Download presentation
Presentation is loading. Please wait.

1
Management of Acute Severe Colitis
Dr Jayne Eaden Consultant Gastroenterologist, UHCW

2
Symptoms Bloody diarrhoea (urgency & tenesmus) Abdominal pain
Weight loss Obstructive symptoms Abdominal mass (esp RIF)
")
3
Warning Signs Fever > 37.8 oC Dehydration
Tachycardia (P>90), Hypotension Abdominal pain and tenderness (beware toxic dilatation and perforation) Patients can look well if been on steroids - beware
, Hypotension. Abdominal pain and tenderness (beware toxic dilatation and perforation) Patients can look well if been on steroids - beware.")
4
Other Signs Mouth ulcers Perianal disease Erythema nodosum
Pyoderma gangrenosum Eye disease Arthropathy (large joints, asymmetrical and non-deforming)
")
8
Truelove & Witts Criteria
Defines severe Ulcerative Colitis Bowels open > 6 times per 24 hours Plus any one or more of the systemic manifestations Haemoglobin < 10.5 ESR > 30 Pulse rate > 90 Temperature > 37.5

9
Differential Diagnoses
Bacterial infection C. diff, Campylobacter, Salmonella, Shigella, E. coli 0157 Viral infection if immuno-compromised (CMV) Amoeba especially if travel history Crohn’s colitis and ischaemia Diverticulitis can occasionally mimic
 Amoeba especially if travel history. Crohn’s colitis and ischaemia. Diverticulitis can occasionally mimic.")
10
Investigations on Admission
Bloods FBC ESR & CRP U&E, creat LFT (albumin) Blood cultures (if temp > 38°) Glucose (Mg+ and Cholesterol)
 Blood cultures (if temp > 38°) Glucose. (Mg+ and Cholesterol)")
11
Investigations on Admission
Stool Culture and Microscopy C. Diff (3 separate samples) AXR: look for stool-free colon (indicates extent involved); severe disease indicated by mucosal oedema (thickened wall), mucosal islands, dilated small bowel loops, colonic dilatation (diameter > 6cm) Inform the surgeons on call if the colon is dilated
 AXR: look for stool-free colon (indicates extent involved); severe disease indicated by mucosal oedema (thickened wall), mucosal islands, dilated small bowel loops, colonic dilatation (diameter > 6cm) Inform the surgeons on call if the colon is dilated.")
12
Colectomy more likely if:
-Mucosal islands present -Dilated small bowel loops

13
Investigations on Admission
Arrange a sigmoidoscopy and rectal biopsy. DO NOT prescribe bowel prep should be done within hours of admission Avoid colonoscopy and barium enema in patients with acute, severe colitis

14
Daily Investigations Bloods FBC
U&E, creat (particularly watch the potassium) LFT CRP (a vital prognostic guide) AXR for severe extensive colitis (any of fever, tachycardia, tenderness, dilatation on initial films) – in absence of these criteria less frequent AXR is OK Results must be reviewed the same day (esp potassium) particularly if abdominal X-ray is requested.
 LFT. CRP (a vital prognostic guide) AXR for severe extensive colitis (any of fever, tachycardia, tenderness, dilatation on initial films) – in absence of these criteria less frequent AXR is OK. Results must be reviewed the same day (esp potassium) particularly if abdominal X-ray is requested.")
15
Extra Investigations In appropriate patients, send Amoebic Fluorescent Antibody test Check CMV titre if patient is not responding after 3 days (EDTA sample)
")
16
Daily Monitoring Temperature and pulse Stool chart
Frequency Colour / blood content Estimate of volume (record even if only passed blood or mucus) Abdo examination findings tenderness, bowel sounds Note increasing pulse / temp / abdominal pain or tenderness may indicate deterioration or frank perforation and requires appropriate urgent investigation and d/w SpR / consultant.
 Abdo examination findings. tenderness, bowel sounds. Note increasing pulse / temp / abdominal pain or tenderness may indicate deterioration or frank perforation and requires appropriate urgent investigation and d/w SpR / consultant.")
17
Management Rehydrate with IV fluids
Correct electrolyte imbalance (in particular potassium) Nutrition : Low residue diet (IV fluids if vomiting) Inform colorectal surgeons & IBD nurse
 Nutrition : Low residue diet (IV fluids if vomiting) Inform colorectal surgeons & IBD nurse.")
18
Management Corticosteroids: Hydrocortisone 100mg QDS IV until remission achieved. May use Predsol/Predfoam PR once or twice per day (mainly for distal disease) Antibiotics (if febrile / toxic dilatation) Severely anaemic patients (Hb < 9g / dl) should be considered for transfusion DVT prophylaxis e.g enoxaparin 40mg od
 Antibiotics (if febrile / toxic dilatation) Severely anaemic patients (Hb < 9g / dl) should be considered for transfusion. DVT prophylaxis e.g enoxaparin 40mg od.")
19
Management Look for and treat proximal constipation
If stop 5-ASA, restart on discharge DO NOT Use opiates / codeine phosphate/ loperamide (may precipitate paralytic ileus, megacolon and proximal constipation) Use anti-cholinergics
 Use anti-cholinergics.")
20
Travis Criteria After three days of intravenous hydrocortisone, the presence of either Stool frequency > 8 times per 24 hours or Stool frequency > 3 times + CRP > 45 gives an 85% likelihood of requiring colectomy on the same admission

21
The Management of Acute Severe UC: options for rescue.......
If no improvement by day 3 make plans for day 5! Surgery or Cyclosporine Infliximab MUST be discussed with a Consultant Gastroenterologist

22
Indications for colectomy
Toxic dilatation with failure to improve clinically / radiologically within 24 hrs Perforation Uncontrolled lower GI haemorrhage Failure to respond after 3 days IV steroids Deterioration at any stage

23
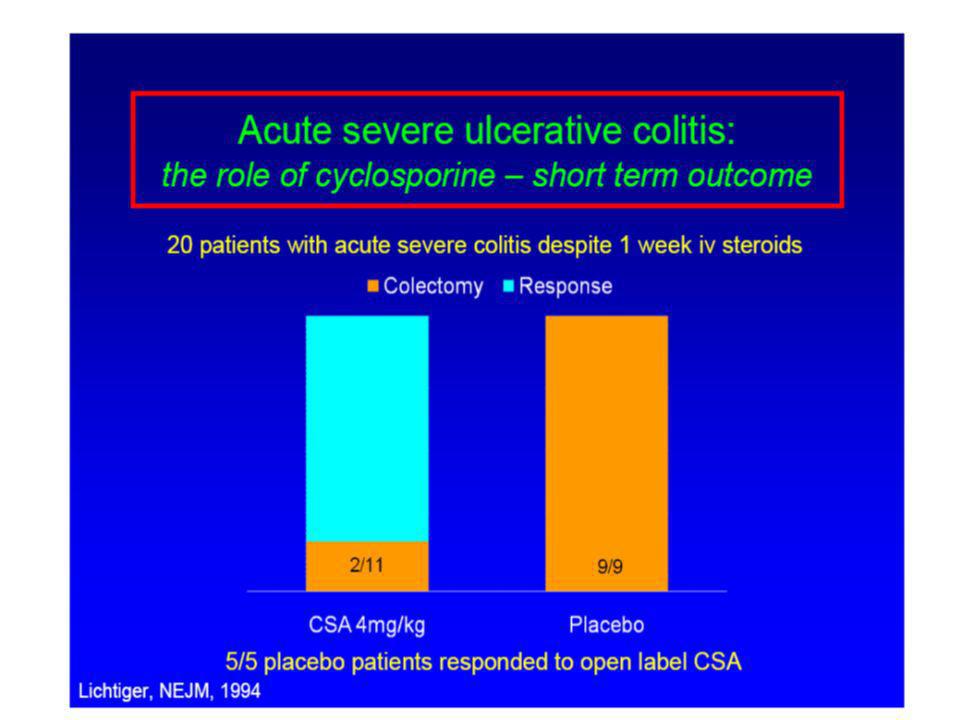
Acute severe UC: the role of cyclosporine
Only use if stool cultures negative Toxic drug – safety is paramount IV hydrocortisone is continued Check Mg+ and ensure cholesterol >3 Be aware of side effects (seizures) Care in elderly / hypertensive / impaired renal function
 Care in elderly / hypertensive / impaired renal function.")
24
Acute severe UC: the role of cyclosporine
What dose? 2mg/kg as IV infusion in 500mls glucose over 2-6 hrs Monitor levels ( mcg/l trough) Levels monitored at UHCW Mon-Fri Rapid steroid wean once clinical response If responded switch to oral after 3-5 days: 5mg/kg/day in 2 divided doses
 Levels monitored at UHCW Mon-Fri. Rapid steroid wean once clinical response. If responded switch to oral after 3-5 days: 5mg/kg/day in 2 divided doses.")
26
Acute severe UC: the role of cyclosporine – long term outcome
Clinical experience from Oxford 76 pts from followed 2.9 yrs 54 received 4mg/kg, 22 oral 5mg/kg 74% entered clinical remission and left hospital BUT 65% relapse at 1 yr, 90% at 3 yrs 58% of those came to colectomy at 7 yrs

28
Acute severe UC: the role of cyclosporine – exit strategy
Azathioprine naive vs refractory Ideally check TPMT levels on admission Commence Azathioprine at discharge Wean off Cyclosporine after 6-8 weeks Septrin 960mg alt days – prophylaxis against opportunistic infection Early follow up to check remission and bloods

34
Three intervention possibilities may prevent CRC: 1) surveillance by colonoscopy, 2) surgical removal of the ‘target’ and 3) cancer chemoprevention. However, despite the use of colonoscopic surveillance programmes for UC Dukes’ A, B, C and metastatic cancers still occur. Therefore, surveillance offers little help in early recognition of CRC. To increase the effectiveness of preventative measures for CRC, patients should be assessed with regard to: 1) family risk of CRC; 2) the genes underlying the inherited syndromes of CRC – which have been identified and 3) improved screening tests – which are now validated9. Whether these approaches offer any advantage in identifying patients at the pre-cancer/dysplastic stage in UC and CD has not been elucidated to date. Cancer prevalence rates of 3–22% have been reported in association with low-grade dysplasia10. In one study, 590 UC patients after proctocolectomy had the histological findings of their preoperative colonoscopy assessed. The odds ratio for synchronous cancer was 43 for low-grade dysplasia and 15 for high-grade dysplasia. 1Rosenstock et al. Gastroenterol 1985; 89: 2Connell et al. Gastroenterol 1994; 107: 3Jones et al. Gut 1988; 29: 4Lennard-Jones et al. The Lancet 1983; 2: 5Brostrom et al. Gut 1986; 27: 6Nugent et al. Gastroenterol 1993; 100: 7Lashner et al. Dig Dis Sci 1989; 34: 8Rozen et al. gastroenterol 1995; 108: 9Burt. Gastroenterology 2000; 119: 10Gorfine et al. Dis Col Rec 2000; 43:

37
Acute severe UC: the role of infliximab – safety issues
Possible risk of lymphoma & malignancy Increased if pt on other immunosuppressants Infectious complications (VZV, candida) Serious in 3% TB reactivation (PPD & CXR required prior to treatment) Interactions tacrolimus / live vaccines
 Serious in 3% TB reactivation (PPD & CXR required prior to treatment) Interactions tacrolimus / live vaccines.")
38
Acute severe UC: the role of infliximab – safety issues
Contraindications: Sepsis Significantly raised LFTs (x3), Hypersensitivity to infliximab Active TB Pregnancy } avoid for 6 months after Breast Feeding } stopping treatment Cautions: Previous TB Hepatic Impairment Renal Impairment Heart Failure Mouse allergies > 14 weeks since last infusion Several patients have died of sepsis following use, so it is contraindicated when uncontrolled bacterial infection is present.
, Hypersensitivity to infliximab. Active TB. Pregnancy } avoid for 6 months after. Breast Feeding } stopping treatment. Cautions: Previous TB. Hepatic Impairment. Renal Impairment. Heart Failure. Mouse allergies. > 14 weeks since last infusion. Several patients have died of sepsis following use, so it is contraindicated when uncontrolled bacterial infection is present.")
40
The 5-aminosalicylates have a lower risk of inducing GI tract bleeding than NSAIDs. Indeed, the risk of developing GI bleeding from 5-ASA is 1% compared with 18% for aspirin (ASA) and 2.6% for ibuprofen-based treatments1. Furthermore, NSAIDs are relatively contraindicated in IBD patients due to intestinal re-bleeding and reactivation of terminal ileitis2. 1Skeith KJ, Wright M et al. Differences in NSAID tolerability profiles. Fact or fiction? Drug Safety :183–195. 2Bjarnason I, Williams P et al. Intestinal permeability and inflammation in rheumatoid arthritis: effects of non-steroidal anti-inflammatory drugs. Lancet :1171–1174.

41
An epidemiological cohort study of 373 CD patients and 1161 UC patients, followed from 1962–1987, recommended maintenance treatment with sulphasalazine (and later 5-ASA, mesalazine)1,2 . In this study, approximately 42% of the patients, monitoring maintenance treatment with sulphasalazine or 5-ASA was continuous, and in 23% was intermittent. It was speculated that this high level of medical therapy with 5-ASA combined with early surgical treatment was responsible for the low occurrence of cancers in this cohort. 1Langholz E. Ulcerative colitis. An epidemiological study based on a regional inception cohort, with special reference to disease course and prognosis. Dan Med Bull :400–415. 2Munkholm P. Crohn's disease--occurrence, course and prognosis. An epidemiologic cohort-study. Dan Med Bull :287–302.

42
Infliximab for chronic active UC: can we predict who will respond?
Serum albumin <30g/l: 67% vs 23% colectomy OR 6.86 ( ) p=0.05 (Lees et al APT 2007) No effect of smoking status, age, stool frequency or disease extent
 p=0.05 (Lees et al APT 2007) No effect of smoking status, age, stool frequency or disease extent.")
43
Management of acute severe UC: summary of evidence
Acute severe UC requires specialist care within an experienced MDT Confirm diagnosis and exclude infection Non responders should be identified early and salvage therapy considered Controlled trials of cyclosporine vs infliximab are awaited

44
Management of acute severe UC: a multi disciplinary model
Physicians Surgeons The Patient Combined approach Nurses Dieticians Pharmacists Radiologists Pathologists

Similar presentations















>")














