Download presentation
Presentation is loading. Please wait.

1
Low Back Pain Dabbas W, M.D. Neurosurgeon
Dept. of Neurosciences, School of Medicine, Al Balqa University

2
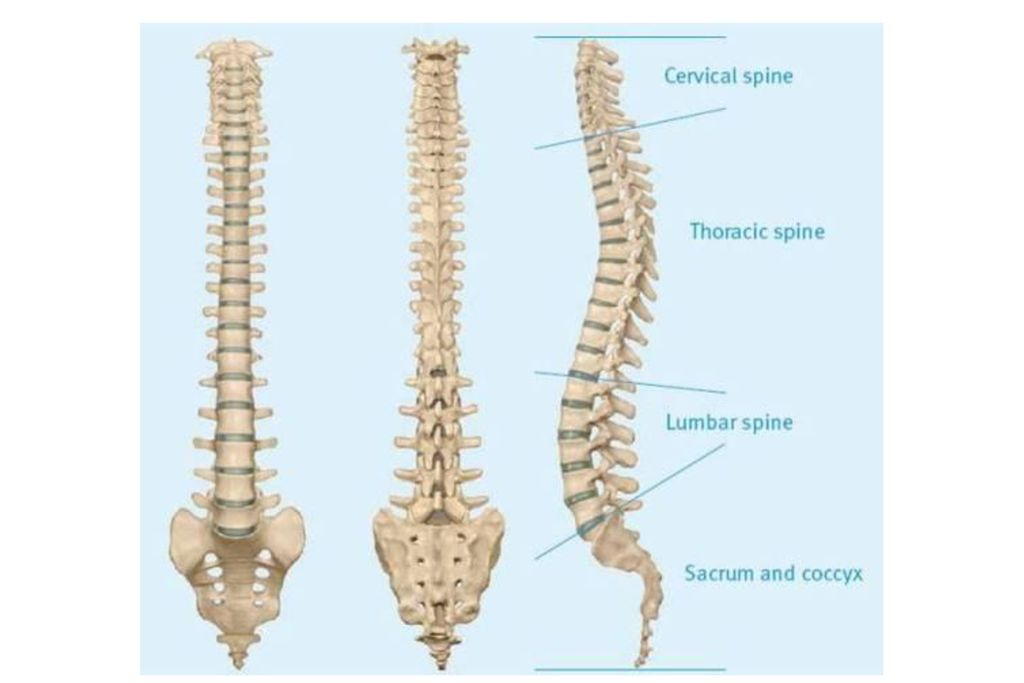
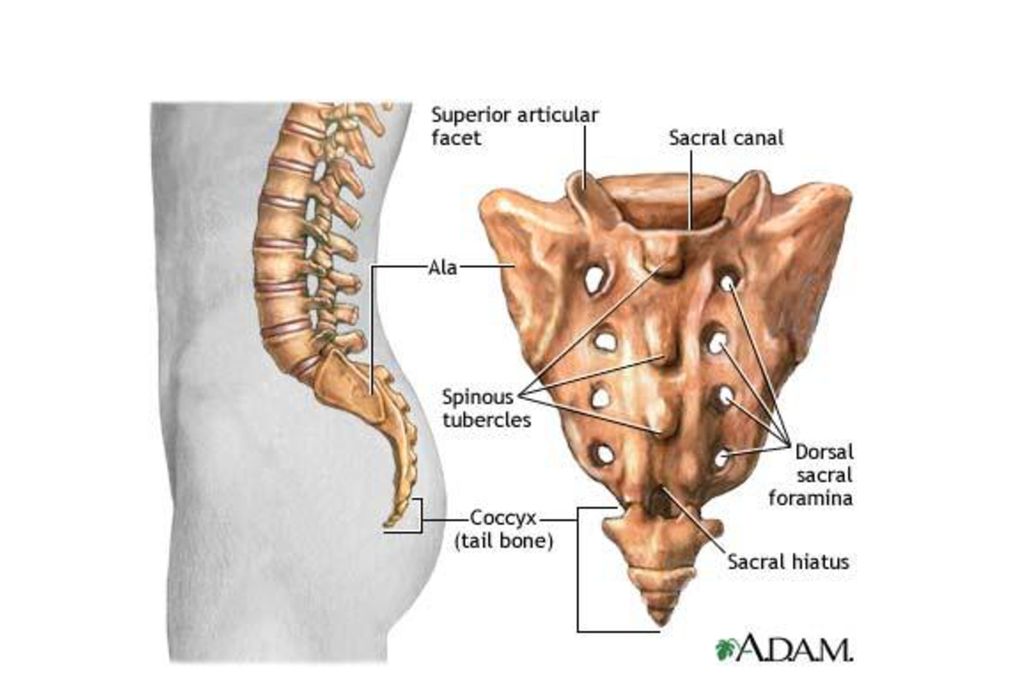
Objectives Review the functional anatomy of lumbo-sacral spine
List essential components of a LBP history, including RED FLAGS Describe common causes of LBP Review proper indications for imaging and referral Review Physical Examination of LS spine Correlate pathology with pertinent physical findings

3
Epidemiology Incidence of LBP: 60-90 % lifetime incidence
5 % annual incidence 90 % of cases of LBP resolve without treatment within weeks 40-50 % LBP cases resolve without treatment in 1 week 75 % of cases with nerve root involvement can resolve in 6 months LBP and lumbar surgery are: 2nd and 3rd highest reasons for physician visits 5th leading cause for hospitalization 3rd leading cause for surgery

4
Disability Age and LBP: Prevalence rate:
Leading cause of disability of adults < 45 years old Third cause of disability in those > 45 years old Prevalence rate: Increased 140 % from to 2000 with only 125 % population growth Nearly 5 million people in the U.S. are on disability for LBP

5
Lifetime Return to Work
Success of < 50 % if off work > 6 months 25 % success rate if off work > 1 year Nearly 0 % success if return to work has not occurred in 2 years

6
Differential Diagnoses
Lumbar Strain Disc Bulge / Protrusion / Extrusion producing Radiculopathy Degenerative Disc Disease (DDD) Spinal Stenosis Spondyloarthropathy Spondylosis Spondylolisthesis Sacro-iliac Dysfunction
 Spinal Stenosis. Spondyloarthropathy. Spondylosis. Spondylolisthesis. Sacro-iliac Dysfunction.")
7
Frequency of Back Pain Types
97% “mechanical”

8
Better anatomy knowledge = Better diagnoses and treatments

11
Vertebra Body, anteriorly Vertebral arch, posteriorly
Functions to support weight Vertebral arch, posteriorly Formed by two pedicles and two laminae Functions to protect neural structures

13
Biomechanics 20% Posterior 80% Anterior
The rule of Spine loading

14
Ligaments Anterior longitudinal ligament
Posterior longitudinal ligament Ligamentum flavum Interspinous ligament Supraspinous ligament

15
Ligamentous Anterior longitudinal ligament

17
Sciatica is defined as…
Pain radiating up the back Pain radiating to the thigh Pain radiating below the knee Pain in the butt

18
L4 L5 S1

19
PATIENT HISTORY “OPQRSTU”
Onset Palliative/Provocative factors Quality Radiation Severity/Setting in which it occurs Timing of pain during day Understanding - how it affects the patient Onset Palliative/Provocative factore Quality Radiation Severity/Setting in which it occurs Timing of pain during day Understanding - how it affects the patient

20
“Red Flags” in back pain
Age < 15 or > 50 Fever, chills, UTI Significant trauma Unrelenting night pain; pain at rest Progressive sensory deficit Neurologic deficits Saddle-area anesthesia Urinary and/or fecal incontinence Major motor weakness Unexplained weight loss Hx or suspicion of Cancer Hx of Osteoporosis Hx of IV drug use, steroid use, immunosuppression Failure to improve after 6 weeks conservative tx

21
Onset Acute - Lift/twist, fall, MVA
Subacute - inactivity, occupational (sitting, driving, flying) Pain effect on: work/occupation sport/activity (during or after)
 Pain effect on: work/occupation. sport/activity (during or after)")
22
Other History Prior h/o back pain Prior treatments and response
Exercise habits Occupation/recreational activities Cough/valsalva exacerbation

23
Diagnoses & Red Flags Cancer Infection Fracture Cauda Equina Syndrome
Age > 50 History of Cancer Weight loss Unrelenting night pain Failure to improve Infection IVDU Steroid use Fever Fracture Age >50 Trauma Steroid use Osteoporosis Cauda Equina Syndrome Saddle anesthesia Bowel/bladder dysfunction Loss of sphincter control Major motor weakness

24
Physical Examination Inspection Palpation Strength testing
Neurologic examination Special tests

25
Approach to LBP History & physical exam Classify into 1 of 4:
LBP from other serious causes Cancer, infection, cauda equina, fracture LBP from radiculopathy or spinal stenosis Non-specific LBP Non-back LBP Workup or treatment

26
Diagnostic Tools 1. Laboratory:
Performed primarily to screen for other disease etiologies Infection Cancer Spondyloarthropathies No evidence to support value in first month unless with red flags Specifics: WBC ESR or CRP HLA-B27 Tumor markers: Kidney Breast Lung Thyroid Prostate

27
Radiographs: Pre-existing Degenerative Joint Disease (Osteoarthritis) is most common diagnosis Usually 3 views adequate with obliques only if equivocal findings Indications: History of trauma with continued pain < 20 years or > 55 years with severe or persistent pain Noted spinal deformity on exam Signs / symptoms suggestive of spondylo-arthropathy Suspicion for infection or tumor

29
3. Electromylogram (EMG):
Measures muscle function Would not be appropriate in clinically obvious radiculopathy 4. Bone Scan: Very sensitive but nonspecific Useful for: Malignancy screening Detection for early infection Detection for early or occult fracture

31
Myelogram: Procedure of injecting contrast material into the spinal canal with imaging via plain radiographs versus CT

32
6. CT with Myelogram: Can demonstrate much better anatomical detail than Myelogram alone Utilized for: Demonstrating anatomical detail in multi-level disease in pre-operative state Determining nerve root compression etiology of disc versus osteophyte Surgical screening tool if equivocal MRI or CT

33
7. CT: Best for bony changes of spinal or foraminal stenosis
Also best for bony detail to determine: Fracture Degenerative Joint Disease (DJD) Malignancy
 Malignancy.")
34
9. MRI Best diagnostic tool for: Soft tissue abnormalities: Infection
Bone marrow changes Spinal canal and neural foraminal contents Emergent screening: Cauda equina syndrome Spinal cord injury Vascular occlusion Radiculopathy Benign vs. malignant compression fractures Osteomyelitis evaluation Evaluation with prior spinal surgery

35
Break for Physical Examination Hands-on Session

36
Inspection Observe for areas of erythema Unusual skin markings
Infection Long-term use of heating element Unusual skin markings Café-au-lait spots Neurofibromatosis Hairy patches, lipomata Tethered cord Dimples, nevi (spina bifida)
")
37
Inspection (cont.) Posture Normal lumbar lordosis
Shoulders and pelvis should be level Bony and soft-tissue structures should appear symmetrical Normal lumbar lordosis Exaggerated lumbar lordosis is common characteristic of weakened abdominal wall

38
Neurologic Examinaion
Includes an exam of entire lower extremity, as lumbar spine pathology is frequently manifested in extremity as altered reflexes, sensation and muscle strength Describes the clinical relationship between various muscles, reflexes, and sensory areas in the lower extremity and their particular cord levels

39
PID L3-L4 L4-L5 L5-S1 Compressed root L4 L5 S1 % 5-10% 40-45%
Reflex affected Knee - Ankle jerk Motor Q. Femoris (knee ex) EHL & tibialis (foot drop) Gastrocnemius (plantarflexion) Sensory M. maleolus Dorsum of foot L. maleolus
 EHL & tibialis (foot drop) Gastrocnemius (plantarflexion) Sensory. M. maleolus. Dorsum of foot. L. maleolus.")
40
Neurologic Examination (T12, L1, L2, L3 level)
Motor Iliopsoas - main flexor of hip With pt in sitting position, raise thigh against resistance Reflexes - none Sensory Anterior thigh

41
Neurologic Examination (L2, L3, L4 level)
Motor Quadriceps - L2, L3, L4, Femoral Nerve Hip adductor group - L2, L3, L4, Obturator N. Reflexes Patellar - supplied by L2, L3, and L4, although essentially an L4 reflex and is tested as such

42
L2, L3, L4 testing

43
Neurologic Examination (L4 level)
Motor Tibialis Anterior Resisted inversion of ankle Reflexes Patellar Reflex (L4) Sensory Medial side of leg
 Sensory. Medial side of leg.")
45
Neurologic Examination (L5 level)
Motor Extensor Hallicus Longus Resisted dorsiflexion of great toe dorsifexion Reflexes - none Sensory Dorsum of foot in midline

47
Neurologic Examination (S1 level)
Motor Peroneus Longus and Brevis Resisted eversion of foot Planter flexion Reflexes Achilles Sensory Lateral side of foot

49
Special Tests Tests to stretch spinal cord or sciatic nerve
Tests to increase intrathecal pressure Tests to stress the sacroiliac joint

50
Tests to Stretch the Spinal Cord or Sciatic Nerve
Straight Leg Raise Cross Leg SLR Kernig Test

52
Kernig Sign Pain relieved Pain present

53
Test to increase intrathecal pressure
Valsalva Maneuver Reproduction of pain suggestive of lesion pressing on thecal sac

54
Tests to stress the Sacroiliac Joint
FABER Test

55
FABER test: Flexion A- Bduction External Rotation

56
Disc Degeneration: Findings?
Narrowing Osteophyts Endplate sclerosis

57
Degeneration & Tears

58
Disc Classification Normal Bulge Canal Protrusion Extrusion Disc
Bony Endplate Normal Bulge Disc Classification Protrusion Extrusion

59
Bulging

60
Protrusion

61
Protrusion

62
Extrusion

63
Extrusion

64
Extrusion

65
Treatment Pharmacological NSAIDS Muscle relaxents:
Re-establish sleep patterns More useful in myofascial/muscular pain Membrane stabilizers TCA / Neurontin Re-establish sleep pain Reduce radicular dysesthesias Narcotics: rarely indicated Morphine, Oxy/hydrocodone, Oxymorphone, Hydromorphone, Fentanyl, Methadone Steroids: more useful for radiculitis Non-narcotic analgesics: Ultram (Tramadol)
")
66
Injections (Neural blockade)
Physical Therapy Modalities Electrical Stimulation/TENS Postural Education / Body Mechanics Massage / Mobilization / Myofascial Release Stretching / Body Work Exercise / Strengthening Traction Pre-conditioning / Work-conditioning Injections (Neural blockade) Epidural blocks Facet blocks Trigger point SI joint
 Epidural blocks. Facet blocks. Trigger point. SI joint.")
67
Epidural Steroid Injections
Indicated for radiculopathy not responding to conservative management Conflicting evidence Small improvement up to 3 months Less effective in spinal stenosis

69
Surgery Laminectomy Hemilaminectomy Discectomy Fusion Instrumented
Non-instrumented fusion Minimally Invasive Spine Surgery (MISS) Kyphoplasty Percutaneous Disc Decompression (PDD)
 Kyphoplasty. Percutaneous Disc Decompression (PDD)")
70
Management of an acute low back muscle strain should consist of all the following EXCEPT:
X-rays to rule out a fracture Educate the patient on generally good prognosis Non-opiate analgesics Remain active

71
Your patient with LBP has paresthesias in the lateral foot, decreased toe-raise strength, diminished sensation lateral foot, and diminished Achilles reflex. This is suggestive of dysfunction of which nerve root? L4 L5 S1 S2

72
Thank you

Similar presentations