Download presentation
Presentation is loading. Please wait.

1
Office-Based Opioid Therapy: Methadone/Buprenorphine Nexus
Edwin A. Salsitz, M.D., FASAM Medical Director Office-Based Opioid Therapy Beth Israel Medical Center, NYC

2
Financial Disclosure Reckitt Benckiser Speaker Honoraria
Pfizer Speaker Honoraria PriCara Speaker Honoraria Purdue Pharma Adv.Board Honoraria

3
MEDICATION ASSISTED ADDICTION TREATMENT
“All Treatments Work For Some People/Patients” “No One Treatment Works for All People/Patients” Alan I. Leshner, Ph.D Former Director NIDA

4
OPIATE AGONIST THERAPY
Pharmacology Addiction Regulatory Stigma Destitution Political

7
The Lexington Narcotic Farm
The first facility opened on May 25, 1935, outside Lexington, Ky. The 1,050-acre site included a farm and dairy, working on which was considered therapeutic for patients. With the increased availability of state and local drug abuse treatment programs, the hospital was closed in February 1974. Drs. Kolb, Himmelsbach, Wikler, Jaffe, Kleber, Vaillant

9
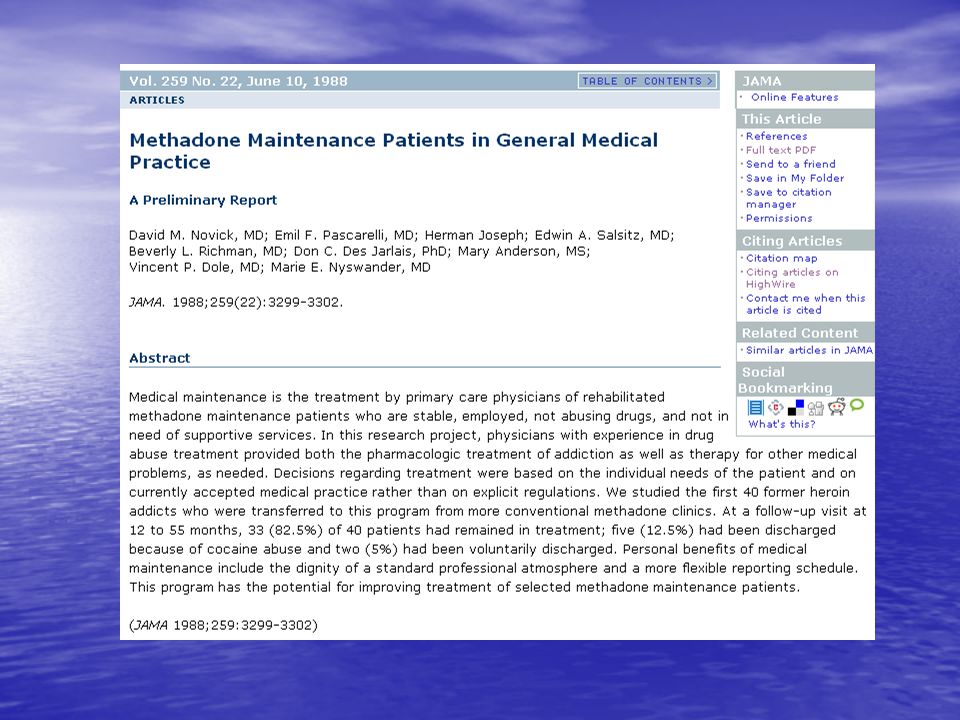
JAMA Classics: Celebrating 125 Years Methadone Maintenance 4 Decades Later
Thousands of Lives Saved But Still Controversial Commentary by Herbert D. Kleber, MD JAMA. 2008;300(19): JAMA. 1965;193(8):
: JAMA. 1965;193(8):")
10
Exclusion: non-opioid addiction/misuse, severe psychiatric problems

11
Opiate Addiction Treatment Outcome*
Methadone Maintenance – 80% Naltrexone Maintenance – 20% “Drug Free” (non-pharmacotherapeutic) 5 – 30% LAAM Maintenance – 80% Buprenorphine-Naloxone Maintenance %** Short-term Detoxification (any mode) – 20% (limited data) * One year retention in treatment and/or follow-up with significant reduction or elimination of illicit use of opiates ** Maximum effective dose (24mgsl) equal to 60 to 70 mg/d methadone. Data base on 6 month follow-up only. Kreek, 1996; 2001
 5 – 30% LAAM Maintenance 50 – 80% Buprenorphine-Naloxone Maintenance 40-50%** Short-term Detoxification (any mode) 5 – 20% (limited data) * One year retention in treatment and/or follow-up with significant reduction or elimination of illicit use of opiates. ** Maximum effective dose (24mgsl) equal to 60 to 70 mg/d methadone. Data base on 6 month follow-up only. Kreek, 1996;")
12
Methadone Synthetic Opioid 1937 Germany T ½ 24—36 hrs. Inherent
Onset of Action 30 min. Peak 3-4 hrs. R/S(l/d) racemic mixture mu/NMDA antag CYP3A4, 2D6 Drug/Drug No Active Metab Renal and biliary excretion Dosing QD for addiction, Q6H for Pain
 racemic mixture mu/NMDA antag. CYP3A4, 2D6 Drug/Drug No Active Metab. Renal and biliary excretion. Dosing QD for addiction, Q6H for Pain.")
13
Functional State (Heroin) Functional State (Methadone)
Impact of Short-Acting Heroin versus Long-Acting Methadone Administered on a Chronic Basis in Humans Study "High" Functional State (Heroin) (overdose) "Straight" "Sick" AM PM AM PM AM Days "High" Functional State (Methadone) "Straight" "Sick" AM PM AM H PM AM Days Dole, Nyswander and Kreek, 1966
 (overdose) Straight Sick AM. PM. AM. PM. AM. Days. High Functional State (Methadone) Straight Sick AM. PM. AM. H. PM. AM. Days. Dole, Nyswander and Kreek,")
15
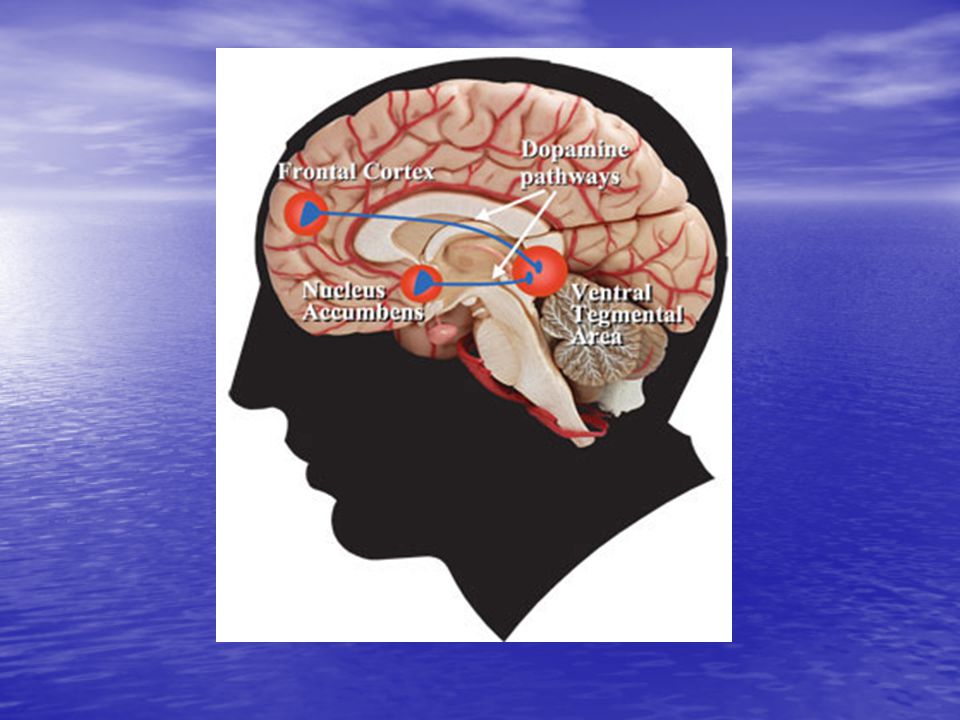
MesoLimbic Dopaminergic Circuit Pleasure/Reward Center
Acc VTA Amphetamine Cocaine Opiates Cannabinoids Phencyclidine Ketamine HIPP GLU FCX AMYG CRF GLU 5HT GABA OPIOID OPIOID ENK GABA GABA VP DYN 5HT OFT DA BNST GABA NE ABN LC Opiates PAG NE HYPOTHAL END LAT-TEG To dorsal horn Opiates Ethanol Barbiturates Benzodiazepines Nicotine Cannabinoids 5HT ICSS Raphé MesoLimbic Dopaminergic Circuit Pleasure/Reward Center H2O, Food, Sex, Parenting, Social RETIC

16
Molecular and Cellular Basis of Addiction
Science 3 October 1997: Eric J. Nestler, George K. Aghajanian Figure 2. Scheme illustrating opiate actions in the locus coeruleus. Opiates acutely inhibit locus coeruleus neurons by increasing the conductance of an inwardly rectifying K+ channel through coupling with subtypes of Gi/o, as well as by decreasing a Na+-dependent inward current through coupling with Gi/o and the consequent inhibition of adenylyl cyclase. Reduced concentrations of cAMP decrease PKA activity and the phosphorylation of the responsible channel or pump. Inhibition of the cAMP pathway also decreases phosphorylation of numerous other proteins and thereby affects many additional processes in the neuron. For example, it reduces the phosphorylation state of CREB, which may initiate some of the longer-term changes in locus coeruleus function. Upward bold arrows summarize effects of chronic morphine administration in the locus coeruleus. Chronic morphine increases concentrations of types I and VIII adenylyl cyclase (AC I and VIII), PKA catalytic (C) and regulatory type II (RII) subunits, and several phosphoproteins, including CREB. These changes contribute to the altered phenotype of the drug-addicted state. For example, the intrinsic excitability of locus coeruleus neurons is increased by enhanced activity of the cAMP pathway and Na+-dependent inward current, which contributes to the tolerance, dependence, and withdrawal exhibited by these neurons. Up-regulation of type VIII adenylyl cyclase is mediated by CREB, whereas up-regulation of type I adenylyl cyclase and of the PKA subunits appears to occur by means of a CREB-independent mechanism not yet identified.
, PKA catalytic (C) and regulatory type II (RII) subunits, and several phosphoproteins, including CREB. These changes contribute to the altered phenotype of the drug-addicted state. For example, the intrinsic excitability of locus coeruleus neurons is increased by enhanced activity of the cAMP pathway and Na+-dependent inward current, which contributes to the tolerance, dependence, and withdrawal exhibited by these neurons. Up-regulation of type VIII adenylyl cyclase is mediated by CREB, whereas up-regulation of type I adenylyl cyclase and of the PKA subunits appears to occur by means of a CREB-independent mechanism not yet identified.")
17
39wk 137wk 39 wk Cerebral phosphorus metabolite abnormalities in opiate-dependent polydrug abusers in methadone maintenance Psychiatry Research: Neuroimaging Volume 90, Issue 3 , 30 June 1999, Pages Kaufman,M Phosphorous MR Spectroscopy Fig. 3. Metabolite levels in control subjects (n=16) and in short- (n=7) and long-term (n=8) methadone maintenance treatment (MMT) subgroups. Shown are means±S.D. of percent metabolite measures. Post hoc Scheffé test results: *P<0.05 vs. control subjects; **P<0.01 vs. control subjects; ***P< vs. control subjects ;†P<0.05 vs. long-term MMT group
 and in short- (n=7) and long-term (n=8) methadone maintenance treatment (MMT) subgroups. Shown are means±S.D. of percent metabolite measures. Post hoc Scheffé test results: *P<0.05 vs. control subjects; **P<0.01 vs. control subjects; ***P< vs. control subjects ;†P<0.05 vs. long-term MMT group.")
18
From these data, we conclude that polydrug abusers in MMT have 31P-MRS results consistent with abnormal brain metabolism and phospholipid balance. The nearly normal metabolite profile in long-term MMT subjects suggests that prolonged MMT may be associated with improved neurochemistry. Psychiatry Research: Neuroimaging Volume 90, Issue 3 , 30 June 1999, Pages

19
Distribution of Opioid Treatment Programs (OTPs)
2002 SAMHSA/CSAT

20
581 Male Heroin Addicts Followed for 33yrs
The natural history of narcotics addiction among a male sample (N = 581). From: Yih-Ing, et. al., A 33-Year Follow-up of Narcotics Addicts. Archives of General Psychiatry, 58: )
. From: Yih-Ing, et. al., A 33-Year Follow-up of Narcotics Addicts. Archives of General Psychiatry, 58: )")
23
Medical Maintenance Admission Criteria
At least 4 years in MMTP Negative urines for last 3 years Working/School etc. Adequate income for fees Recommendation from clinic Not in military reserves Stable and safe storage environment

24
Medical Maintenance Procedures
Patient given 28 day supply of methadone, by MD,in disket form, every 4 weeks. Medication prepared by hospital pharmacy in usual Rx type bottle and label Routine urine toxicologies Patient returns before “run out” date Primary care provided

25
Methadone Maintenance Total duration in years N = 233 patients
4/05 Duration in years

26
Medical Maintenance Total Duration in Years N= 233 patients
4/05 Duration in years

27
Medical Maintenance--Dosage
Average = 75mg./day Median = 80mg./day Range = 5mg mg./day 30% Split Dose 04/ N=223

28
Medical Maintenance 1983 - Present
347 =Total Enrolled Withdrew 22 (6%) MMTP 41(12%) Active 184 (53%) Deaths 59 (17%) TransferMMTP 7 Cocaine 19 Cause 22 23 14 4 9 1 2 - Tobacco - Hepatitis C - Lymphoma - Medical - HIV Old Age -Homi/Suicide -Prostate Ca Leukemia Buprenorphine 24 Deaths: 1 Tob 1 Hep C Pain 9 9 liver transplants 8 patients 4 alive Revised –06/16/09 10
 MMTP. 41(12%) Active. 184 (53%) Deaths. 59 (17%) TransferMMTP. 7. Cocaine. 19. Cause Tobacco. - Hepatitis C. - Lymphoma. - Medical. - HIV. Old Age. -Homi/Suicide. -Prostate Ca. Leukemia. Buprenorphine 24. Deaths: 1 Tob 1 Hep C. Pain liver transplants. 8 patients. 4 alive. Revised –06/16/")
30
Prevalence of HIV-1 (AIDS Virus) Infection in Intravenous Drug Users New York City: Study: Protective Effect of Methadone Maintenance Treatment 50 – 60% Untreated, street heroin addicts: Positive for HIV-1 antibody 9% Methadone maintained since<1978 (beginning of AIDS epidemic): less than 10% positive for HIV-1 antibody Kreek , 1984; Des Jarlais et al., 1984; 1989
: less than 10% positive for HIV-1 antibody. Kreek , 1984; Des Jarlais et al., 1984;")
31
New York Times

32
Dry Mouth Decay, Crave Sugary Drinks, Brushing/Flossing, Caustic Ingredients
Grinding/Clenching Teeth,

33
STIGMA--METHADONE “My Wife’s Opinion Is That Methadone Maintenance Treatment Is As Close To Evil As You Can Get, Without Killing Someone.” A “successful” methadone patient quoting his wife’s attitude toward methadone treatment

34
U.S. Drug Enforcement Administrative Agent Joanne Masur, one of the last government witnesses in the case against Shinderman, took the stand Friday in U.S. District Court in Portland. Masur, whose job is preventing the diversion of prescription drugs to the black market, said she consulted with Shinderman on at least two occasions. But she said she had no bias against him or his clients, although she said she may have referred to them as "dirt bags." "That is a term I use," she said. "But it's not necessarily derogatory." Portland Press Herald, 7/15/06

35
Crane collapses in busy New York street, killing seven in worst construction accident in recent memory'

36
SUBSTITUTION TREATMENT
SUBSTITUTION TREATMENT ??????? Helpful/Harmful “Substituting one addiction for another”

37
3/19/08 Critics say methadone simply replaces one dependency with another, and some say methadone can be even harder to quit than heroin. Scottish Conservative Party justice spokesman, Bill Aitken, recently described many of those in methadone programmes in Scotland as “sitting fat, dumb and happy" on the drug.

38
Percent Change in Distribution of Methadone and Three Comparison Drugs, 1998--2002
Percent Change from Baseline Year 1998 This slide illustrates the recent increase in distribution of methadone. MMT programs for addiction and pain therapy are the two uses of methadone. Distribution of methadone through MMT programs remained relatively flat during this period suggesting the increase in distribution was primarily for analgesia. Center for Substance Abuse Treatment, Methadone-Associated Mortality: Report of a National Assessment, May 8-9, SAMHSA Publication No Rockville, MD: Center for Substance Abuse Treatment, SAMHSA, 2004.

39
54% 390%

40
Methadone Deaths Not Linked to Misuse of Methadone from Treatment Centers
The consensus report, “Methadone-Associated Mortality, Report of a National Assessment”, concludes that “although the data remain incomplete, National Assessment meeting participants concurred that methadone tablets and/or diskettes distributed through channels other than opioid treatment programs most likely are the central factor in methadone-associated mortality.” The panel based it conclusion that methadone is coming from other sources on data showing that the greatest growth in methadone distribution in recent years is associated with its use as a prescription analgesic prescribed for pain, primarily in solid tablet or diskette form, and not in the liquid formulations that are the mainstay of opioid treatment programs that treat patients with methadone for abuse of heroin or prescription pain killers. The experts surmise that current reports of methadone deaths involve one of three scenarios: illicitly obtained methadone used in excessive or repetitive doses in an attempt to achieve euphoric effects; methadone, either licitly or illicitly obtained, used in combination with other prescription medications, such as benzodiazepines (anti-anxiety medications), alcohol or other opioids; or an accumulation of methadone to harmful serum levels in the first few days of treatment for addiction or pain, before tolerance is developed SAMHSA--2004
, alcohol or other opioids; or an accumulation of methadone to harmful serum levels in the first few days of treatment for addiction or pain, before tolerance is developed. SAMHSA")
41
JAMA 2000:283:

42
Survival Function by Treatment Group
Sees, K. L. et al. JAMA 2000;283: Copyright restrictions may apply.

43
Proportion of Participants Using Heroin and Mean Days of Heroin Use in Previous 30 Days
Sees, K. L. et al. JAMA 2000;283: Copyright restrictions may apply.

44
Buprenorphine Maintenance/Withdrawal: Retention
20 15 Remaining in treatment (nr) 10 1. This figure shows treatment retention, which was significantly better for the maintenance (buprenorphine) vs. control (withdrawal followed by placebo) group. All placebo patients who dropped out did so following relapse to drug use (as determined by urine testing). In the maintenance group, one patient dropped out of treatment, and four were discharged due to relapse in their drug use. 2. Urine results showed that 74.8% of samples were negative for drugs in the buprenorphine maintenance group over the course of the year. 5 Control Buprenorphine 50 100 150 200 250 300 350 Treatment duration (days) (Kakko et al., 2003)
 This figure shows treatment retention, which was significantly better for the maintenance (buprenorphine) vs. control (withdrawal followed by placebo) group. All placebo patients who dropped out did so following relapse to drug use (as determined by urine testing). In the maintenance group, one patient dropped out of treatment, and four were discharged due to relapse in their drug use. 2. Urine results showed that 74.8% of samples were negative for drugs in the buprenorphine maintenance group over the course of the year. 5. Control. Buprenorphine Treatment duration (days) (Kakko et al., 2003)")
45
Kakko et al, Lancet Feb 22, 2003 Buprenorphine Maintenance/Withdrawal: Mortality Placebo Buprenorphine Cox regression Dead 4/20 (20%) 0/20 (0%) 2=5.9; p=0.015 1. While not the primary goal of the study, the study noted that four of the patients who underwent a withdrawal (which was inpatient, and lasted six days) had died after one year -- compared to none of the patients in the buprenorphine maintenance group.
 0/20 (0%) 2=5.9; p= While not the primary goal of the study, the study noted that four of the patients who underwent a withdrawal (which was inpatient, and lasted six days) had died after one year -- compared to none of the patients in the buprenorphine maintenance group.")
46
Transitioning Stable Methadone Maintenance Patients to Buprenorphine Maintenance
Edwin A. Salsitz, M.D., FASAM Beth Israel Medical Center New York City 46

47
Why Transition From Methadone?
Office-based availability Less than monthly visits Different side effect profile Possible diminished stigma Geographic Flexibility

48
Why Not Transition? May not be as effective for individual
Fear of destabilization Transition difficult Opioid withdrawal required May precipitate withdrawal Less social and psychological services Insurance/cost Satisfied with methadone “If it Ain’t Broke….”

49
Subjects MMM eligibility requirements
4 years in Methadone Maintenance Treatment Program (MMTP) 3 years of illicit drug abstinence No excessive drinking Employment/Education, etc. Emotional stability 6/03 - 1/08 patients on methadone ≤ 80 mg/day offered transition to buprenorphine Johnson RE, Chutuape MA, et al. A comparison of levomethadyl acetate, buprenorphine, and methadone for opioid dependence. N Engl J Med. 2000;343:1290–1297. 49
 3 years of illicit drug abstinence. No excessive drinking. Employment/Education, etc. Emotional stability. 6/03 - 1/08 patients on methadone ≤ 80 mg/day offered transition to buprenorphine. Johnson RE, Chutuape MA, et al. A comparison of levomethadyl acetate, buprenorphine, and methadone for opioid dependence. N Engl J Med. 2000;343:1290–")
50
Transfer Patients given option to taper methadone to 30-40 mg/day
Standard protocol used Patients abstained from methadone for hours First buprenorphine/naloxone dose given when Clinical Opiate Withdrawal Scale (COWS) score indicated withdrawal Stabilized over following week Center for Substance Abuse Treatment. Clinical guidelines for the use of buprenorphine in the treatment of opioid addiction. Treatment Improvement Protocol Series (TIPS) 40. Department of Health and Human Services Publication #SMA Rockville, MD: Substance Abuse and Mental Health Services Administration, 2004. 50
 score indicated withdrawal. Stabilized over following week. Center for Substance Abuse Treatment. Clinical guidelines for the use of buprenorphine in the treatment of opioid addiction. Treatment Improvement Protocol Series (TIPS) 40. Department of Health and Human Services Publication #SMA Rockville, MD: Substance Abuse and Mental Health Services Administration,")
51
Study Participants 102 MMM patients offered buprenorphine
23 (22.5%) accepted Two stable MMTP patients referred 104 patients total-25 (24.0%) accepted Reasons for not wanting to switch no perceived advantage of switching concern about efficacy concern about side effects (withdrawal)
 accepted. Two stable MMTP patients referred. 104 patients total-25 (24.0%) accepted. Reasons for not wanting to switch. no perceived advantage of switching. concern about efficacy. concern about side effects (withdrawal)")
52
Outcomes 25/25 patients successfully stabilized on buprenorphine (100%) Average buprenorphine dose mg (S.D. 7.6) Average time on buprenorphine maintenance months (S.D. 16.5)
")
53
Methadone Dose Compared to Buprenorphine Dose
40 35 30 25 Final buprenorphine dose mg/day 20 15 10 5 10 20 30 40 50 60 70 80 90 Baseline methadone dose mg/day Low-moderate correlation - Spearman rank order coefficient = 0.46, p = 0.02 53

54
Positive Experiences No stabilized subjects elected to return to methadone Less frequent office visits every months, not monthly several patients moved further away from program 24/25 patients reported feeling “clearer”

55
Unsuccessful Transfers
5 initially reluctant patients agreed to attempt conversion All unsuccessful Duration of buprenorphine treatment - 1 dose to 5 days Returned to methadone without event 2 cases - “dysphoria” 3 cases – no reason listed 55

56
Study Strengths Subjects
Unique population in research Findings applicable to stable methadone maintained patients seeking transfer to Buprenorphine Very long follow-up period - absence of negative outcomes 56

57
CONCLUSIONS Buprenorphine is viable maintenance treatment for stable patients on methadone doses up to 80 mg/day Transitioning generally well tolerated Buprenorphine efficacious and safe long-term Low to moderate association between methadone and buprenorphine doses

58
Admission EKG QTc~ 600 msec.

60
QTc ~ 440 msec. Off methadone x 1 Week
Bupe started

62
Russia Scorns Methadone for Heroin Addiction Science Times 7-22-08, Michael Schwartz
After the conference in February, which Dr. Mendelevich helped organize, Moscow’s legislature began an inquiry into whether he had engaged in “drug propaganda,” and it called on prosecutors to open a case against him, he said At the same AIDS conference, Dr. Gennady G. Onishchenko, the country’s chief sanitary doctor, the equivalent of surgeon general, said health officials “are not convinced that this is effective,” and added, “There is little optimism for legalizing methadone therapy in the near future.” “Scientific arguments, evidence-based data, are not convincing them,” said Evgeny M. Krupitsky, the head of a laboratory that conducts research on drug addiction at St. Petersburg State Pavlov Medical University. Russian methodology regarding opiate addiction “is not evidence-based,” but relies on “subjective opinions of major leaders in this field.

63
DRUG PROBLEM Patients in a program for heroin addiction in Yekaterinburg, Russia, run by a nongovernmental group.

65
MEDICATION ASSISTED ADDICTION TREATMENT
“All Treatments Work For Some People/Patients” “No One Treatment Works for All People/Patients” Alan I. Leshner, Ph.D Former Director NIDA

Similar presentations














 Matt Wolfe>")




 The anatomy of the reward pathway defines the road to drug abuse (?) Cellular.>")




 Medical University of Sofia, Faculty of Medicine Department of Pharmacology and Toxicology.>")
