can be diagnosed when the symptoms for both inattention and hyperactivity/impulsivity are present; in all cases, persistence of symptoms for at least 6 months is a requisite. Those not meeting criteria are labeled “not otherwise specified” and include children who are impaired but who do not meet the full criteria for diagnosis. 1APA. DSM-IV® 1APA. DSM-IV
1. Predominantly inattentive type. Predominantly hyperactive-impulsive type. Combined type. Slide 6: DSM-IV® Defines 3 ADHD Subtypes. The DSM-IV® defines specific subtypes of ADHD.1 The first is the predominantly inattentive type, which is diagnosed when only the criteria for inattention are met. The predominantly hyperactive-impulsive type is diagnosed when only the criteria for hyperactive and/or impulsive behavior are met. The combined type can be diagnosed when the symptoms for both inattention and hyperactivity/impulsivity are present; in all cases, persistence of symptoms for at least 6 months is a requisite. Those not meeting criteria are labeled not otherwise specified and include children who are impaired but who do not meet the full criteria for diagnosis. 1APA. DSM-IV® APA. DSM-IV")
18
Meeting the Diagnostic Criteria for ADHD
Presence of 6 or more symptoms of inattention or hyperactivity/impulsivity that have persisted for at least 6 months to a degree that is maladaptive and inconsistent with developmental level Symptoms present before age 7 years Impairment from symptoms present in 2 or more settings Significant social, academic, or occupational impairment Exclude other mental disorders Slide 7: Meeting the Diagnostic Criteria for ADHD As shown in this slide, in order for a child to be diagnosed with ADHD, he or she must meet the criteria listed in the DSM-IV®.1 Symptoms of inattention include: carelessness; difficulty sustaining attention during activity; trouble following through; avoiding tasks requiring sustained mental effort; difficulty organizing; losing important items; easily distracted; forgetful in daily activities; and does not appear to be listening when spoken to directly. Symptoms of hyperactivity/impulsivity include: squirming and fidgeting; inability to stay seated; running/climbing excessively; being “on the go” or appearing “driven by a motor”; talking excessively; cannot perform leisure activity quietly; blurting out answers; cannot wait turn; and intrusive/interrupts others. It is important to note that the child must display the symptoms to a degree that is maladaptive and inconsistent with developmental level for a period of at least 6 months prior to the evaluation. Symptoms must cause functional impairment across 2 or more settings. A number of psychiatric conditions co-occur with ADHD. Between 10% and 20% of children with ADHD have mood disorders; 20% have conduct disorders; and up to 40% may have oppositional defiant disorder.2 1APA. DSM-IV 2Goldman LS et al. JAMA. 1998;279: APA. DSM-IV

19
DSM IV-R criteria for diagnosis
6 symptoms of inattention for>6months Fails to give close attention to details/makes careless mistakes in schoolwork/activities. Does not listen when spoken to directly. Does not follow through on instructions and fails to finish schoolwork,chores other duties. Difficulties organizing tasks and activities. Avoids and dislikes to engage in tasks that require sustained mental effort

20
ADD Difficulties sustaining attention in tasks or play activities.
Often loses things necessary for tasks or activities- toys,books, pencils, assignments. Easily distracted by extraneous stimuli. Often forgetful in daily activities. Daydreams in situations of stress

21
ADHD Impulsive Often blurts out answers before questions have been completed Often has difficulty waiting turn Often interrupts or intrudes on others- in conversations and games. Changes goals and other interests suddenly

22
ADHD Symptoms that caused impairment were present before age of 7years
Symptoms present in two or more settings Clear clinical evidence of significant impairment in social academic or occupational functioning Symptoms do not occur exclusively in PDD, SPT etc. i.e. Primary or Secondary

23
Psychiatric comorbidity
Depression Bipolar Affective Disorder Conduct disorder Oppositional Defiant disorder Generalized Anxiety Disorder OCD Substance use & abuse Hallucinations-/childhood schizophrenia MR

24
Neurological Substrate

25
The earliest indication of abnormal brain activity with ADHD came from electrophysiological studies, which demonstrated that children with ADHD exhibited lower amplitudes in brain areas believed to be correlated with attention and memory. In recent years, various imaging modalities have contributed both to confirming the validity of ADHD in adults and to better understanding the disorder. Magnetic resonance imaging (MRI) studies provide data showing that the prefrontal lobe and right caudate nucleus is smaller in patients with ADHD. In adults with ADHD since childhood, positron emission tomography (PET) scans have revealed decreased frontal cortical activity as well as abnormal regional and global glucose metabolism during the performance of a task involving executive function.
 studies provide data showing that the prefrontal lobe and right caudate nucleus is smaller in patients with ADHD. In adults with ADHD since childhood, positron emission tomography (PET) scans have revealed decreased frontal cortical activity as well as abnormal regional and global glucose metabolism during the performance of a task involving executive function.")
26
Additionally, PET scans actually have been able to demonstrate decreased dopamine neurotransmission in the left and medial portions of the prefrontal cortex. These findings are significant because the stimulant pharmacologic agents used to ameliorate ADHD symptoms are known to increase extracellular catecholamines. Functional magnetic resonance imaging (fMRI), a technique that maps neuronal activity within the brain by using the naturally occurring changes in blood oxygen levels that follow any neural activity, is just beginning to be applied to ADHD research. Preliminary investigations using fMRIs have been a pioneering modality in determining the etiology and pathophysiology of ADHD. FMRI comparison of adults with ADHD vs normal controls during a Stroop interference task demonstrated failure of the anterior cingulate gyrus to activate in the ADHD subjects, suggesting that these individuals were depending on a different part of the brain to accomplish this task.
, a technique that maps neuronal activity within the brain by using the naturally occurring changes in blood oxygen levels that follow any neural activity, is just beginning to be applied to ADHD research. Preliminary investigations using fMRIs have been a pioneering modality in determining the etiology and pathophysiology of ADHD. FMRI comparison of adults with ADHD vs normal controls during a Stroop interference task demonstrated failure of the anterior cingulate gyrus to activate in the ADHD subjects, suggesting that these individuals were depending on a different part of the brain to accomplish this task.")
29
Dopamine Pathways in ADD

30
Dopamine Pathways in ADD

32
EEG and ADD

33
Cortical abnormalities in children with ADHD
Results of structural brain imaging studies of patients with attention-deficit hyperactivity disorder have shown subtle reductions in total brain volume and in volumes of the right frontal lobe and caudate nucleus. Although various conventional volumetric and voxel-based methods of image analysis have been used in these studies, regional brain size and grey-matter abnormalities have not yet been mapped over the entire cortical surface in patients with this disorder. The task of mapping these features in patients with attention-deficit hyperactivity disorder continues to improve.

35
Abnormal morphology was noted in the frontal cortices of patients with attention-deficit hyperactivity disorder, with reduced regional brain size localised mainly to inferior portions of dorsal prefrontal cortices bilaterally. Brain size was also reduced in anterior temporal cortices bilaterally. Prominent increases in grey matter were recorded in large portions of the posterior temporal and inferior parietal cortices bilaterally.

37
The frontal, temporal, and parietal regions are heteromodal association cortices that constitute a distributed neural system, which subserves attention and behavioural inhibition. Physicians have identified region-specific anatomical abnormalities in cortical components of attentional systems, which may help better account for the symptoms of attention-deficit hyperactivity disorder. Volume 362, Number 9397 Lancet / Sowell

38
Our morphometric procedures allow more precise localization of group differences than do the methods used in previous studies," lead author Elizabeth R. Sowell, PhD, from the University of California at Los Angeles, says in a news release. "Our results therefore suggest that the disturbances in prefrontal cortices are localized to more inferior aspects of prefrontal regions than was previously appreciated. Our findings also indicate that prefrontal abnormalities are represented bilaterally, by contrast to the predominantly right-sided findings that were emphasized in other reports."

39
The findings are not only in brain regions controlling attention, but also in regions that subserve impulse control," says coauthor Bradley Peterson, MD, from Columbia University and the New York State Psychiatric Institute in New York City. "Disordered impulse control is often the most clinically debilitating symptom in children with ADHD." Although measures of the severity of ADHD symptom subtypes generally did not correlate significantly with these morphological measures, gray matter in the occipital lobe was inversely correlated with measures of inattention.

40
FMRI and ADD 8 yrs vs 28 yrs

41
Treatment of ADD

42
Enviroment Brain Body Mind

43
Treatment Triangle P Child T D

44
Pharmacotherapy is the first line of treatment for ADHD
Pharmacotherapy is the first line of treatment for ADHD. Studies of the treatment of ADHD in childhood show that pharmacological treatment is superior to behavioral treatment and that combining the 2 treatments does not significantly improve ADHD symptoms[, although it may provide added benefit in the event of a comorbid anxiety disorder or oppositional disorder. Until the launch of atomoxetine, stimulant medications were the only medications to receive FDA approval for treatment of ADHD. Atomoxetine is the only medication with FDA approval for management of ADHD in adults. Antidepressants (for all ages) and antihypertensives (in children) are used to treat ADHD that is refractory to treatment with stimulants.
 and antihypertensives (in children) are used to treat ADHD that is refractory to treatment with stimulants.")
45
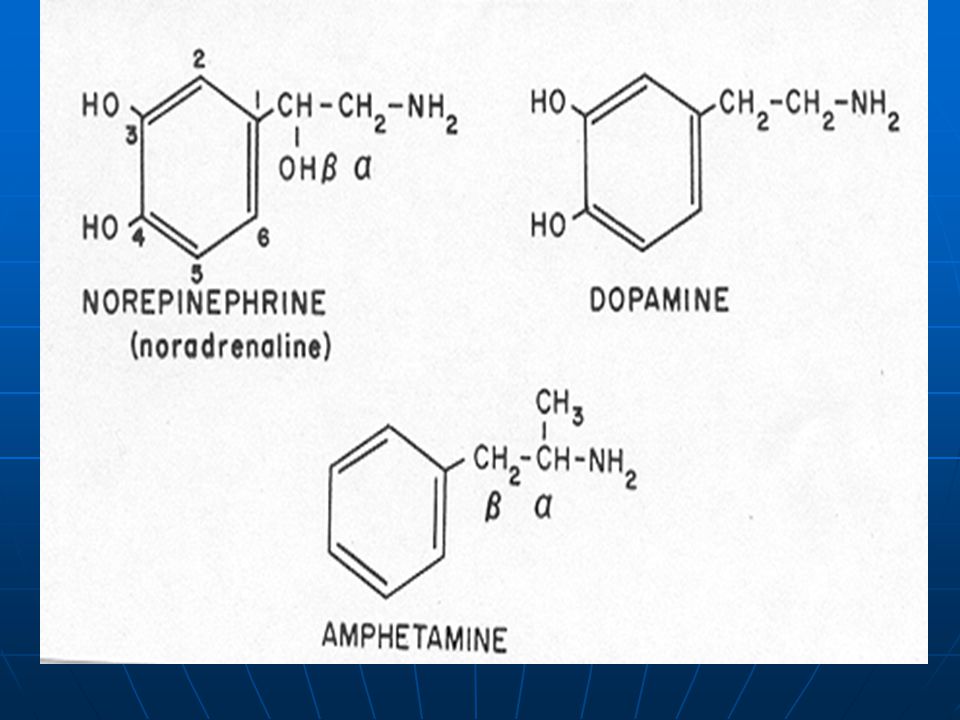
For children and adolescents, a review of therapeutic trials shows a clear pattern of symptom improvement with stimulants, with approximately 70% of patients responding to treatment. Once dosage was adequately titrated for adults, studies showed similar patterns of symptom improvement. ADHD is presumed to stem from dysfunction of the catecholamine system, particularly dopamine and norepinephrine. Stimulants enhance transmission of catecholamines, often by blocking dopamine and norepinephrine reuptake transporters, with the net effect of increasing attention and decreasing impulsivity.

47
Pharmacotherapy Overview

50
Understanding Dopamine Neurotransmission in ADHD
Synaptic terminal Vesicles containing DA DA transporters 3. Dopamine in the synapse is reabsorbed (reuptake) 1. Dopamine is released into the synapse Slide 10: Understanding Dopamine Neurotransmission in ADHD As seen in this slide, dopamine (DA) is stored in vesicles in the presynaptic neuron. Activity in the DA-containing cell causes vesicles to release DA into synaptic space. DA diffuses and binds to receptors on the postsynaptic cell. DA inactivation occurs via diffusion and reuptake by DA transporters as well as by degradation of DA by monoamine oxidase present in the synapse. In ADHD, DA deficiency may be the result of [1] excessive reuptake [2] postsynaptic receptor malfunction and/or [3] a deficiency in the fusion of DA containing vesicles with the plasma membrane leading to a relative deficiency in dopamine availability. Many experts on ADHD believe that the symptoms of ADHD may be the direct result of a deficiency of dopamine and, indirectly, norepinephrine, particularly within the prefrontal cortex.1 Low levels of dopamine would be expected to lead to diminished activity in the affected structures. Underactivity in the prefrontal cortex is associated with many of the symptoms observed in ADHD, as described on the previous slide.2 This theory is supported by studies in which dopamine transporter density was found to be as much as 70% greater in patients with ADHD as compared with normal control subjects.3 In addition, there is evidence of norepinephrine dysregulation in patients with ADHD. The noradrenergic system appears to prime the prefrontal cortex for response to sensory stimuli.1 1Pliszka SR et al. J Am Acad Child Adolesc Psychiatry ;35: 2Barkley RA. Sci Am ;279:66-71. 3Dougherty DD et al. Lancet ;354; 2. Dopamine temporarily attaches to receptors DA receptors Postsynaptic cell Adapted from: Barkley RA. Sci Am ;279:66-71. Pliszka SR et al. J Am Acad Child Adolesc Psychiatry. 1996;35:264–272. Barkley RA. Sci Am. 1998;279:66–71. Dougherty DD et al. Lancet. 1999;354:2132–2133.
 1. Dopamine is released into the synapse. Slide 10: Understanding Dopamine Neurotransmission in ADHD. As seen in this slide, dopamine (DA) is stored in vesicles in the presynaptic neuron. Activity in the DA-containing cell causes vesicles to release DA into synaptic space. DA diffuses and binds to receptors on the postsynaptic cell. DA inactivation occurs via diffusion and reuptake by DA transporters as well as by degradation of DA by monoamine oxidase present in the synapse. In ADHD, DA deficiency may be the result of [1] excessive reuptake [2] postsynaptic receptor malfunction and/or [3] a deficiency in the fusion of DA containing vesicles with the plasma membrane leading to a relative deficiency in dopamine availability. Many experts on ADHD believe that the symptoms of ADHD may be the direct result of a deficiency of dopamine and, indirectly, norepinephrine, particularly within the prefrontal cortex.1 Low levels of dopamine would be expected to lead to diminished activity in the affected structures. Underactivity in the prefrontal cortex is associated with many of the symptoms observed in ADHD, as described on the previous slide.2. This theory is supported by studies in which dopamine transporter density was found to be as much as 70% greater in patients with ADHD as compared with normal control subjects.3 In addition, there is evidence of norepinephrine dysregulation in patients with ADHD. The noradrenergic system appears to prime the prefrontal cortex for response to sensory stimuli.1. 1Pliszka SR et al. J Am Acad Child Adolesc Psychiatry. 1996;35: Barkley RA. Sci Am. 1998;279: Dougherty DD et al. Lancet. 1999;354; Dopamine temporarily attaches to receptors. DA receptors. Postsynaptic cell. Adapted from: Barkley RA. Sci Am. 1998;279: Pliszka SR et al. J Am Acad Child Adolesc Psychiatry. 1996;35:264–272. Barkley RA. Sci Am. 1998;279:66–71. Dougherty DD et al. Lancet. 1999;354:2132–2133.")
52
Dopamine Pathways in ADD

54
Pharmacotherapy Studies including randomized trials have established the efficiency of stimulant medication for alleviating symptoms. Clear indication that medication is more effective than psychosocial therapies. Effect central norepinephrine/dopamine overcoming deficits in inhibitory control and working memory.

55
Pharmacotherapy Effects rapid & appear within 30 minutes
Short half- life fast absorption,metabolism and elimination Peak 1-3 hours- eliminated by 5 hours Sustain release can last up to 9 hours Short term effects well studied need more long term studies One most extensive Klein MD /Mannuzza Studied effects on 226 kids over 16 yrs-no long term adverse outcomes( incl..Growth)
")
56
Dextroamphetamine sulfate /amphetamine sulfate mix
Stimulant Medication /Dosage Form(s) Available Methylphenidate Ritalin 5mg,10mg, and 20mg tablets / Ritalin SR Focalin (d- isomer Methylphenidate) 2.5mg,5mg,10mg Methylphenidate extended release Ritalin LA 20mg,30mg,40mg capsules Metadate CD 10mg and 20-mg capsules /Metadate ER Concerta 18mg, 27mg, 36mg, and 54-mg caplets Methylin / Methylin ER Dextroamphetamine sulfate /amphetamine sulfate mix Adderall 5mg,7.5mg,10mg 12.5mg,15mg, 20mg, 30-mg double-scored tabs Adderall XR 5mg,10mg,15mg,20mg,30mgcapsules Dextroamphetamine Dexedrine 5mg, 10mg, and 15mg sustained release caps Dexedrine( regular) 5mg and 10 mg tablets and Dexedrine 5 mg/ml elixir Dextrostat spansules 5mg 10mg Methamphetamine Desoxyn 5mg tabs Pemoline ( Cylert) mg-, 37.5mg-, 75-mg tablets/ 37.5-mg chewable
 Available. Methylphenidate. Ritalin 5mg,10mg, and 20mg tablets / Ritalin SR. Focalin (d- isomer Methylphenidate) 2.5mg,5mg,10mg. Methylphenidate extended release. Ritalin LA 20mg,30mg,40mg capsules. Metadate CD 10mg and 20-mg capsules /Metadate ER. Concerta 18mg, 27mg, 36mg, and 54-mg caplets. Methylin / Methylin ER. Dextroamphetamine sulfate /amphetamine sulfate mix. Adderall 5mg,7.5mg,10mg 12.5mg,15mg, 20mg, 30-mg double-scored tabs. Adderall XR 5mg,10mg,15mg,20mg,30mgcapsules. Dextroamphetamine. Dexedrine 5mg, 10mg, and 15mg sustained release caps. Dexedrine( regular) 5mg and 10 mg tablets and Dexedrine 5 mg/ml elixir. Dextrostat spansules 5mg 10mg. Methamphetamine. Desoxyn 5mg tabs. Pemoline ( Cylert) 18.75mg-, 37.5mg-, 75-mg tablets/ 37.5-mg chewable.")
57
November 2002, atomoxetine (Strattera) was the first medication approved by the Food and Drug Administration (FDA) for the treatment of ADHD, not just for children and adolescents, but specifically for adults as well This is the first medication to receive an FDA indication for treatment of ADHD in adults, and in fact the initial clinical trials were done in adults rather than children. Atomoxetine is a highly selective norepinephrine reuptake inhibitor that lacks cardiovascular toxicity. Atomoxetine does not have abuse potential, minimizing the likelihood that it would be sold as a street drug. Therefore, unlike the stimulants,It is not classified as a controlled substance and does not require a special prescription.

58
Atomoxetine has been shown to alleviate both inattentive and hyperactive symptoms in ADHD, with good tolerability and few adverse events. The dose ranges from 1.2 to 1.8 mg/kg/day in children and between 60 and 120 mg/day for adults greater than 70K. The drug is rapidly absorbed, with a half-life of 5 hours. Atomoxetine is a highly selective norepinephrine reuptake inhibitor that has a mechanism of action different than the stimulant drugs, making it unique among medications approved for the treatment of ADHD. Some understanding of the mechanism of action is valuable, as it will clarify issues relating to efficacy, tolerability, and side effects.

60
Atomoxetine is a potent inhibitor of presynaptic norepinephrine reuptake. Bymaster and colleagues performed an experiment using rat prefrontal cortex brain tissue to identify atomoxetine receptor affinity and, simultaneously, demonstrate the brain area of greatest activity. Atomoxetine was shown to have an affinity to norepinephrine but minimal affinity for serotonin (5-HT) or dopamine transporters and neuronal receptors. Extracellular concentrations of norepinephrine and dopamine were increased 3-fold by atomoxetine In the prefrontal cortex (ie, the key region for executive function, including attention and memory), in a dose-dependent manner, but did not alter 5-HT levels or significantly affect dopamine outside of the prefrontal cortex. Furthermore, atomoxetine was tested on over 60 other neuronal receptors, transporters, and binding sites, without finding any significant affinity.
 or dopamine transporters and neuronal receptors. Extracellular concentrations of norepinephrine and dopamine were increased 3-fold by atomoxetine. In the prefrontal cortex (ie, the key region for executive function, including attention and memory), in a dose-dependent manner, but did not alter 5-HT levels or significantly affect dopamine outside of the prefrontal cortex. Furthermore, atomoxetine was tested on over 60 other neuronal receptors, transporters, and binding sites, without finding any significant affinity.")
61
In contrast to atomoxetine, the researchers found that methylphenidate had a higher affinity for dopamine transporters than for norepinephrine transporters. Like atomoxetine, methylphenidate increased extracellular norepinephrine and dopamine equally in prefrontal cortex, but it also increased dopamine in the striatum and nucleus accumbens to the same level as in the prefrontal cortex. Interestingly, atomoxetine exhibited only small increases in dopamine in the striatum and nucleus accumbens, which are the areas of greatest concentration of dopamine transporters. Stimulants are known to work via dopaminergic neuronal pathways leading from the brain stem to the nucleus accumbens, producing positive reinforcement. The fact that atomoxetine does not increase dopamine in this region may relate to the demonstrated a lack of abuse potential

62
The most common drug-related event reported across trials has been gastrointestinal effects, such as nausea. A decrease in appetite is experienced by 15% to 20% of patients, with an initial period of weight loss that seems to appear early in treatment and then declines. Atomoxetine has also been associated with slight increases in diastolic blood pressure and heart rate, but no effects were seen on cardiac conduction or the QTc interval. The mild cardiac effects are comparable to the effects reported with stimulants and ADHD medications should be used with caution with patients at risk of hypertension.

63
STRATTERA should not be taken with an MAOI, or within 2 weeks after discontinuing an MAOI. Treatment with an MAOI should not be initiated within 2 weeks after discontinuing STRATTERA. With other drugs that affect brain monoamine concentrations, there have been reports of serious, sometimes fatal, reactions (including hyperthermia, rigidity, myoclonus, autonomic instability with possible rapid fluctuations of vital signs, and mental status changes that include extreme agitation progressing to delirium and coma) when taken in combination with an MAOI. Some cases presented with features resembling neuroleptic malignant syndrome. Such reactions may occur when these drugs are given concurrently or in close proximity.

64
Albuterol --STRATTERA should be administered with caution to patients being treated with systemically-administered (oral or intravenous) albuterol (or other beta 2 agonists) because the action of albuterol on the cardiovascular system can be potentiated. CYP2D6 inhibitors --Atomoxetine is primarily metabolized by the CYP2D6 pathway to 4-hydroxyatomoxetine. In EMs, selective inhibitors of CYP2D6 increase atomoxetine steady-state plasma concentrations to exposures similar to those observed in PMs. Dosage adjustment of STRATTERA may be necessary when coadministered with CYP2D6 inhibitors, e.g., paroxetine, fluoxetine, and quinidine

65
The various stimulant formulations seem to be quite similar in their efficacy. However, the short half-life of the original formulations required multiple daily dosing. In recent years, long-acting formulas have been put on the market, ameliorating the stigma, inconvenience, noncompliance, and rebound associated with a short duration of action. The newer extended-release agents are effective for as long as 10 to 12 hours, yet some patients are still requiring additional short-acting stimulants to extend their treatment time. The current doses that are available are often too low for adults, requiring them to take several pills and sometimes this means paying considerably more for the medication or having the needed dose refused by the insurer.

66
Methylphenidate vs Amphetamine
Absorption Acidic foods limit absorption Readily absorbed; independent of pH Distribution Low plasma protein binding Metabolism pH of urine determines degree of hepatic clearance Moderate P450 metabolism, some CYP2D6 Presystemic metabolism limits oral bioavailability Little P450 metabolism; no CYP2D6 metabolism Elimination Acidic urine results in decreased plasma half-life and increased renal clearance Shows up on routine drug testing Elimination of MPH metabolites unaffected by urinary pH Does not show up on routine drug testing

67
Newer Stimulants Vyvanse (lysamphetamine)
-dosages 10 ,20,30,40,60,70 mg ZENZEDI -dosages 5mg, 7.5mg, 10mg. Quillivant liquid MPD 10ml = 4 mg

68
Selection of the Optimal Dose Ratio for Metadate® CD
1Wigal et al. J Appl Res 2003;3:46-63

69
Biphasic Release Pattern of Metadate® CD Capsules
1Metadate® CD (methylphenidate HCl, USP) Extended-Release Capsules, full Prescribing Information. Celltech Pharmaceuticals, Inc, Rochester, NY; R312D (07/03) 2Wigal et al. J Appl Res 2003;3:46-64
 Extended-Release Capsules, full Prescribing Information. Celltech Pharmaceuticals, Inc, Rochester, NY; R312D (07/03) 2Wigal et al. J Appl Res 2003;3:")
70
Generally, stimulant medications are well tolerated
Generally, stimulant medications are well tolerated. Side effects from stimulants include insomnia, headaches, weight loss or anorexia, tics, anxiety, and dysphoria. Cardiovascular effects typically involve only mild increases in heart rate and blood pressure, but need to be more closely watched in adults than in children .Adults who present with borderline hypertension may not be able to tolerate even a mild increase. In this circumstance the hypertension should be treated before stimulant is reinstituted. Insomnia is common for adults with ADHD both before and after initiation of a course of a stimulant. A delay in sleep onset may decrease with longer administration of the medication. Stimulant medication is initially administered by titrating the dose until symptoms are well controlled and, concurrently, side effects are manageable for the patient.

71
Both methylphenidate and dextroamphetamine are C-II controlled substances and much has been written in medical and popular literature about their potential for abuse, necessitating clarity on the issue. An adult who suffers from ADHD, uses the medication as prescribed, and does not concurrently have a substance abuse problem will not become addicted. There are reports of stimulant medication prescribed medically being diverted for nonmedical recreational use. Clinicians should therefore be circumspect in prescribing medication to patients with current substance abuse, or whom they suspect might sell the drug. Interestingly, some studies offer intriguing evidence that stimulant treatment of ADHD does decrease the risk of future substance abuse, including cocaine use, among adult ADHD sufferers.

72
Key points: Pharmacotherapy is a central element in the treatment of ADHD, and some studies have shown it to be more effective than behavioral treatment in reducing the symptoms of ADHD. Stimulants increase dopamine and norepinephrine levels in the synapse, ameliorating symptoms associated with ADHD in about 70% of patients. Side effects from stimulants can include hypertension, insomnia, headaches, weight loss or anorexia, tics, anxiety, and dysphoria. When prescribed and taken appropriately for the treatment of ADHD, stimulant medication is not addictive. Care should be taken when using stimulants to treat patients with a comorbid substance abuse disorder.

73
Other Stimulant Medications
Desoxyn (Methamphetamine Hcl) Adipex-P (Phenteraimine) Didex (Benzphetamine) Tenuate (Diethylpropion Hcl) Mazindol (Imidazoisoindol) Phenazine (Phendimetrazine Tartarate) Dopram (Doxapram Hcl)
 Adipex-P (Phenteraimine) Didex (Benzphetamine) Tenuate (Diethylpropion Hcl) Mazindol (Imidazoisoindol) Phenazine (Phendimetrazine Tartarate) Dopram (Doxapram Hcl)")
74
Alpha 2 adrenergic agonists
Clonidine Adverse effects, sedating, hypotension Guaifenesin Adverse effects - few & less sedating *Both are often used in combination with other medications to augment treatment.

75
Antidepressants Prozac Paxil Zoloft Tofranil Effexor SR Lexapro
Desipramine (Norpramin), a tricyclic antidepressant that blocks norepinephrine and serotonin uptake, and bupropion (Wellbutrin), an antidepressant with greater dopamine reuptake block than most antidepressants, have been shown to have some effectiveness in treatment of ADHD. Prozac Paxil Zoloft Tofranil Effexor SR Lexapro Generally Maximum benefit in co- morbidity
, a tricyclic antidepressant that blocks norepinephrine and serotonin uptake, and bupropion (Wellbutrin), an antidepressant with greater dopamine reuptake block than most antidepressants, have been shown to have some effectiveness in treatment of ADHD. Prozac. Paxil. Zoloft. Tofranil. Effexor SR. Lexapro. Generally Maximum benefit in co- morbidity.")
76
Melatonin Melatonin may be helpful for treating delayed sleep onset in children with attention deficit-hyperactivity disorder (ADHD), Since melatonin is in an unusual category, being an unpatentable hormone considered in the U.S. to be a 'nutritional supplement' that is unregulated by the [Food and Drug Administration], and since there is evidence that some brands contain other than 'pharmaceutically pure' melatonin, evidence of safety and efficacy is of great importance to clinicians

77
Repetitive Transcranial Magnetic Stimulation (rTMS): New Tool, New Therapy and New Hope for ADHD
Transcranial magnetic stimulation (TMS) is a newly developed tool for assessing functionality of the central nervous system (CNS). After Baker et al. demonstrated its value in humans in 1985, single and paired-pulse TMS have proven useful in detecting clinical and subclinical abnormalities in a large array of neurological and neuropsychiatric disorders including Tourette's syndrome, obsessive compulsive disorder, depression, schizophrenia, bipolar disorders and ADHD among others. Regarding ADHD specifically, TMS seems to be an ideal method for studying the maturational process of the motor pathways since it clearly excites the corticomotoneuronal system presumed to be involved in this disorder.
 is a newly developed tool for assessing functionality of the central nervous system (CNS). After Baker et al. demonstrated its value in humans in 1985, single and paired-pulse. TMS have proven useful in detecting clinical and subclinical abnormalities in a large array of neurological and neuropsychiatric disorders including Tourette s syndrome, obsessive compulsive disorder, depression, schizophrenia, bipolar disorders and ADHD among others. Regarding ADHD specifically, TMS seems to be an ideal method for studying the maturational process of the motor pathways since it clearly excites the corticomotoneuronal system presumed to be involved in this disorder.")
78
Using single stimulation in children with ADHD, found a prolongation of central motor conduction time as well as some side-to-side stimulation differences compared with those found in age- and sex-matched controls. These findings demonstrated a delay in the maturation of the corticomotoneuronal system in patients with ADHD. Moll et al.[11] reported that children with ADHD had significantly reduced intracortical inhibition (ICI) with a normal intracortical facilitation compared to healthy controls and such ICI showed improvement after giving 10 mg of MPH. However, most of the morphophysioneurochemical hallmarks of ADHD involving prefrontal-caudate-cerebellar pathways with noteworthy dopaminergic abnormalities have not yet been taken into account. Therefore we consider that they should be the current focus if rTMS is to be employed as a therapeutic option.
 with a normal intracortical facilitation compared to healthy controls and such ICI showed improvement after giving 10 mg of MPH. However, most of the morphophysioneurochemical hallmarks of ADHD involving prefrontal-caudate-cerebellar pathways with noteworthy dopaminergic abnormalities have not yet been taken into account. Therefore we consider that they should be the current focus if rTMS is to be employed as a therapeutic option.")
79
rTMS has been found effective in Parkinson disease, depression, obsessive-compulsive disorder, Tourette's syndrome and some types of tic. With regard to children rTMS has been tried with a small number of patients with action myoclonus, progressive myoclonic epilepsy, bipolar disorder, major depression and schizophrenia with some promising, albeit, short-lasting positive results. Some of these disorders are due to dopamine abnormalities and share some genetic, clinical, biochemical, neuranatomical and neuro-behavioural similarities with ADHD. Even though a complete understanding of the mechanism of action of rTMS has not been developed, it is now clear that rTMS at low frequencies could cause long-term depression of cortico-cortical transmission in normals as well as improvement of symptoms of some neuropsychiatric disorders commented on above, including the modulation of several neurotransmitters such as dopamine and its metabolites (e.g. homovanilic acid) mainly after prefrontal cortex stimulation.
 mainly after prefrontal cortex stimulation.")
80
Some safety issues must be considered in some of patients since there is a limited experience of possible side-effects in children and adolescents using TMS particularly rTMS.[] Even though muscle-tension headache that resolved promptly is the only only side-effect found in children receiving rTMS, Tis still concern in applying it with pulse frequencies of 50 Hz or more for periods of several seconds because of the possiblity of seizures. At present, there is no reason for applying rTMS at higher frequencies, intensities or with longer train durations than those employed in clinical or research studies. Thus, frequencies lower than 50 Hz might be used with some confidence in humans until new safety guidelines on rTMS applications can be published
![Some safety issues must be considered in some of patients since there is a limited experience of possible side-effects in children and adolescents using TMS particularly rTMS.[] Even though muscle-tension headache that resolved promptly is the only only side-effect found in children receiving rTMS,](http://slideplayer.com/slide/2366686/8/images/80/Some+safety+issues+must+be+considered+in+some+of+patients+since+there+is+a+limited+experience+of+possible+side-effects+in+children+and+adolescents+using+TMS+particularly+rTMS.%5B%5D+Even+though+muscle-tension+headache+that+resolved+promptly+is+the+only+only+side-effect+found+in+children+receiving+rTMS%2C.jpg "Tis still concern in applying it with pulse frequencies of 50 Hz or more for periods of several seconds because of the possiblity of seizures. At present, there is no reason for applying rTMS at higher frequencies, intensities or with longer train durations than those employed in clinical or research studies. Thus, frequencies lower than 50 Hz might be used with some confidence in humans until new safety guidelines on rTMS applications can be published.")
81
Treatment Triangle P Child T D

82
ADHD Parent Information & education Child management skills School
Evaluation / PPT (Pupil Placement Team) Teacher training / Special education School Nurse Doctor Diagnosis Information & treatment
 Teacher training / Special education. School Nurse. Doctor. Diagnosis. Information & treatment.")
83
ADHD Role of School Evaluation-medical & psychological
PPT (Pupil Placement Team) Learning Disability definition & placement Teacher Training in ADHD Teacher documentation( changes with treatment, feedback to Parents etc) School Nurse -medication documentation & dispensation
 Learning Disability definition & placement. Teacher Training in ADHD. Teacher documentation( changes with treatment, feedback to Parents etc) School Nurse -medication documentation & dispensation.")
84
ADHD Contingency management : point token, reward systems- time out
Cognitive Behavioral training (self monitoring,verbal self instruction solving strategies, self reinforcement) Parent training /child management skills
 Parent training /child management skills.")
86
Adult ADD

87
Hallmark characteristics of attention-deficit hyperactivity disorder (ADHD) include hyperactivity, impulsiveness, and inattentiveness. Research has established that ADHD, still the most common psychiatric disorder in children, can persist not only through adolescence but into adulthood as well. While ADHD can remit, an estimated 30% to 70% of childhood ADHD cases continue into adulthood. However, much of what we know about ADHD comes from the wealth of research that has been collected on its manifestations In childhood. Increasingly, evidence points to a developmental shift in the presentation of ADHD in adults. This shifting profile may well have resulted in underdiagnosis of adult cases of ADHD.

88
ADHD is a developmental disorder, which by definition must have been present from childhood. Many of these adults may not have had the opportunity to be assessed or diagnosed, since ADHD services and expertise may not have been available. More recently investigators have shifted their focus of interest towards understanding the nature of attention problems and the executive functions. Executive function refers to skills such as working memory, planning, prioritization, organization, and time management. The theory holds that the prefrontal lobes, which are associated with memory, motivation, and synthesis of behavior, are the site of the brain's executive function and regulate behavior via a process of inhibition. Advances in neuro imaging technology and the development of neuropsychological assessments have permitted researchers to measure and quantify executive function in adults with ADHD as compared with controls.

89
Many of the associated symptoms of ADHD involve dysregulation of sleep, appetite, energy, and mood that are easily understood within the framework of mood disorders with which adult psychiatrists are more familiar. Most patients with ADHD also have another comorbid disorder. The adult psychiatrist may attribute the patient's impairment to the comorbid disorder more familiar to him (ie, anxiety disorder, bipolar II disorder, or personality disorder) and miss the contribution of the ADHD. Some of the comorbid disorders that accompany ADHD are developmental disorders in their own right that adult psychiatrists do not recognize such as Asperger's syndrome, learning disabilities, Tourette's syndrome, or oppositional defiant disorder
 and miss the contribution of the ADHD. Some of the comorbid disorders that accompany ADHD are developmental disorders in their own right that adult psychiatrists do not recognize such as Asperger s syndrome, learning disabilities, Tourette s syndrome, or oppositional defiant disorder.")
90
The research that identified the continued prevalence of ADHD in adults had also identified a pattern of lifelong adaptive functioning difficulties. The maladaptive patterns might manifest with or without comorbidities -- each topic will be covered in sections to follow. What began as a problem functioning in the classroom and playground became persistent social and vocational troubles, if not failures. Research has demonstrated that adult ADHD is associated with functional impairments that result in an array of problematic behaviors, such as increased traffic accidents and violations, difficulty with smoking, educational and occupational impairment and marital problems.[ ] In addition, ADHD was shown to predict specific disorders in adulthood, such as antisocial behavior and substance abuse.[11] Given the studies showing that patients who receive pharmacological treatment have an 85% reduction in risk for substance abuse, it is unfortunate that establishing validity of ADHD in adults was so lengthy a process.

91
Key points: It is well established that ADHD affects some individuals across their lifespan. Prospective studies illustrate that adults diagnosed with ADHD as children retained at least one ADHD symptom into adulthood. Sequelae of ADHD may continue to impair the lives of individuals with ADHD throughout adulthood, particularly those who have not received treatment.

93
Key points: Hyperactivity tends to decrease with age, while problems with sustained attention persist and predominate the symptom profile in many adults. Adults exhibit impairments in the brain's executive function both at home and at the workplace. While all 3 core symptoms can persist over a lifetime, adults with ADHD may have more attenuated symptoms that are expressed in manners different from children

94
It is estimated that nearly 75% of adults with ADHD have a comorbid condition, with reports ascertaining that 77% of this population has had at least 1 of 17 comorbid psychiatric disorders. Comorbidity immeasurably complicates the diagnosis of ADHD and, as will be discussed in the section on diagnosis, is not excluded for an accurate diagnosis of ADHD, according to DSM-IV criteria. The inclusive standard is likely based on an accumulation of research, Indicating that the comorbidities are indeed discrete conditions in their own right. As one group of researchers states, "among adults, ADHD does not appear to be an artifact of symptoms shared with other psychiatric disorders (eg, major depression, bipolar disorder, generalized anxiety disorder) nor are the comorbidities themselves the result of symptomatic overlap with ADHD.
 nor are the comorbidities themselves the result of symptomatic overlap with ADHD.")
95
Key points: Approximately 75% of adults with ADHD have at least 1 comorbid condition. Learning disabilities and disruptive behavior disorders are the 2 comorbid conditions most prevalent in childhood. Adults with ADHD are at considerable risk for substance abuse (especially marijuana), and smoking, but this risk is diminished by appropriate treatment. Mood and anxiety disorders are significant comorbidities among adults with ADHD but more research is needed to determine their prevalence.
, and smoking, but this risk is diminished by appropriate treatment. Mood and anxiety disorders are significant comorbidities among adults with ADHD but more research is needed to determine their prevalence.")
96
While researchers may disagree about age of childhood onset in diagnosing adult ADHD, all agree that ADHD is not an adult-onset disorder and must be verified from childhood. An assessment of ADHD symptoms and behavior from childhood may include any or all of the following: The Wender Utah Rating Scale (WURS) is designed to measure whether the adult had ADHD in childhood. School report cards, if available, might include comments about behavior problems, poor focus, lack of effort, or underachievement relative to the student's potential. Parents may serve as collateral informants and complete an ADHD scale with respect to the individual's symptoms in childhood. The adult may self report symptoms in childhood on a diagnostic interview or on an ADHD scale completed for childhood symptoms.] The developmental history would be consistent with ADHD, including evidence of problems with peers, other delays such as enuresis, school failure, suspensions, or special interventions such as sitting in front of the class, etc.
 is designed to measure whether the adult had ADHD in childhood. School report cards, if available, might include comments about behavior problems, poor focus, lack of effort, or underachievement relative to the student s potential. Parents may serve as collateral informants and complete an ADHD scale with respect to the individual s symptoms in childhood. The adult may self report symptoms in childhood on a diagnostic interview or on an ADHD scale completed for childhood symptoms.] The developmental history would be consistent with ADHD, including evidence of problems with peers, other delays such as enuresis, school failure, suspensions, or special interventions such as sitting in front of the class, etc.")
97
Symptom rating scales. Conners Adult ADHD Rating Scale -- available either in 26- or 42-item version, perhaps the best scale available to discriminate between patients with ADHD and those with other conditions; internal reliability and validity ratings are high (available from Multi-Health Systems at mhs.com). DSM-IV-based rating scales list the 18 items of DSM-IV ADHD (and sometimes those for oppositional defiant disorder and conduct disorder as well) along with a 4 point scale. The patient rates each item as: 0. Not at all or never 1. Somewhat or sometimes 2. Pretty much or often 3. Very much or very often Scores of 2 or 3 are usually considered to be in the clinical range. If 6/9 items of inattention and/or hyperactive/impulsive symptoms are rated 2 or 3 this would be considered to have met the DSM-IV categorical cutoff. Several versions of this scale are available, and 1 is available on the net. Barkley has adapted this scale for use with adults.
. DSM-IV-based rating scales list the 18 items of DSM-IV ADHD (and sometimes those for oppositional defiant disorder and conduct disorder as well) along with a 4 point scale. The patient rates each item as: 0. Not at all or never 1. Somewhat or sometimes 2. Pretty much or often 3. Very much or very often. Scores of 2 or 3 are usually considered to be in the clinical range. If 6/9 items of inattention and/or hyperactive/impulsive symptoms are rated 2 or 3 this would be considered to have met the DSM-IV categorical cutoff. Several versions of this scale are available, and 1 is available on the net. Barkley has adapted this scale for use with adults.")
98
Neuropsychological assessments were initially developed for children and established that children evidenced clinically significant deficits in executive functioning, even when IQ scores were above average. Neuropsychological assessments performed on adults with ADHD reveals deficits in speed, memory, and attention. However, research on these measurements demonstrates that the spectrum of deficit functions associated with ADHD is not consistent across the various neuropsychological tests available for adults. Therefore, neuropsychological testing of adults may contribute to an overall evaluation but, again, should not be used as the sole diagnostic instrument. The same is true for computerized tests of attention such as the Continuous Performance Test (CPT) or Test of Visual Attention (TOVA).
 or Test of Visual Attention (TOVA).")
99
Compared with children who have problems in both cognitive and behavioral control, adults with ADHD have greater deficits in the use of executive functions relating to cognitive control. As the years pass, the 3 core dimensions of the disorder do persist in some form.[] However, the demands on the brain's executive function to regulate, organize, and manage behaviors both at home and at the workplace become ever more complex. Experts suggest that failure of the brain's executive functions is 1 of the most prominent attributes in adult ADHD.

101
Hyperactivity -- not excessive action itself, but the inability to control arousal and amount of activation Inattentiveness -- not a global inability to focus per se, but rather the inability to sustain, shift, and establish attention to particular tasks the individual finds boring but are nonetheless essential to adult functioning Impulsiveness -- no longer the inability to control actions, but the inability to determine when and how actions should be expressed and sequenced, and continued environmental dependency where circumstances control action, rather than the other way around

102
Cognitive Therapy

103
Cognitive Therapy

104
CONSCIOUSNESS GOAL FOCUS “Now” Requirement “Stray” Deflection
‘Thought” Potentials

105
GOAL Nebula

109
Plague

114
Relationship between Add
& Lunar Ecllipse ? NO!!

Similar presentations


























>")
 By: Bianca Jimenez Period:5.>")
. Diagnostic and.>")

 is one of the most common childhood disorders and can continue.>")







