Download presentation
Presentation is loading. Please wait.

1
THE LEEDS CENTRE FOR REPRODUCTIVE MEDICINE SEACROFT HOSPITAL Version 1.1: January 2010

2
Explain the treatment process Clinical Laboratory Nursing Highlight risks in treatment OHSS Multiple pregnancy Factors affecting outcome Increase awareness of protocols Information regarding research projects

6
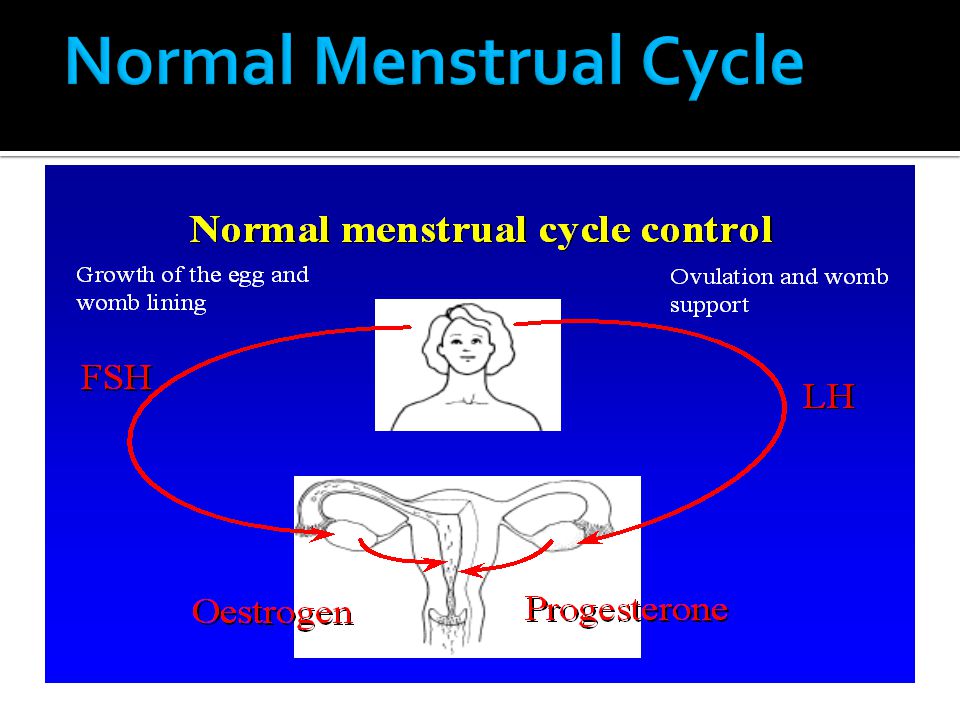
Why do we need to make changes? We need more than one egg in the cycle Not all eggs fertilise or grow Not all embryos have a good potential for development We want to transfer 1-3 embryos for a good success rate We do not want the gland in the brain to become confused in treatment

7
Long Protocol Flare Protocol Short Protocol

8
1. Suppression of the natural cycle To switch off the gland in the brain so that it does not interfere in treatment 2. Stimulation Hormone injections to produce multiple eggs 3.Ovulation trigger or HCG injection 4.Egg collection 5.Embryo transfer 6.Hormonal support after the embryo transfer

9
Oral Contraceptive Pill Prostap once a month injection OR Buserelin daily injection OR Nafarelin three times a day nasal spray Side effects headaches, hot flushes, night sweats, mood-swings, prolonged period or second bleeding

10
Ovary Uterus

11
Dose of stimulation is adjusted for: Reserve of eggs in the Ovary (hormone levels and scan findings) Age Weight or Body Mass Index Past history (infections, cyst removal) Presence or absence of PCOS Types:Menopur, Merional, Puregon, Gonal-F, Fostimon All are subcutaneous injections
 Age Weight or Body Mass Index Past history (infections, cyst removal) Presence or absence of PCOS Types:Menopur, Merional, Puregon, Gonal-F, Fostimon All are subcutaneous injections")
12
x x x x

13
HCG injection Pregnyl (commonest) Ovitrelle Recombinant LH Timed 36 hours prior to egg collection
 Ovitrelle Recombinant LH Timed 36 hours prior to egg collection")
14
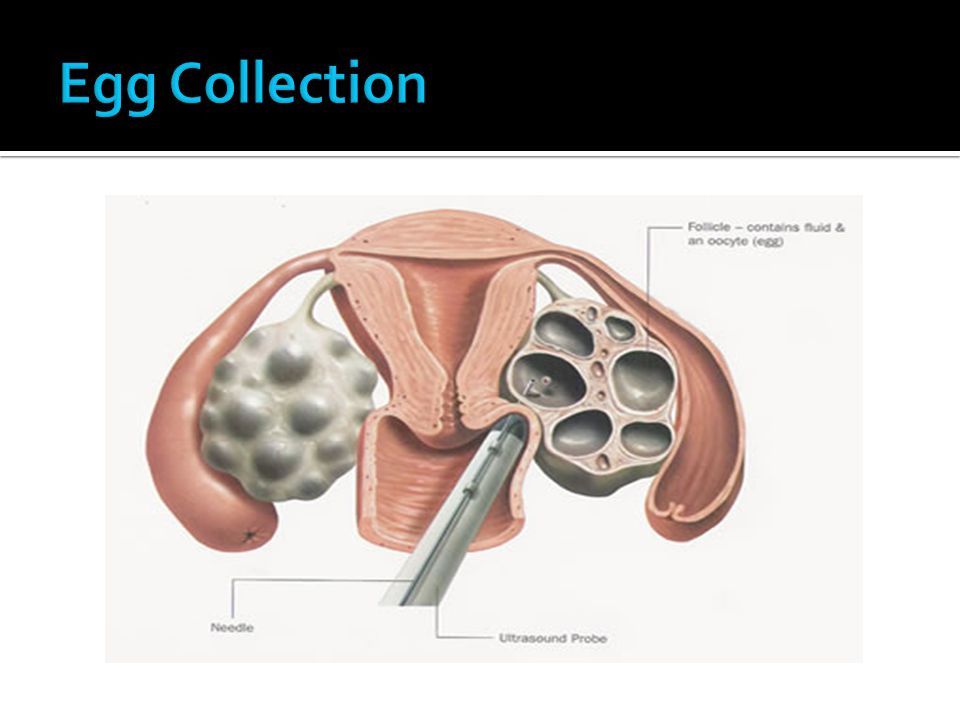
Performed under ultrasound guidance Fast acting sedation & analgesia Duration 20 - 45 minutes Out-patient based Return home after 2-3 hours Need care after returning home DO NOT DRIVE OR OPERATE MACHINERY

16
Common Symptoms mild discomfort for 1 - 3 days (Paracetamol suppository) slight discharge hang-over effect
 slight discharge hang-over effect")
17
Sperm production Insemination of Eggs or Sperm injection into the eggs Fertilisation check Observation of growth Selection of embryos for transfer

18
Embryo Transfer Procedure Requires a full bladder Performed under ultrasound guidance After Embryo Transfer: Hormone support: Mainly Progesterone Some HCG (with low risk) Pregnancy test 14-16 days later Worried Please contact US
 Pregnancy test days later Worried Please contact US")
20
Risk: Multiple embryos = in multiple pregnancy rate Our Objectives: 1.To maximise the pregnancy rate 2.To reduce the risk of a multiple pregnancy Before you think great, a twin pregnancy! We have our family completed in one go! Let us look at the facts of the next slide...

21
RiskTwinsTriplets Average Duration of Pregnancy (Term = 40 weeks) 37 weeks 34 weeks Proportion of premature low birth weight infants 50% 90% Neonatal death (1 st week of life) 5 x higher 9 x higher Postnatal cerebral palsy 4 x higher 18 x higher Maternal pre-eclampsia 3 x higher 9 x higher Maternal diabetes 2-3 x higher Maternal coronary heart disease 2 x higher Maternal death from cardiovascular causes 7-11 x higher Maternal death (overall) 2 x higher
 37 weeks 34 weeks Proportion of premature low birth weight infants 50% 90% Neonatal death (1 st week of life) 5 x higher 9 x higher Postnatal cerebral palsy 4 x higher 18 x higher Maternal pre-eclampsia 3 x higher 9 x higher Maternal diabetes 2-3 x higher Maternal coronary heart disease 2 x higher Maternal death from cardiovascular causes 7-11 x higher Maternal death (overall) 2 x higher")
22
We consider SET in: Women < 35 years First treatment cycle When fertilisation and growth of embryos is satisfactory When there are spare embryos for freezing

23
Day 2, 3 or 5 Objective: Select the best embryo at the earliest opportunity Choice is dependent upon: Total number of embryos available Quality of embryos Please trust us to do the BEST in your cycle

24
Cyst formation during the suppression phase Risk of cycle being abandoned ( Poor or Excessive response) (5-10%) On the day of egg collection No eggs (<1%) Not being able to give a sperm sample (anxiety, stress, very low counts, poor testicular function) Back up freezing or Emergency PESA After egg collection Complete fertilisation failure (3-5%) Failure of growth of embryos (<5%) Failed embryo transfer (very rare ; one a year)
 (5-10%) On the day of egg collection No eggs (<1%) Not being able to give a sperm sample (anxiety, stress, very low counts, poor testicular function) Back up freezing or Emergency PESA After egg collection Complete fertilisation failure (3-5%) Failure of growth of embryos (<5%) Failed embryo transfer (very rare ; one a year)")
26
Infection Pre-treatment swabs Dalacin cream Cleaning the vagina Sterile environment No touch technique Antibiotic in flush Prophylactic antibiotic in at risk cases RARE Injury to bowel leading to internal infection RARE Injury to blood vessel leading to internal bleeding RARE Version 2: March 2008: VS / EB

28
The risk is highest after the ovulation trigger and if you become pregnant Who is at a higher risk? Women with polycystic ovaries Young women < 30 years Severe OHSS is RARE (1-2%). However this is because we monitor everybody at risk ANY CONCERNS: Contact the Emergency On-Call phone
. However this is because we monitor everybody at risk ANY CONCERNS: Contact the Emergency On-Call phone.")
29
Miscarriage (15-20%) Ectopic pregnancy (3-4%) Multiple pregnancy (25%) Version 2: March 2008: VS / EB
 Ectopic pregnancy (3-4%) Multiple pregnancy (25%) Version 2: March 2008: VS / EB")
31
Age (years)
")
33
PESAMESA

34
Anonymity Laws Scarcity Recruiting known donor

35
Version 2: March 2008: VS / EB

36
Egg Collection Preparation of sperm sample Insemination (IVF) or sperm injection (ICSI) Fertilization check Embryo Transfer Freezing
 or sperm injection (ICSI) Fertilization check Embryo Transfer Freezing")
37
Looking for the eggs

38
A human egg in its surrounding cells A tenth of a millimeter

40
Produced in unit by masturbation Sterile specimen pot Witnessing procedures

42
In vitro fertilisation: IVF

43
Intra cytoplasmic sperm injection: ICSI

44
Only mature eggs can be injected (usually ~70%) Around 10% will be damaged by the injection Pregnancy rates are the same as for IVF
 Around 10% will be damaged by the injection Pregnancy rates are the same as for IVF")
45
Fertilisation overnight next day Version 2: March 2008: VS / EB

46
Normally fertilised egg

47
Usually around 60% of eggs will fertilise normally A proportion may be unfertilised, abnormally fertilised or non-viable, these eggs cannot be selected for treatment Patients will be telephoned the day after egg collection

48
Embryonic Development 2 cells4 cells 8 cells Morula Blastocyst Early day 2 Late day 2Day 3 Day 4 Day 5

49
fragmentation unevenness of cells cell numbers GoodPoor

50
Embryos for transfer selected (consents checked) Spare embryos may be - frozen - or placed into extended culture with a view to freezing (depending on quality)
 Spare embryos may be - frozen - or placed into extended culture with a view to freezing (depending on quality)")
52
Stresses of infertility and infertility treatment HFEA Code of Practice requires all units to offer counselling as a normal part of treatment Types of counselling Arranging an appointment Confidentiality

54
Both Partners: Healthy life style No Smoking Female: Avoid alcohol altogether Male: maximum of 12 units per week Female Partner: Good diet and normal body weight Up to date cervical smear Folic acid 400 mcgs daily Rubella

55
Tight schedule Please arrive promptly for appointments Allow plenty of time for parking Please ring unit if late or unable to attend to give us time to reschedule appointments Be sure you know what to do next before leaving the Unit

56
Both partners must attend the nurse consultation session Bring a passport sized photo of both partners and think of a password Photo ID (passport or driving licence) HFEA Registration
 HFEA Registration")
57
Welfare of the child Communication consent GP letters Information check list Trust consents to treatment number of embryos to be transferred observation and freezing of spare embryos

58
IVF /and ICSI consent Use of donor sperm / eggs Embryo research HFEA forms – use of eggs, sperm and embryos embryo freezing fate of sperm and embryos in the event of death or mental incapacity – disposal, research or posthumous use

59
1. NHS 2. Self-Funding or Private Payment If you are paying for your own treatment, payment must be made at the consultation appointment cash cheque credit card

60
Homecare dispensary service for all patients Pharmacy (prescription charge is payable) Injections Need to consider self/partner injection GP/Practice nurse Daily attendance to ACU/Gynae ward
 Injections Need to consider self/partner injection GP/Practice nurse Daily attendance to ACU/Gynae ward")
61
9-10 visits over 6 weeks 2-3 months

62
LCRM working hours - 8.30am - 5.00pm (0113 2063100) In an emergency... Out of hours weekdays (5pm until 8am) and weekends - A team member can be reached on a mobile phone via St Jamess switchboard (0113 2433144) Please try to contact staff during working hours as at other times they are not in the hospital and do not have access to your notes or the appointment diaries. Support Line – www.lacu-patient2patient.org.uk
 and weekends - A team member can be reached on a mobile phone via St Jamess switchboard ( ) Please try to contact staff during working hours as at other times they are not in the hospital and do not have access to your notes or the appointment diaries. Support Line –")
Similar presentations























 IVF enables fertilisation, outside the body, in a culture dish.>")

 is a process by which egg cells are manually fertilized by sperm outside of the womb. IVF is a major treatment.>")
.>")
