Download presentation
Presentation is loading. Please wait.

1
UPDATE ON DIABETES AND INSULIN THERAPY BY Dr. M. SYED SULAIMAN. M
UPDATE ON DIABETES AND INSULIN THERAPY BY Dr.M.SYED SULAIMAN.M.D; PHYSICIAN & DIABETOLOGIST

2
DIABETES ENVIRONMENT IN INDIA
Diabetes is no more an epidemic, it is a PANDEMIC. Diabetes related complications pose greatest risk of morbidity and mortality.

3
No COUNTRY 2000 2030 1 INDIA 31.7 79.4 2 CHINA 20.8 42.3 3 U.S.A 17.7 30.3 4 INDONESIA 8.4 21.3 5 JAPAN 6.8 PAKISTAN 13.9 6 5.2 BRAZIL 11.3 7 U.S.S.R 4.6 BANGLADESH 11.1 8 8.9 9 ITALY 4.3 PHLIPPINES 7.8 10 BANGLADEH 3.2 EGYPT 6.7

4
BURDEN OF DIABETES : MORBIDITY
DIABETIC RETINOPATHY #1 Cause of blindness in working age adults DIABETIC NEPHROPATHY #1 Cause of ESRD DIABETIC NEUROPATHY AMPUTATIONS #1 Cause of non-traumatic amputations of lower Extremity. DIABETIC VASCULAR DISEASE 2 to 6 fold higher risk of CVD

5
DEFINITION Diabetes Mellitus is a group of metabolic diseases characterized by Hyperglycemia resulting from defects in Insulin secretion, Insulin action, or both.

6
ETIOLOGIC CLASSIFICATION OF
DIABETES MELLITUS 1.Type 1 Diabetes Immune mediated Idiopathic 2.Type 2 Diabetes

7
3.Other specific types: a. Genetic defects of b-cell function
b. Genetic defects in insulin action c. Disease of exocrine pancreas d. Endocrinopathies e. Drug/chemical induced f. Infection g. Uncommon immune mediated h. Other Genetic Syndromes 4. GESTATIONAL DIABETES MELLITUS(GDM)
")
8
IMPAIRED INSULIN SECRETION &
ETIOLOGY OF TYPE 2 DM IMPAIRED INSULIN SECRETION & INSULIN RESISTANCE GENES & ENVIRONMENT GENES AND ENVIRONMENT IMPAIRED INSULIN SECRETION IMPAIRED INSULIN SECRETION + INSULIN RESISTANCE INSULIN RESISTANCE IMPAIRED GLUCOSE TOLERANCE IMPAIRED GLUCOSE TOLERANCE TYPE 2 DM

9
IFG -Impaired Fasting Glucose IGT -Impaired Glucose Tolerance
DIAGNOSTIC CRITERIA OF DIABETES NORMAL IFG/IGT DIABETES FPG <100 ≥100<126 ≥126 2hrPost Glucose Load <140 ≥140<200 ≥ 200 IFG -Impaired Fasting Glucose IGT -Impaired Glucose Tolerance

10
What is pre diabetes? Abnormal blood glucose Values which is clearly Above the normal values but less than the Values diagnostic of Diabetes [IMPAIRED GLUCOSE METABOLISM]

11
MAJOR RISK FACTORS FOR TYPE 2 DM
1. Age>45 2. Race / Ethnicity (Asian / Asian American / Hispanics / etc) 3. Obesity (>30kg/m) 4. Family h/o Diabetes 5. Sedentary lifestyle 6. h/o GDM or delivered a baby weighing>4.5kg 7. PCOS
 3. Obesity (>30kg/m) 4. Family h/o Diabetes. 5. Sedentary lifestyle. 6. h/o GDM or delivered a baby. weighing>4.5kg. 7. PCOS.")
12
ACUTE METABOLIC COMPLICATIONS OF DIABETES MELLITUS
A.) DIABETIC KETOACIDOSIS B) HYPEROSMOLAR HYPERLYCEMIC STATE C) HYPOGLEMIA
 DIABETIC KETOACIDOSIS. B) HYPEROSMOLAR HYPERLYCEMIC STATE. C) HYPOGLEMIA.")
13
Diabetes Mellitus and chronic complications
Diabetes is a vascular disease Affects both small and medium sized arteries (micro vascular ¯o vascular)
")
14
Chronic complications
MICRO VASCULAR Retinopathy Nephropathy Neuropathy Macrovascular CVD CAD PVD

15
MANAGEMENT Diet Exercise Insulin Oral Antidiabetic Drugs
DPP 4 Inhibitors Amylin Analogues

16
ORAL ANTI DIABETIC DRUGS
Secretogauges a) Sulphonylurias b) Non sulphonylurias Biguanides Alpha Glucosidase Inhibitors( A G I ) Thiozolidinediones DPP 4 Inhibitors Amylin Analogues Exenatide
 Sulphonylurias. b) Non sulphonylurias. Biguanides. Alpha Glucosidase Inhibitors( A G I ) Thiozolidinediones. DPP 4 Inhibitors. Amylin Analogues. Exenatide.")
17
SECRETOGOUGES Sulphonyluria Groups First Generation SU 1.Tolbutamide
2.Chlorpropamide Second Generation SU 1.Glibenclamide(Daonil,Euglucon) 2.Glipizide(Glynase,Dibizide) 3.Gliclazide(Diamicron,Reclide) 4.Glimipride(Amaryl,Glipride,Glimer)
 2.Glipizide(Glynase,Dibizide) 3.Gliclazide(Diamicron,Reclide) 4.Glimipride(Amaryl,Glipride,Glimer)")
18
SECRETOGOGUES Currently available secretogogues stimulate Insulin secretion by causing closure of ATP dependent Potassium channel in Islet β cells.

19
NON SU SECRETOGOGUES Meglitinides Repaglinide(Novonorm)
")
20
INSULIN SENSITIZERS Agents from this group enhances the effect of endogenous Insulin. A reduction in Insulin resistance at each and every stage of diabetes will improve Glucose metabolism. Biguanide(Metformin),Thiozolidinediones(PIO,ROSI)
,Thiozolidinediones(PIO,ROSI)")
21
BIGUANIDES METFORMIN(Glyciphage,Glycomet).
Primary site of action:Liver. Reduces hepatic glucose output. Reduce fasting hyperglycemia.

22
THIOZOLIDINEDIONES Troglitazone Rosiglitazone(Rezult,Enselin)
Pioglitazone(Pioz,Pioglit) Primary site of action : Adipose Cells, Skeletal muscles.
 Primary site of action : Adipose. Cells, Skeletal muscles.")
23
AGI Acarbose(Glucobay,Acarb) Miglitol(Misobit,Mignor)
Voglibose(Volibo,Volix) Blocks alpha glucosidase enzyme Targets postprandial hyperglycemia
 Blocks alpha glucosidase enzyme. Targets postprandial hyperglycemia.")
24
DPP 4 Inhibitors (Dipeptidyl Pepsidase 4)
Nateglinide Citagliptin Vidagliptin DPP 4 Inhibits GLP 1.Thus extends Insulin action. Improves satiety,Increases β cell production,Inhibits β cell apoptosis delays gastric emptying,stimulate Insulin release

25
AMYLIN ANALOGUES Pramlintide

26
INSULIN First hormone to be Discovered Introduced in clinical practice
Structurally characterized Synthesized – chemically Biosynthesized – by rDNA technology

27
Insulin – Definitive Therapy for Diabetes
In diabetes there is impaired insulin secretion and impaired insulin action Exogenously administered Insulin can overcome both defects Thus insulin is the definitive therapy for all types of diabetes

28
INSULIN ABSOLUTE INDICATIONS
Regular Use Type 1 Diabetes Patients Type 2 Diabetes Patients with OHA failure - Primary - Secondary Intermittent Use Type 2 diabetes patients during - major surgery - pregnancy, labour and delivery - myocardial infarction - acute infections - acute metabolic crisis like hyperosmolar non ketotic coma and lactic acidosis Gestational diabetesmellitus

29
Type 1 DM Insulin Therapy
Initiating insulin therapy in uncomplicated ambulatory Type 1 patients Initiating insulin therapy in ill patients with altered sensorium

30
Type 1 DM Insulin Therapy : Initiation
In uncomplicated ambulatory Type 1 patients Patients should preferably be admitted to hospital Initiate with short-acting insulin [0.5 IU/Kg body weight per day] divided over 3 doses/day given pre-meal; subcutaneously

31
Type 1 DM Insulin Therapy : Initiation
If hospital admission is not possible, close continuous monitoring of the patient is necessary After adequate control is obtained with the above treatment a minimum of twice daily regimen with a short and intermediate-acting insulin may be given as per individual patient requirement

32
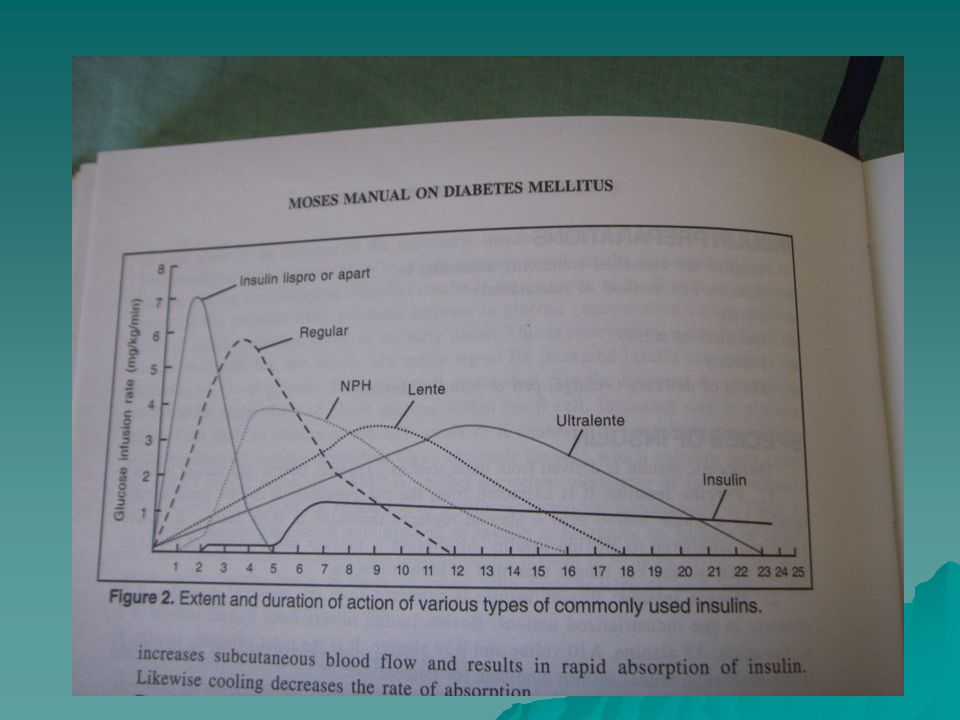
ACTION PROFILE OF INSULIN
Type Onset Peak Duration Rapid-Acting Analogues (Aspart, Lyspro) min 1-1.5 h 4-5 h
 min h. 4-5 h.")
34
ACTION PROFILE OF INSULIN
Type Onset Peak Duration Short-Acting (Regular) 30-60 min 2-4 h 6-8 h
 min. 2-4 h. 6-8 h.")
36
ACTION PROFILE OF INSULIN
Type Onset Peak Duration Intermediate-Acting(Basal) NPH 2-5 h 6-8 h 14-18 h
 NPH. 2-5 h. 6-8 h h.")
38
ACTION PROFILE OF INSULIN
Type Onset Peak Duration Pre-Mixed (30/70,50/50 Regular/NPH) 30 min 2-8 h 14-18 h
 30 min. 2-8 h h.")
40
ACTION PROFILE OF INSULIN
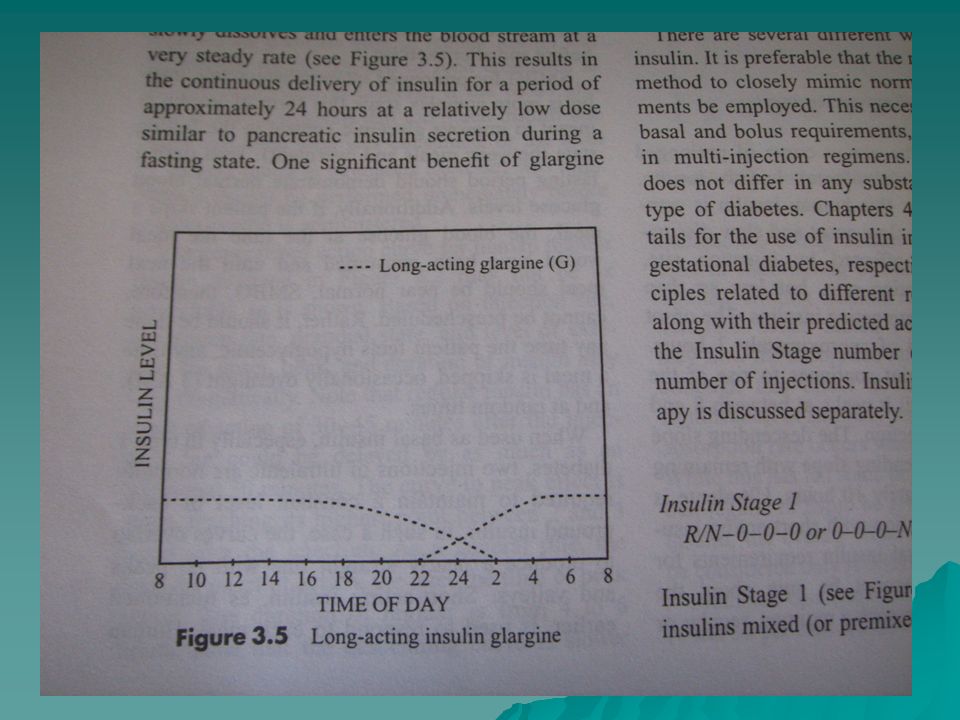
Type Onset Peak Duration Long-Acting Analogue (Detemir,Glargine) 2-3 h No peak 24-30 h
 2-3 h. No peak h.")
42
TYPES OF INSULINS Type Formulation preparation Onset (hr) Max.
effect (hr) Duration (hr) Short Regular H.Actrapid Actrapid 0.5 1-3 8 Intermediate - NPH (Neutral protamine Hagedom)/ Isophane H.Insulatard Insulatard 1.5 4-12 24 - Insulin Zinc Suspension/ Lente H.Monotard Lentard 2.5 7-15 Biphasic Regular (30%) + NPH (70%) H.Mixtard Mixtard 2-8
 Duration (hr) Short. Regular. H.Actrapid Actrapid Intermediate. - NPH (Neutral protamine Hagedom)/ Isophane. H.Insulatard Insulatard Insulin Zinc Suspension/ Lente. H.Monotard Lentard Biphasic. Regular (30%) + NPH (70%) H.Mixtard Mixtard")
43
REGIMENS Should maintain normal blood glucose levels (Normoglycemia)
Mimic normal physiological profile Regimens vary in Type 1 and type 2 diabetes because of different pathophysiology

45
INSULIN REGIMENS – Type 1 Diabetes
Insulin secretion totally absent Insulin administration tailored to match demand (food intake) Need for multiple injections Popular Regimens * Basal Bolus: Ideal but difficult to implement * Split mix therapy: Popular regimen; Patients find mixing insulins difficult Premixed Insulins: Most popular regimen world- wide and in India Right mix of compliance and control Insulin required i.u/kg body weight/day - Regimen depends on blood glucose profiles
 Need for multiple injections. Popular Regimens. * Basal Bolus: Ideal but difficult to implement. * Split mix therapy: Popular regimen; Patients find mixing insulins difficult. Premixed Insulins: Most popular regimen world- wide and in India. Right mix of compliance and control. Insulin required i.u/kg body weight/day. - Regimen depends on blood glucose profiles.")
46
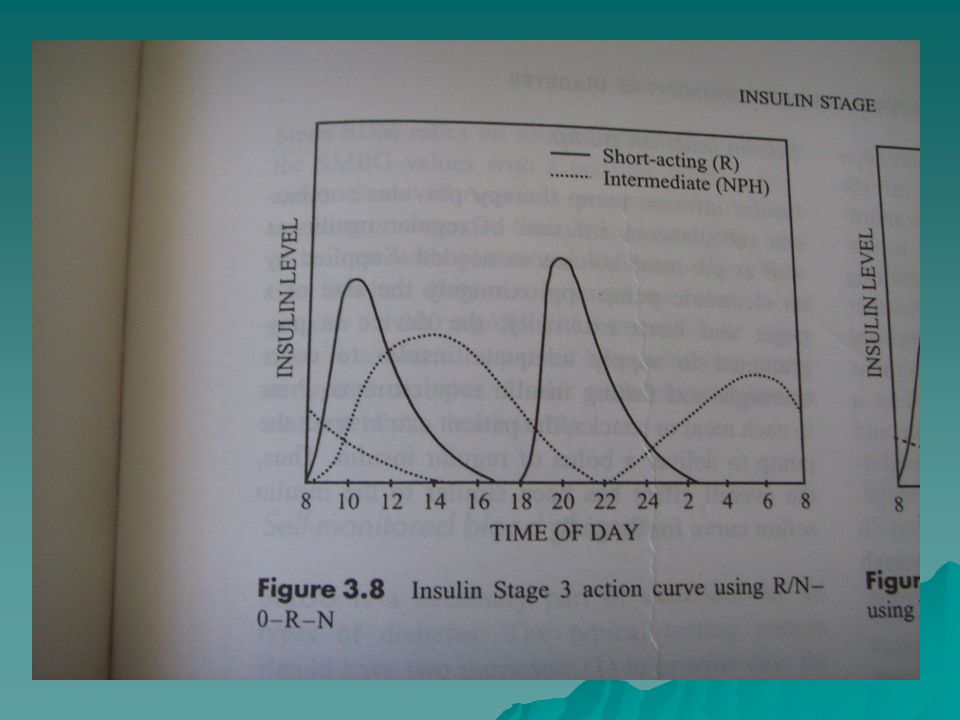
BASAL BOLUS THERAPY At least four injections/day
Intermediate injection at bedtime soluble insulin before breakfast, lunch and dinner Regular blood monitoring must Requires highly motivated patient

48
SPLIT MIX REGIMENS Two injections (intermediate + soluble) per day
before breakfast and before bedtime Proportion/dosage of insulin titrated based on blood glucose profile Mixing insulin is tedious and problematic

51
A. COMPLIANCE Defective insulin regimen
Incorrect technique of mixing and measuring Inconsistent eating and exercise habits Omission of insulin during inter current illness Lack of awareness about diabetes at the beginning and during the course of illness Emotional and psychological disturbance

52
B. CHANGE IN INSULIN REQUIREMENTS
Inactivity Weight gain / Loss Pregnancy and Post delivery phase Change in the exercise pattern Change in the food habits Stress period

53
PREMIXED REGIMENS – Human Mixtard
Very Popular regimen Most popular World-wide & in India Right balance of convenience and control Improves compliance Popular schedule is 2/3rd daily dose half an hour before breakfast 1/3rd daily dose half an hour before dinner

54
Insulin Therapy for Type 2 DM
Basal Insulin Supplementation: Bedtime NPH Suppresses basal hepatic production Reduces fasting plasma glucose Generally used in combination with OHA Helps initiate the patient on insulin therapy with Insulatard NovoLet

56
Guidelines for Initiating Insulin
Alone or in combination with an OHA 0.2 units/kg body wt./day of intermediate acting insulin e.g. Insulatard NovoLet Increase dose by 2-4 u every 3-4 days if necessary. If requirement exceeds u, split the dose into two daily : 2/3 before breakfast, 1/3 before dinner If postprandial glucose levels are high introduce short acting insulin in 30:70 or 50:50 ratio

57
Early Insulin Initiation
Is therefore beneficial in: Providing better control of hyperglycemia Reversing other metabolic defects Controlling inflammation which may initiate and aggravate development and progression of diabetes and diabetes-induced tissue damage Preserving beta cell function and thus helping maintain better glycemic control in the long-term Should be done when it can be useful to the patient

58
FACTORS AFFECTING INSULIN PHARMAKOKINETICS
Injection site Exercise Depth of injection Insulin source Potency Insulin antibodies

59
Injection Site The absorption varies with change of area
Rotation of site within the same area Short Acting - ABDOMEN - If rapid action desired Suspensions - THIGH - for longer action Random rotation of the site should be avoided

60
Rotation of Site in a given area
Blood flow Temperature Heavy massage in the injected area

61
Exercise Exercise following insulin injection increases the amount of insulin absorbed as well as the rate at which it is absorbed Exercise increases the peripheral glucose utilisation by increasing the insulin sensitivity

62
Depth of injection IM Vs SC inj
Absorbed faster with IM injections IM injections are not recommended for routine use Useful only in patients with subcutaneous insulin degradation or resistance IM injections are more painful SC is therefore ideal Soluble [ Human Actrapid ] can be given IV during surgery and diabetic emergencies

63
Source of insulin Human Insulin is absorbed quicker
Bovine Insulin is the slowest Porcine is absorbed little slower than Human Auxiliary Substances Preservative - phenol, metacresol Retarding Agent – protamine, zinc Water as solvent

64
Insulin Antibodies Circulating antibodies and exogenous insulin bind to form insulin antibody complex The antibody bound insulin may produce a delayed effect at an unexpected time Resulting from Reduced absorption , Delayed clearance

65
Thankyou

Similar presentations