Download presentation
Presentation is loading. Please wait.

1
Lisa Johnson, DPT, OCS, WCS, CSCS 2013
The Link Between Pelvic Floor Dysfunction and Pelvic Girdle Pain in the Female Athlete Lisa Johnson, DPT, OCS, WCS, CSCS 2013

2
Case: Pro Softball Player
Chief Complaints: Constant, aching suprapubic and low back pain. Intermittent left LE radicular pain to calf. Intermittent vaginal pressure, severe cramping, painful defecation and increased urinary urgency. Worse with running and jogging. Pain Scale: 6/10 (rest) / 10/10 (activity) 32 yr/old woman, phys ed teacher, basket ball coach
 / 10/10 (activity) 32 yr/old woman, phys ed teacher, basket ball coach.")
3
History: While catching a football pass four years prior, the pt. felt a sudden, sharp vaginal pain which persisted and progressed to the pubic and rectal regions. Symptoms have progressively worsened. PMH: Long history of low back pain. Treated by chiropractor (x 3yrs), PT, acupuncture and massage therapy with minimal benefit. MRI: (+) L 4-5 HNP Due to the forces of impact involved in sport, the female pelvis is susceptible to injury which can manifest itself in complex musculoskeletal dysfunction involving the spine and pelvis. Often times, we treat out the spine, Si joint and common muscle injuries of the LE, without considering the role of the pelvic floor in balancing and stabilizing the pelvic girdle.
, PT, acupuncture and massage therapy with minimal benefit. MRI: (+) L 4-5 HNP. Due to the forces of impact involved in sport, the female pelvis is susceptible to injury which can manifest itself in complex musculoskeletal dysfunction involving the spine and pelvis. Often times, we treat out the spine, Si joint and common muscle injuries of the LE, without considering the role of the pelvic floor in balancing and stabilizing the pelvic girdle.")
4
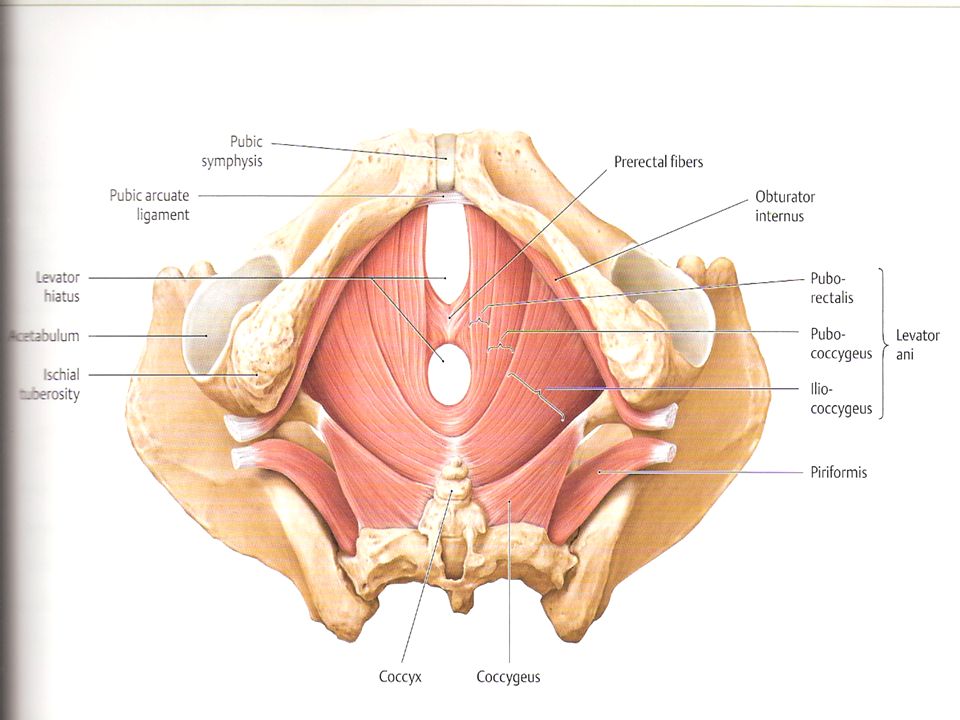
Pelvic Floor Anatomy The pelvic floor consists of five layers:
III – Pelvic Diaphragm / Levator Ani Muscles (Deep): 1. Pubococcygeus 2. Puborectalis 3. Iliococcygeus 4. Ischiococcygeus (Coccygeus) Levator Ani- First three muscles, responsible for elevating the pelvic floor, resisting increases in intra-abdominal pressure. Innervated by the perineal branch of the pudendal nerve (S2-S4) and ventral rami of (S3,4).
: 1. Pubococcygeus. 2. Puborectalis. 3. Iliococcygeus. 4. Ischiococcygeus (Coccygeus) Levator Ani- First three muscles, responsible for elevating the pelvic floor, resisting increases in intra-abdominal pressure. Innervated by the perineal branch of the pudendal nerve (S2-S4) and ventral rami of (S3,4).")
5
Pelvic Floor Anatomy III – Levator Ani Muscles (Deep): Pubococcygeus:
Arises from the dorsal surface of the pubic bone and obturator internus fascia, inserts on the anococcygeal and perineal bodies, anal wall. Forms a hammock to support the urethra, vagina and rectum. Pulls the rectum toward the pubic bone. Common complaint in runners –”pulling on my tailbone while I run”.

6
Pelvic Floor Anatomy III – Levator Ani Muscles (Deep):
2. Puborectalis: Arises from the medio-lateral, dorsal surface of the pubic bone, blends with the lateral walls of the anus and rectum, and inserts at the external anal sphincter and anococcygeal body. Controls descent of feces by elevating and constricting anal canal. Restriction will impede defecation and prevent fecal clearing.

7
Pelvic Floor Anatomy III – Levator Ani Muscles (Deep):
3. Iliococcygeus: Arises from the ischial spine and fascia of obturator internus, inserts to the anococcygeal body, anal wall and the coccyx. Pulls the vagina and rectum toward the pubic bone. Most widely recognized source of peri-anal referred pain to the sacrum, coccyx, rectum, vagina and lumbar spine.

8
Pelvic Floor Anatomy III – Levator Ani Muscles (Deep):
4. Ischiococcygeus (Coccygeus): Originates on the ischial spine and inserts on the caudal aspect of the sacrum and the coccyx. Provides tension to the pelvic floor, but not truly part of levator ani. Pulls the coccyx forward and stabilizes the sacroiliac joint. Innervated by ventral rami S4-S5
: Originates on the ischial spine and inserts on the caudal aspect of the sacrum and the coccyx. Provides tension to the pelvic floor, but not truly part of levator ani. Pulls the coccyx forward and stabilizes the sacroiliac joint. Innervated by ventral rami S4-S5.")
10
Pelvic Floor Function Supportive: to the pelvic/abdominal organs. Elevates the pelvic floor, resisting increases in intra-abdominal pressure. Sphincteric: Relaxes and contracts the urethral, vaginal and rectal openings. Sexual: Maintains clitoral erection, provides tone and proprioception to the vaginal wall.

11
PELVIC FLOOR DYSFUNCTIONS
Two types of pelvic floor dysfunctions: Hypertonus Dysfunctions (pain) - 15% of women have chronic pelvic pain. - Persistent or recurrent pelvic pain (> 3 mos) associated with symptoms of lower urinary tract, sexual, bowel or gynecological dysfunction. No proven infection or obvious pathology. - More common in women (Steege, 1996) - Hypertonicity of the PFM often arises in young, very fit women with a hypertonic abdominals, preventing PFM relaxation.(Sapsford et al 2001) Chronic pelvic pain - >3mos(National Inst. Of Child Health and Human Development, 1999); anywhere from umbilicus to genital region (Zondervan and Barlow, 2000)
 - 15% of women have chronic pelvic pain. - Persistent or recurrent pelvic pain (> 3 mos) associated with symptoms of lower urinary tract, sexual, bowel or gynecological dysfunction. No proven infection or obvious pathology. - More common in women (Steege, 1996) - Hypertonicity of the PFM often arises in young, very fit women with a hypertonic abdominals, preventing PFM relaxation.(Sapsford et al 2001) Chronic pelvic pain - >3mos(National Inst. Of Child Health and Human Development, 1999); anywhere from umbilicus to genital region (Zondervan and Barlow, 2000)")
12
PELVIC FLOOR DYSFUNCTIONS
Supportive Dysfunction (weakness) Incontinence (UI) and Prolapse - Prevalence rates: 10-55% general population 28-49% HS/college athletes % elite athletes. (Thyssen et al, 2002) Athletic activity can affect the development of (UI), depending on the extent of intra-abdom pressure and the strength of impact forces involved. (Bourcier et al. 1996) - Highest prevalence in sports involving high impact such as gymnastics, track and field and some ball games. (Bo, 2004) Gen pop, aged 15-64 While prevalence the same in elite athletes and age matched controls; rate of leakage during physical activity signif higher in elite athletes (Bo & Borgen, 2001) SUI has shown to lead to withdrawal from participation in sport and fitness activities. (Bo 1989, Nygaard, 1990); may be considered a barrier for lifelong participation in health & fitness activites in women (Brown & Miller, 2001) Question if UI due to wekness or tightness..if tightness, will this predispose them to pain later in life?? Is it weakness or other musculoskeltal issues inhibitting or “turning off the pelvic floor and causing UI; This is why assessment is keyresearch needed on PF function during physical activity and the effect of PF training on elite athletes
 Incontinence (UI) and Prolapse. - Prevalence rates: 10-55% general population % HS/college athletes 52% elite athletes. (Thyssen et al, 2002) Athletic activity can affect the development of (UI), depending on the extent of intra-abdom pressure and the strength of impact forces involved. (Bourcier et al. 1996) - Highest prevalence in sports involving high impact such as gymnastics, track and field and some ball games. (Bo, 2004) Gen pop, aged While prevalence the same in elite athletes and age matched controls; rate of leakage during physical activity signif higher in elite athletes (Bo & Borgen, 2001) SUI has shown to lead to withdrawal from participation in sport and fitness activities. (Bo 1989, Nygaard, 1990); may be considered a barrier for lifelong participation in health & fitness activites in women (Brown & Miller, 2001) Question if UI due to wekness or tightness..if tightness, will this predispose them to pain later in life Is it weakness or other musculoskeltal issues inhibitting or turning off the pelvic floor and causing UI; This is why assessment is keyresearch needed on PF function during physical activity and the effect of PF training on elite athletes.")
13
PELVIC FLOOR HYPERTONUS DYSFUNCTIONS
Symptoms: Primarily PAIN! Lumbar, perivaginal, perirectal, lower abdomen, coccygeal, posterior thigh. Vulvar/clitoral burning Dyspareunia (46% women-Steege, 1996) Constipation Common Diagnoses: Vulvodynia, interstitial cystitis, levator ani synd, coccydynia, pudendal neuralgia Dyspareunia_ recurrent or persistant genital pain before, during, after intercourse. (Amer. Psychiatric Assoc, 1994); 46% reproductive age)-Steege
 Constipation. Common Diagnoses: Vulvodynia, interstitial cystitis, levator ani synd, coccydynia, pudendal neuralgia. Dyspareunia_ recurrent or persistant genital pain before, during, after intercourse. (Amer. Psychiatric Assoc, 1994); 46% reproductive age)-Steege.")
15
PF Hypertonus Dysfunctions: Associated Myofascial Structures
Piriformis: Can compromise pudendal nerve. Refers pain into SI region, laterally to buttocks/posterior hip, 2/3 posterior thigh. Obturator Internus: Tendinous attachment with levator ani. Refers pain into vagina, occasionally to posterior thigh, feeling of “fullness” of rectum. It originates from the anterior (front) part of the sacrum, the part of the spine in the gluteal region, and from the superior margin of the greater sciatic notch (as well as the sacroiliac joint capsule and the sacrotuberous ligament). It exits the pelvis through the greater sciatic foramen to insert on the greater trochanter of the femur. Its tendon often joins with the tendons of the superior gemellus, inferior gemellus, and obturator internus muscles prior to insertion. It arises from the inner surface of the antero-lateral wall of the pelvis, where it surrounds the greater part of the obturator foramen, being attached to the inferior rami of the pubis and ischium, and at the side to the inner surface of the hip bone below and behind the pelvic brim, reaching from the upper part of the greater sciatic foramen above and behind to the obturator foramen below and in front. It also arises from the pelvic surface of the obturator membrane except in the posterior part, from the tendinous arch which completes the canal for the passage of the obturator vessels and nerve, and to a slight extent from the obturator fascia, which covers the muscle.
 part of the sacrum, the part of the spine in the gluteal region, and from the superior margin of the greater sciatic notch (as well as the sacroiliac joint capsule and the sacrotuberous ligament). It exits the pelvis through the greater sciatic foramen to insert on the greater trochanter of the femur. Its tendon often joins with the tendons of the superior gemellus, inferior gemellus, and obturator internus muscles prior to insertion. It arises from the inner surface of the antero-lateral wall of the pelvis, where it surrounds the greater part of the obturator foramen, being attached to the inferior rami of the pubis and ischium, and at the side to the inner surface of the hip bone below and behind the pelvic brim, reaching from the upper part of the greater sciatic foramen above and behind to the obturator foramen below and in front. It also arises from the pelvic surface of the obturator membrane except in the posterior part, from the tendinous arch which completes the canal for the passage of the obturator vessels and nerve, and to a slight extent from the obturator fascia, which covers the muscle.")
16
PF Hypertonus Dysfunctions: Associated Myofascial Structures
Hip Adductors: Adductor Magnus : Refers pain deep into groin, pubis, vagina, rectum. Usually “sharp, shooting” pain. Pectineus: Refers pain deep into groin, anterior hip joint, below inguinal ligament. The adductor magnus is a large triangular muscle, situated on the medial side of the thigh. It consists of two parts. The portion which arises from theischiopubic ramus (a small part of the inferior ramus of the pubis, and the inferior ramus of the ischium) is called the adductor portion or adductor minimus, and the portion arising from the tuberosity of the ischium is called the "hamstring portion” Those fibers which arise from the ramus of the pubis are short, horizontal in direction, and are inserted into the rough line of the femur leading from the greater trochanter to the linea aspera, medial to the gluteus maximus. The medial portion of the muscle, composed principally of the fibers arising from the tuberosity of the ischium, forms a thick fleshy mass consisting of coarse bundles which descend almost vertically, and end about the lower third of the thigh in a rounded tendon which is inserted into the adductor tubercle on the medial condyle of the femur, and is connected by a fibrous expansion to the line leading upward from the tubercle to the linea aspera. It arises from the pectineal line of the pubis and to a slight extent from the surface of bone in front of it, between the iliopectineal eminence and pubic tubercle, and from the fascia covering the anterior surface of the muscle; the fibers pass downward, backward, and lateral, to be inserted into the pectineal line of the femur which leads from the lesser trochanter to the linea aspera.
 is called the adductor portion or adductor minimus, and the portion arising from the tuberosity of the ischium is called the hamstring portion Those fibers which arise from the ramus of the pubis are short, horizontal in direction, and are inserted into the rough line of the femur leading from the greater trochanter to the linea aspera, medial to the gluteus maximus. The medial portion of the muscle, composed principally of the fibers arising from the tuberosity of the ischium, forms a thick fleshy mass consisting of coarse bundles which descend almost vertically, and end about the lower third of the thigh in a rounded tendon which is inserted into the adductor tubercle on the medial condyle of the femur, and is connected by a fibrous expansion to the line leading upward from the tubercle to the linea aspera. It arises from the pectineal line of the pubis and to a slight extent from the surface of bone in front of it, between the iliopectineal eminence and pubic tubercle, and from the fascia covering the anterior surface of the muscle; the fibers pass downward, backward, and lateral, to be inserted into the pectineal line of the femur which leads from the lesser trochanter to the linea aspera.")
17
Case: Evaluation Assess lumbar spine, SI joint, hips
Lower quarter muscle strength, tone and length Lower quarter neuro screen Assess pelvic floor muscles External and internal digital exam Sensation Symmetry Tone Strength How to assess for hypertonicity in the absence of internal assessment? History and ask the right questions: pain with penetration? (sex, tampons); difficulty completely emptying with voiding; constipation Hip ; Coady: 95% improvement in hip; 65% “” “” hip and pelvic floor; 30% - hip, not pelvic pain; 5% no hip or pelvic pain
; difficulty completely emptying with voiding; constipation. Hip. ; Coady: 95% improvement in hip; 65% hip and pelvic floor; 30% - hip, not pelvic pain; 5% no hip or pelvic pain.")
19
Case: Objective Findings
Tenderness to palpation: (Severe) pubic symphysis, lower abdom, pirif, levator ani mus; (Mod) lumbar L3-5, sacrotuberous lig, obturator int, sacrococcygeal region. ROM: Minimal limitation in trunk ext. MMT: R LE – 5/5; L LE – 4/5 Neural: ANTT L sciatic nerve, myotomal weakness L4-S1, Diminished L DTR Structural: R/L Backward sacral torsion Left posterior innominate, lumbar rot. right
 pubic symphysis, lower abdom, pirif, levator ani mus; (Mod) lumbar L3-5, sacrotuberous lig, obturator int, sacrococcygeal region. ROM: Minimal limitation in trunk ext. MMT: R LE – 5/5; L LE – 4/5. Neural: ANTT L sciatic nerve, myotomal weakness L4-S1, Diminished L DTR. Structural: R/L Backward sacral torsion. Left posterior innominate, lumbar rot. right.")
20
Physical Therapy Intervention
Manual Therapy & Therapeutic Ex Joint mobilization – lumbar, SI jt, hip Soft tissue mobilization External – lumbar, pirif, OI, IP, abdom.CTM Internal – pelvic floor muscles, OI Exercise Program Lumbar stabilization Aerobic conditioning LE muscle strengthening and flexibility Modalities – ES, biofeedback to relax PF Postural ed / body mechanics Pelvic floor one of the three primary stabilizers of the spine (Richardson et al. ther ex for spinal stab in low back pain text) Case: treated for 18 visits over 10 wks; returned for
 Case: treated for 18 visits over 10 wks; returned for.")
Similar presentations