Download presentation
Presentation is loading. Please wait.

1
Public Health and Human Rights: Challenges, Synergies, Methodologies June 22 nd, 2008 Chris Beyrer MD, MPH Center for Public Health and Human Rights Johns Hopkins Bloomberg School of Public Health

2
Core Themes Human rights abrogation or protection can have profound impacts on the health of individuals, communities, and populations Rights violations which affect populations need to be investigated and addressed using population-based methods Responses based on human rights principles may improve disease prevention and control, and better the human rights contexts for those at dual risk

3
Outline I.Introduction II.Health rights and human rights III.Putting PHHR into practice Luke Mullany, PhD

4
Introduction Modern human rights movement a response to Nazi atrocities of WWII Universal Declaration of Human Rights passed by United Nations on December 10, 1948 – Defines the fundamental human rights of persons and violations of those rights – Universalist – Aspirational – Lacking enforcement mechanisms

5
UDHR Resolutions include: Article 4: Prohibits slavery Article 5: Prohibits torture Article 18: Freedom of thought Article 19: Freedom of opinion and of expression Article 25: Standard of Living – Includes access to medical care as a human right

6
Human Rights Instruments and Public Health 1948 The Universal Declaration of Human Rights 1976 International Covenant on Civil and Political Rights 1976 International Covenant on Economic, Social and Cultural Rights General Comment 14: Health rights Prevention, treatment, control of epidemic diseases Focus on realizing rights of women to health throughout the life span 1981 Convention on the Elimination of All Forms of Discrimination against Women (CEDAW) Health services to be consistent with the human rights of women: Autonomy, Privacy, Confidentiality, Informed consent, and Choice
 Health services to be consistent with the human rights of women: Autonomy, Privacy, Confidentiality, Informed consent, and Choice")
7
State Responsibilities Signatory States must not violate these rights Commit to measurable progress to: Respect Protect Fulfill

8
What is meant by “ The Right to Health ” “ The right to health does not mean the right to be healthy, nor does it mean poor governments must put in place expensive health services for they have no resources. But it does require authorities put in place policies and action plans which lead to available and accessible health care for all in the shortest possible time. To ensure that this happens is the challenge facing both the human rights community and public health professionals. ” UN High Commissioner for Human Rights, Mary Robinson

9
The Center for Public Health and Human Rights at Hopkins Focus is the impact of rights of violations on the health of populations Research, Teaching, Advocacy Use of population based methods (epidemiology) to study, document, measure these impacts Bring increased awareness of human rights and health interactions to the scientific community Enhance public health through rights based interventions Advocate for public health and human rights
 to study, document, measure these impacts Bring increased awareness of human rights and health interactions to the scientific community Enhance public health through rights based interventions Advocate for public health and human rights")
10
PHHR Center Activities Burma: Cross border health and rights projects with ethnic minority health groups (IDPs, migrants); HIV/AIDS epi; Mobile Obstetric Medics (Gates Inst.); Capacity building for human rights and democracy (DOS) Southern Africa: MSM, HR, and HIV (OSI) Russia: MSM, HR, and HIV (Ford, NIH) China: Treatment access and advocacy for blood donors (OSI, Levi Strauss) Kazakhstan, Kyrgyzstan: HIV prevention, NSEPs, HIV VCT access (NIH/NIMH, NIDA)
; HIV/AIDS epi; Mobile Obstetric Medics (Gates Inst.); Capacity building for human rights and democracy (DOS) Southern Africa: MSM, HR, and HIV (OSI) Russia: MSM, HR, and HIV (Ford, NIH) China: Treatment access and advocacy for blood donors (OSI, Levi Strauss) Kazakhstan, Kyrgyzstan: HIV prevention, NSEPs, HIV VCT access (NIH/NIMH, NIDA)")
11
JHU Press, 2007

12
Human rights violations and associations with population-level health indicators June 22 nd, 2008 Luke C. Mullany, PhD MHS Center for Public Health and Human Rights Johns Hopkins Bloomberg School of Public Health

13
Population – 50 million Ethnically diverse 90% Buddhist Military junta (SPDC) Poor health indicators –IMR: 76/1000 –U5MR: 104/1000 –WFP: 33% of children chronically malnourished –WHO: 190 / 191 ranking for health system Burma
 Poor health indicators –IMR: 76/1000 –U5MR: 104/1000 –WFP: 33% of children chronically malnourished –WHO: 190 / 191 ranking for health system Burma")
14
Human rights violations Forced labor Destruction / seizure of crops / livestock Arbitrary arrest and detention Forced military conscription Torture, rape, execution “ Four cuts ”

15
Backpack Health Worker Team Novel approach to data collection within internally displaced populations –Programmatic context –IDPs actively gathering information among themselves Workers also specific targets of the conflict

16
Data collection activities Health information systems developed over past 10 years with tech. asst. from CPHHR and Global Health Access Program (www.ghap.org)www.ghap.org Major goal: estimation of mortality –U5MR / IMR through surveys –Tracking of human rights violations Others: –Morbidity estimation –Compliance with specific programs –Knowledge / practices / attitudes

17
Methods - Design Retrospective household surveys –Reporting of vital events –12 month recall period Sampling –Two stage cluster design –100 clusters –20 households / cluster

18
Methods - Design Cluster selection: –Village based –Selection proportionate to population size –Census provides complete lists of population by village Household selection – various methods used – “ spin the pen ”, random-proximity method –Interval sampling with random start

19
Survey elements Context demands simplicity –Constant movement by interviewers –Travel on foot –One page limit Household census All deaths recorded (cause) Listing by age / sex
 Listing by age / sex")
20
Results – Sample Response rate has varied: 70-92% Total sample 7,500-9,000 –(5-6 persons / household) <5 years old ~ 18-20% <15 years old ~ 45 – 50% Male to female ratios – consistently <0.9
 <5 years old ~ 18-20% <15 years old ~ 45 – 50% Male to female ratios – consistently <0.9")
21
Population pyramid - 2004 900 800 700 600 500 400 300 200 100 0 200 300 400 500 600 700 800 900 Age Group 95-100 90-95 85-90 80-85 75-80 70-75 65-70 60-65 55-60 50-55 45-50 40-45 35-40 30-35 25-30 20-25 15-20 10-15 5-10 0-5 Males Females Male to Female Ratio 15-25yrs: 0.86 Mullany LC, Richards AK, Lee CI, et al. Application of population-based survey methodology to quantify associations between human rights violations and health outcomes in eastern Burma. J Epidemiol Community Health. 2007;61:908-14

22
Lee TJ, Mullany LC, Richards AK, et al. Mortality rates in conflict zones in Karen, Karenni, and Mon states in eastern Burma. Trop. Med. Int. Health. 2006;11(7):1119-27. Mullany LC, Richards AK, Lee CI, et al. Application of population-based survey methodology to quantify associations between human rights violations and health outcomes in eastern Burma. J Epidemiol Community Health. 2007;61:908-14.
: Mullany LC, Richards AK, Lee CI, et al. Application of population-based survey methodology to quantify associations between human rights violations and health outcomes in eastern Burma. J Epidemiol Community Health. 2007;61:")
23
Lee TJ, Mullany LC, Richards AK, et al. Mortality rates in conflict zones in Karen, Karenni, and Mon states in eastern Burma. Trop. Med. Int. Health. 2006;11(7):1119-27.
:")
24
Impact of human rights violations? Overall, mortality rates represent a non- specific, indirect relationship only Evidence –Violence-related deaths, especially landmine –Preponderance of malaria deaths –Male / female ratio Families of former rebels Angola (80:100) Afghan refugees in Pakistan (88:100)
 Afghan refugees in Pakistan (88:100).")
25
Indirect, or ecological inference regarding impact of conflict Compare likelihood of 1 or more deaths of live born children Areas under “ Four-Cuts ” policy vs. “ Cease-Fire ” areas –Four Cuts: 39.9% –Cease Fire:16.6% –PRR = 2.40 (2.02 – 2.86)
.")
26
Measure HRV and health directly? Documentation of human rights violations comes largely from legalistic tradition Use classical epidemiological tools to quantify associations BPHWT structure and experience provided important opportunity to directly link HRV to health outcomes

27
Linking Morbidity and Mortality to Human Rights Backpack medics added short set of questions to health surveys –6 questions –household level –past 12 months recall period Secondary data analysis of this existing data to quantify associations between HRV and health outcomes

28
Sample Questions In the past 12 months, how many people, from your household: –were forced to work against their will –were shot at, stabbed, or beaten by a soldier –had a landmine or UXO injury In the past 12 months, how many times has your household: –Had the food supply (including rice field, paddy, food stores, and livestock) been taken or destroyed? –Been forcibly displaced or moved due to security risk?

29
Prevalence of human rights violations, 2004 Mullany LC, Richards AK, Lee CI, et al. Application of population-based survey methodology to quantify associations between human rights violations and health outcomes in eastern Burma. J Epidemiol Community Health. 2007;61:908-14. Violation / Event % of Households Forced Labor32.6% Forced Displacement8.9% Food Destruction / Theft25.2% Landmine Injuries1.3% Multiple rights violations14.4%

30
Infant mortality: OR=1.72 (0.52 – 5.74) Child mortality: OR=2.80 (1.04, 7.54) Landmine injury: OR=3.89 (1.01 – 15.0) Child malnutrition: OR=3.22 (1.74 – 5.97) Malaria parasitemia: OR=1.58 (0.97 – 2.57) Families forced to move have higher odds of poor health outcomes: Mullany LC, Richards AK, Lee CI, et al. Application of population-based survey methodology to quantify associations between human rights violations and health outcomes in eastern Burma. J Epidemiol Community Health. 2007;61:908-14.

31
Child mortality: OR=1.19 (0.67 – 2.15) Crude mortality: OR=1.58 (1.09, 2.29) Landmine injury: OR=4.55 (1.23 – 16.9) Child malnutrition: OR=1.94 (1.20 – 3.14) Malaria parasitemia: OR=1.82 (1.16 – 2.89) Families reporting theft/destruction of their food supply have higher odds of poor health outcomes: Mullany LC, Richards AK, Lee CI, et al. Application of population-based survey methodology to quantify associations between human rights violations and health outcomes in eastern Burma. J Epidemiol Community Health. 2007;61:908-14.

32
Child mortality: IRR=2.18 (1.11 – 4.29) Crude mortality: IRR=1.75 (1.14, 2.70) Landmine injury: IRR=19.8 (2.59 – 151.2) Malaria parasitemia: IRR=2.34 (1.27 – 4.32) Families reporting three or more violations: –Child mortality: IRR = 5.23 (1.93 – 14.4) Exposure to multiple rights violations: Mullany LC, Richards AK, Lee CI, et al. Application of population-based survey methodology to quantify associations between human rights violations and health outcomes in eastern Burma. J Epidemiol Community Health. 2007;61:908-14.

33
Mobile Obstetric Medics (MOM) Providing essential maternal health services in the conflict zones in Eastern Burma Karen, Karenni, Mon, Shan ethnic teams, Mae Tao Clinic (Dr. Cynthia Maung), Hopkins, UCLA Cross border MCH program –Family planning, ANC and PNC care –Bringing Emergency Obstetric care to the household level Supported by Bill & Melinda Gates Institute for Population and Reproductive Health at Johns Hopkins
, Hopkins, UCLA Cross border MCH program –Family planning, ANC and PNC care –Bringing Emergency Obstetric care to the household level Supported by Bill & Melinda Gates Institute for Population and Reproductive Health at Johns Hopkins.")
34
Mobile teams carrying medical supplies to IDP Communities, Eastern Burma, 2007. The Mobile Obstetric Medic Project

35
Baseline Survey Results Access to attendant with ability to deliver component low: 5.1% Insecticide Treated Net: 21.6% Malaria Test: 21.9% Iron/Folate: 11.8% Any ANC visit: 39% –Content unknown, unlikely effective

36
Baseline Survey Results Unmet need is high; substantial potential for family planning impact –25% do something to delay pregnancy –Overall 61% with unmet need for limiting/spacing Neonatal, infant, child mortality rates moderately high –Lower than more unstable direct conflict areas –Higher than Burma national estimates

37
For access to individual ANC interventions, trend toward decreased access for those experiencing human rights violations Forced relocation:Odds Ratio –anemia: 2.90 (1.90, 4.44) –unmet need: 1.68 (1.15, 2.46) –No ANC: 3.34 (0.97, 11.5) –<2 core ANC ints7.63 (1.85, 31.5) HRVs and Health Indicators Mullany LC, Lee CI, Yone L, Paw P, Shwe Oo EK, Maung C, Lee TJ, Beyrer C. Access to essential maternal health interventions and human rights violations among displaced communities in eastern Burma. FORTHCOMING, 2008

38
Preliminary PRF data ANC InterventionCoverage - Malaria screening during pregnancy68% - Insecticide treated net75% - Fe/FA supplement91% - Deworming83% - Nutrition / ENC89% Labor and Delivery - Attended by person with some BEOC69% - Misoprostol prophylactic dose given78% PNC Intervention - Family planning counseling provided90%

39
Cross-Border Medical Obstetric Medic in Eastern Burma, 2007

40
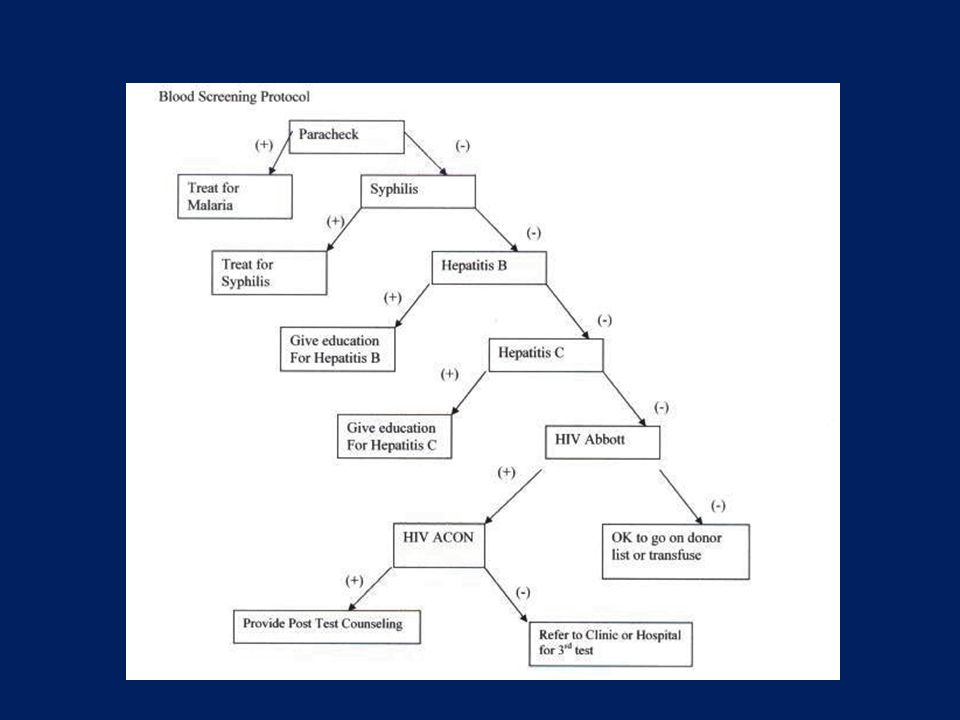
Adapt interventions to setting Developed a field protocol for blood screening for emergency transfusions Based on “living blood bank” concept- prescreening of family, community for typing Heat stable rapid test algorithm based on disease prevalence Improves safety of prior transfusion practices in this setting

42
How do human rights violations increase vulnerability to STI & HIV? Increased Exposure –Coercion, sexual violence, rape as tool of war, population mixing Increased Acquisition and Transmission –Treatment delays or gaps, barriers to access, lack of condoms/contraception Increased morbidity and mortality –Barriers to access and to information

43
Burmese Migrants and Barriers to Access in Thailand Knowledge about Condoms Condom Usage Thai Nationals Burmese Migrants Source: Mullany et al, AIDS Care, 2003; Lertpiriyasuwat et al, AIDS, 2003; Leiter et al, Health & Human Rights, 2006 Barriers to information, health care: Language, Legal, Physical, Economic, & Political PHR/JHU: Thailand’s failure to provide access to services violates Thai law AND undermines national HIV and STD programs P<0.05 Men Women Men Women

44
Conclusions Constraints inherent in IDP context demand creative thinking and adapted solutions Grass-roots community organizations can take the lead even in refugee and IDP settings Building capacity to monitor PH programs –Ensures success of programs –Potential to understand direct and indirect impacts of human rights violations on health

45
Ways Forward Recognize –Human rights contexts of our work Partner –With the grassroots, with human rights groups in country and internationally, with those we seek to serve facing rights violations Act –Research, Advocate, and Fund

Similar presentations


 By the Human Rights and Adolescent RH Working Groups of the POLICY Project 2002.>")










>")





