Download presentation
Presentation is loading. Please wait.

1
4th Annual Healthcare Informatics Symposium
Design and Implementation of a Diabetes Medication Computer Assisted Decision Support (CADS) System 4th Annual Healthcare Informatics Symposium April 29th, 2011 Richard ‘RJ’ Kedziora In partnership with several leading researchers and endocrinologists (Rodbard &Vigersky) at Walter Reed Army Medical Center with support and funding from the Army Telemedicine and Advanced Technology Research Center (TATRC), we have developed and published a CADS application for the management of patients with Type 2 Diabetes who are on oral agents. The CADS program simplifies the work of the primary care provider by automatically making medication recommendations based on an established consensus algorithm integrating the essential information necessary including the patient’s blood glucose data upload from home, current and previous medications, diagnoses, and current laboratory data. Medication regimen recommendations include modifying the existing regimen, increasing or decreasing the current medication(s) used and/or adding additional oral agents to better control the patient’s diabetes. A one-year multi-site IRB-approved, randomized controlled trial is scheduled to begin the summer of 2011 to test the clinical efficacy of the system. Additional work is scheduled to expand the rules to include Type 1 Diabetes and multiple daily insulin doses (MDI). This presentation will provide an overview of the system and discuss the process of designing and implementing the clinical algorithms within the Comprehensive Diabetes Management Program (CDMP), an open source disease management application. Particular attention will be focused on the decisions and challenges in implementing the complex clinical rules and the technology chosen to implement the solution.
 System. 4th Annual Healthcare Informatics Symposium. April 29th, Richard ‘RJ’ Kedziora. In partnership with several leading researchers and endocrinologists (Rodbard &Vigersky) at Walter Reed Army Medical Center with support and funding from the Army Telemedicine and Advanced Technology Research Center (TATRC), we have developed and published a CADS application for the management of patients with Type 2 Diabetes who are on oral agents. The CADS program simplifies the work of the primary care provider by automatically making medication recommendations based on an established consensus algorithm integrating the essential information necessary including the patient’s blood glucose data upload from home, current and previous medications, diagnoses, and current laboratory data. Medication regimen recommendations include modifying the existing regimen, increasing or decreasing the current medication(s) used and/or adding additional oral agents to better control the patient’s diabetes. A one-year multi-site IRB-approved, randomized controlled trial is scheduled to begin the summer of 2011 to test the clinical efficacy of the system. Additional work is scheduled to expand the rules to include Type 1 Diabetes and multiple daily insulin doses (MDI). This presentation will provide an overview of the system and discuss the process of designing and implementing the clinical algorithms within the Comprehensive Diabetes Management Program (CDMP), an open source disease management application. Particular attention will be focused on the decisions and challenges in implementing the complex clinical rules and the technology chosen to implement the solution.")
2
Funding / Disclosures Founding Partner/Owner - Estenda Solutions
Funding from U.S. Army Medical Research and Materiel Command (USARMC) AMEDD Advanced Medical Technology Initiative (AAMTI) program. Congressionally Directed Medical Research Programs administered by Air Force in partnership with University of Pittsburgh Medical Center - sponsored by the honorable U.S. Representative John P. Murtha PI on grant COL. Robert Vigersky M.D. at Walter Reed Army Medical Center
 AMEDD Advanced Medical Technology Initiative (AAMTI) program. Congressionally Directed Medical Research Programs administered by Air Force in partnership with University of Pittsburgh Medical Center - sponsored by the honorable U.S. Representative John P. Murtha. PI on grant COL. Robert Vigersky M.D. at Walter Reed Army Medical Center.")
3
The Problem Not enough endocrinologist to treat patients with diabetes – most care is managed by primary care doctors Most patient’s not goal (A1C 6.5 – 7%) SMBG Issues SMBG not used effectively by patients / providers SMBG perception is that it is not used to adjust medications Large number of drug and combinations Therapy is not adjusted frequently enough
 SMBG Issues. SMBG not used effectively by patients / providers. SMBG perception is that it is not used to adjust medications. Large number of drug and combinations. Therapy is not adjusted frequently enough.")
4
Potential Medication Combinations
Drug classes include: biguanide, DPP-4 inhibitor, GLP-1 agonist, secretagogue, TZD, AGI, and basal insulin Excluded: Colesevelam and Bromocriptine 68 potential treatment combinations 8 mono 26 dual 31 triple 3 quadruple Dual : (M + DPP-4, M + TZD, TZD + GLP-1) Triple : (M + DPP-4 +TZD, M + GLP-1 + AGI)
 Triple : (M + DPP-4 +TZD, M + GLP-1 + AGI)")
5
The Solution - CADS Designed for primary care doctors to assist in better decision-making in modifying patient’s drug regimen to bring their blood glucose into better control. Currently Type 2 (Type 1 planning) Idea, concept and rules developed by COL. Robert Vigersky, M.D. - Director, Diabetes Institute, Endocrinology Service, Department of Medicine, Walter Reed Army Health Care System, Washington DC David Rodbard, M.D. – Biomedical Informatics Consultants, LLC, Potomac, Maryland
 Idea, concept and rules developed by. COL. Robert Vigersky, M.D. - Director, Diabetes Institute, Endocrinology Service, Department of Medicine, Walter Reed Army Health Care System, Washington DC. David Rodbard, M.D. – Biomedical Informatics Consultants, LLC, Potomac, Maryland.")
6
Journey Multiple facilitated group clinical chart reviews to reach consensus Initial standalone prototype development using CLIPS and Microsoft ASP – early 2000s Experimented with DROOLS moved to table-driven algorithm coded in Java Production system coding and integration with CDMP Clinical Trial 2011 – 2012 and beyond FDA Validation

7
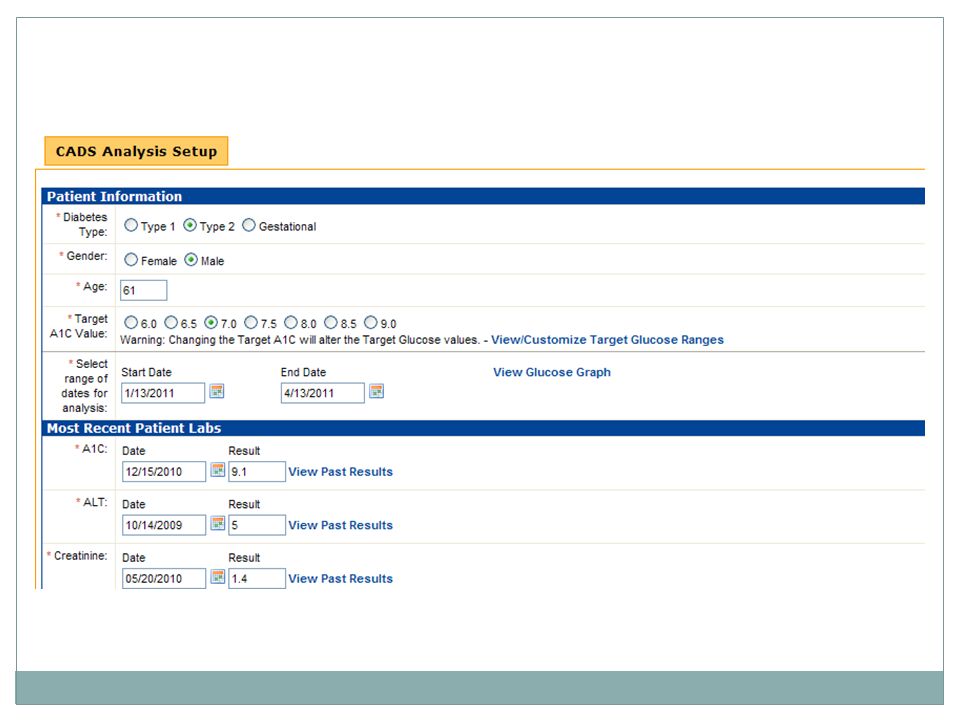
Input Age, Gender, Type of Diabetes
Self-managed blood glucose data (SMBG) Current and past medications Adverse Reactions Labs (A1C, ALT, Creatinine) Significant Diagnoses Renal, Hepatic, Gastrointestinal, Cardiac Target A1C
 Current and past medications. Adverse Reactions. Labs (A1C, ALT, Creatinine) Significant Diagnoses. Renal, Hepatic, Gastrointestinal, Cardiac. Target A1C.")
11
SMBG Testing Protocol For 3 months
Twice daily (or more depending on DR. discretion) Once a week Before meals (x3) and bedtime = 4 tests Once a month Before and 2 hours after meals (x3), bedtime and night at approximately 3AM = 8 tests
 Once a week. Before meals (x3) and bedtime = 4 tests. Once a month. Before and 2 hours after meals (x3), bedtime and night at approximately 3AM = 8 tests.")
12
Pre-Analysis Availability of SMBG
SMBG correlation with most recent A1c Identification of problem time-frames based on SMBG data Hypoglycemia Hyperglycemia Variability Time frames – before breakfast, after lunch

13
Analysis Overall quality of glycemic control
Effectiveness of SMBG testing Inappropriate medication combinations Existing Medication Contraindications Age, Gender, Labs, Diagnoses Based on SMBG profile analysis and medication effectiveness First, address Hypoglycemia Then address Hyperglycemia Still make recommendations if not enough data, but mark as suspect

14
Algorithm for Treatment of Type 2 Diabetes
Diet and Exercise If A1C > 6.5% Monotherapy or Combination Therapy Adequate Not adequate Follow-up q 3 mo Other Oral Combinations Adequate Not adequate Follow-up q 3 mo Oral Agent Plus Insulin at Bedtime (Glargine or NPH) Adequate Not adequate Follow-up q 3 mo Split-Mixed Insulin or Lispro or Aspart qac + Glargine or NPH qhs
 Adequate. Not adequate. Follow-up q 3 mo. Split-Mixed Insulin. or Lispro or Aspart qac. + Glargine or NPH qhs.")
15
Recommendations Modify the existing regimen because of contraindications Increase or decrease the dosage of current medication(s) Add additional oral agents/basal insulin 5+ medications or 4 with hyperglycemia - recommendation to consult endocrinologist Contraindications related to age, labs and diagnoses Increase only if patient is not already on ½ max of FDA recommended dosage.

16
Additional Output Where testing can be improved FDA Warnings
Rosiglitazone use has been severely restricted by the FDA because of concerns that it causes an increased number of cardiovascular events. Continued use requires your patient be enrolled in a risk evaluation and mitigation strategy program established by GlaxoSmithKline. You should consider switching this patient to pioglitazone at an equivalent dose… SMBG Profile by Time Period Min, Max, Average, Standard Deviation % high, % low based on thresholds

17
Sensitivity to being authoritarian
Suggestion vs. Command Multiple suggestions Education of clinicians

23
Algorithm Development
Started with Expert Rules System Initially used CLIPS Migrated to DROOLS Final solution - Table-driven logic with algorithm coded in Java Number of combinations Ability for versioning and customization by individual non-rule experts

25
Next Steps A one-year multi-site IRB-approved, cluster-randomized controlled trial Expand rule base to include Insulin dependant Type 2 Type 1 Expanded pattern recognition and treatment plans Post-prandial fluctuations Trends during day or night Hypoglycemia followed by rebound "Somogyi reaction“ Dawn Phenomenon cluster-randomized, controlled, clinical trial involving 30 PCPs who will each recruit approximately 19 patients from their respective geographic site. There will be up to 570 patients and 30 primary care providers in 3 geographic regions Trial – recently extended to a second year – controls become test subjects

26
Publication Rodbard and Vigersky, Design of a Decision Support System to Help Clinicians Manage Glycemia in Patients with Type 2 Diabetes Journal of Diabetes Science and Technology, Volume 5, Issue 2, March 2011

27
Thank you! Richard ‘RJ’ Kedziora Office: (610) Cell: (610)
 Cell: (610)")
28
CDMP Background Complete customizable web-based clinical application for management of patients with chronic disease. Based on the Chronic Care Model, it was originally designed for military healthcare to better manage patients with diabetes. Evolved into a generalized chronic disease and population health management system supporting the Patient Centered Medical Home model. For details visit:

Similar presentations