Download presentation
Presentation is loading. Please wait.

1
Diagnosis and Management of Common Electrolyte Disorders
Eric I. Rosenberg, MD, MSPH, FACP Rev 11/06 electrolytes1106

2
Objectives To discuss diagnostic and therapeutic strategies for:
Hyponatremia Hypernatremia Hyperkalemia Hypokalemia

3
Case 1 60 year old man “Admit for weakness and hyponatremia”
[Na+] 120 mg/dL

5
Clinical Evaluation History Physical Labs Symptomatic? Predisposed?
Medications? IVF’s? Physical Volume status? Labs Confirm (if unusually abnormal) Context Additional diagnostic tests
 Context. Additional diagnostic tests.")
6
Case 1 (cont’d) Nausea, weak, confused x 1 week HTN, CHF
JVD, crackles (rales), edema Na+ 120 mEq/L BUN 93 mg/dL Cr 3 mg/dL Glucose 135 mg/dL Albumin 2.9 mg/dL Plasma osm 252 mOsm/kg Urine osm 690 mOsm/kg
, edema. Na+ 120 mEq/L. BUN 93 mg/dL. Cr 3 mg/dL. Glucose 135 mg/dL. Albumin 2.9 mg/dL. Plasma osm 252 mOsm/kg. Urine osm 690 mOsm/kg.")
7
“Choose the most appropriate treatment”
3% I.V. NaCl 0.9% I.V. NaCl 50 mg hydrochlorothiazide daily Salt and water restriction Demeclocycline

8
Differential diagnosis

9
Hyponatremia usually reflects excessive H20

10
Common Differential Dx
Decreased Water Excretion GFR Kidney perfusion SIADH Addison’s Disease Malnutrition *Pseudohyponatremia ±Psychogenic (>1 L / hour) Prompt them for answers *100mg/dL glucose increase 1.6 mEq/L [Na] decrease ± Urine specific gravity < 1.003
 Prompt them for answers. *100mg/dL glucose increase 1.6 mEq/L [Na] decrease. ± Urine specific gravity <")
11
COMMON CAUSES of HYPONATREMIA
History: predisposing features Exam: volume status (including orthostatics supine/standing) BMP; Urinalysis; Serum Osmolality; (Urine Sodium; Urine Osmolality) Head C.T. (if symptomatic) Other imaging/labs to evaluate CV, Renal, Endocrine systems as needed
 BMP; Urinalysis; Serum Osmolality; (Urine Sodium; Urine Osmolality) Head C.T. (if symptomatic) Other imaging/labs to evaluate CV, Renal, Endocrine systems as needed.")
12
Complications of Treating Hyponatremia
Delayed treatment Cerebral edema Permanent neurological injury Death Inappropriately rapid treatment Cerebral dehydration/demyelination Inappropriate treatment Failure to improve morbidity Delayed improvement morbidity Further deterioration

13
Common Treatment Options
Water restriction Diuresis (with loop diuretic) Volume infusion (with crystalloid) Hypertonic saline Demeclocycline
 Volume infusion (with crystalloid) Hypertonic saline. Demeclocycline.")
14
What if he had cerebral edema?
Correct [Na+] to mEq/L to temporarily relieve edema [Na+] should NOT increase by more than mEq/L in 1st 24 hours Slow/Stop infusion as soon as symptoms improve

15
3% NaCl Calculation [Na+] = 116 mEq/L
Goal [Na+] = 125 mEq/L at 24 hours Amount of Na+ to be given as 3% infusion: = [Serum Na+ (desired) – Serum Na+(measured) ] (TBW) = [125 – 116] [(0.5)(60kg)] = 270 mEq Na+ 3% saline = 513 mEq sodium/L 270/513 = 0.5 L = 500 ml over 24 hrs.
![3% NaCl Calculation [Na+] = 116 mEq/L](http://slideplayer.com/slide/1661765/7/images/15/3%25+NaCl+Calculation+%5BNa%2B%5D+%3D+116+mEq%2FL.jpg "Goal [Na+] = 125 mEq/L at 24 hours. Amount of Na+ to be given as 3% infusion: = [Serum Na+ (desired) – Serum Na+(measured) ] (TBW) = [125 – 116] [(0.5)(60kg)] = 270 mEq Na+ 3% saline = 513 mEq sodium/L. 270/513 = 0.5 L = 500 ml over 24 hrs.")
16
Hyponatremia: Key Points
127 mEq/L Excess water If symptomatic, treat rapidly Slowly correct [Na+] *towards* normal Find the underlying cause

17
Case 2 40 y/o woman s/p hypertensive brain hemorrhage 2 weeks ago.
This morning she’s less responsive. What may have caused this new problem?

18
Stuporous BP 150/70, HR 94 Dry mouth, poor turgor Na 160 mEq/L; K 2.8 mEq/L; HCO3: 18 mEq/L; Cl 137 mEq/L

19
Differential diagnosis

20
Hypernatremia usually reflects insufficient H20

21
Differential Diagnosis
Lack of water Severe diarrhea Severe burns H20 excretion Osmotic diuresis H20 conservation Diabetes insipidus

22
Guidelines for Hypernatremia Rx
Determine and treat likely cause(s) Most common error is “underguesstimation” of water deficit: TBW x ([Na+(measured)] – [Na+(desired) ])/[Na+ (desired)] Replace H20 enterally if possible Frequent monitoring
 Most common error is underguesstimation of water deficit: TBW x ([Na+(measured)] – [Na+(desired) ])/[Na+ (desired)] Replace H20 enterally if possible. Frequent monitoring.")
23
Sodium Content of IVF’s (mEq/L)
3% saline: 513 0.9% (normal) saline: 154 Ringer’s Lactate: 130 Half Normal (0.45%) saline: 77 5% Dextrose (D5W): 0
 saline: 154. Ringer’s Lactate: 130. Half Normal (0.45%) saline: 77. 5% Dextrose (D5W): 0.")
24
Hypernatremia: Key Points
[Na+] >145 mEq/L Net water loss Calculate the water deficit [Na+] >145 mEq/L Usually inadequate water intake in an obtunded/ill person Increased [Na+] in ECF Water shift from ICF Cerebral shrinkage lethargy, coma, ICH from tearing of bridging veins

25
Case 3 29 y/o man with severe muscle weakness.
No vomiting or diarrhea. Normal physical exam.

26
Na = 141 mEq/L K = 1.4 mEq/L Cl = 116 mEq/L HCO3- = 11 mEq/L pH = 7.25, pCO2 = 21 mmHg

27
Consequences of Hypokalemia [K] <3
Neuromuscular manifestations Weakness, fatigue, rhabdomyolysis, myonecrosis, respiratory failure GI symptoms Constipation, ileus Nephrogenic Diabetes Insipidus Dysrhythmias (if heart disease)
![Consequences of Hypokalemia [K] <3](http://slideplayer.com/slide/1661765/7/images/27/Consequences+of+Hypokalemia+%5BK%5D+%3C3.jpg "Neuromuscular manifestations. Weakness, fatigue, rhabdomyolysis, myonecrosis, respiratory failure. GI symptoms. Constipation, ileus. Nephrogenic Diabetes Insipidus. Dysrhythmias (if heart disease)")
28
Common Causes of Hypokalemia
Malnutrition/NPO Diarrhea (100 mEq/L) Vomiting (volume depletion) DRUGS Thiazides (stimulate excretion) Amphotericin B Penicillins Gentamicin Foscarnet
 Vomiting (volume depletion) DRUGS. Thiazides (stimulate excretion) Amphotericin B. Penicillins. Gentamicin. Foscarnet.")
29
“Choose the most likely diagnosis”
Bartter’s syndrome Laxative abuse Primary aldosteronism Diuretic abuse Distal renal tubular acidosis

30
Less Common Causes Hormonal Renal tubular disease
Primary hyperaldosteronism Adenomas, hyperplasia, ectopic ACTH, ectopic mineralocorticoid (licorice, chaw) Secondary hyperaldosteronism Renal hypoperfusion (CHF, RAS, severe HTN) Renin-secreting tumor Renal tubular disease Type 1 or 2 RTA Bartter’s syndrome (metabolic alkalosis, polyuria) Chronic magnesium depletion Laxative abuse (metabolic alkalosis)
 Secondary hyperaldosteronism. Renal hypoperfusion (CHF, RAS, severe HTN) Renin-secreting tumor. Renal tubular disease. Type 1 or 2 RTA. Bartter’s syndrome (metabolic alkalosis, polyuria) Chronic magnesium depletion. Laxative abuse (metabolic alkalosis)")
31
Hypokalemia Rx Recognize likely total body depletion
1 mEq/L decrease = mEq total deficiency Gradual oral replacement I.V. replacement if serum level less than 3 mEq/L Check & Replace magnesium Consider telemetry

32
Hypokalemia: Key Points
[K+] < 3.5: review medications, review health status [K+] < 3: intervention Recognize Mg+ is cofactor Renal/CV monitoring

33
Case 4 59 y/o man with 3-days malaise, decreased mental acuity and responsiveness, slurred speech. ESRD on hemodialysis; HTN, DM, Hypothyroidism

34
Disoriented and lethargic
BP (supine) 148/79mmHg, HR 101/min (supine) RR 26/min, T 37.7oC. Mucous membranes are moist, neck veins are distended. Bilateral crackles and wheezes. Loud S peripheral edema.
 148/79mmHg, HR 101/min (supine) RR 26/min, T 37.7oC. Mucous membranes are moist, neck veins are distended. Bilateral crackles and wheezes. Loud S4. 3+ peripheral edema.")
37
Begin I.V. infusion of normal saline for volume repletion
What is the next most appropriate step in managing this patient? Begin I.V. infusion of normal saline for volume repletion Administer 1 ampule dextrose and 10 units insulin I.V. for hyperkalemia Transfer to the ICU and perform emergent peritoneal dialysis Transfer to the ICU and perform emergent hemodialysis

38
“Dialysis machine available in 20 minutes”

39
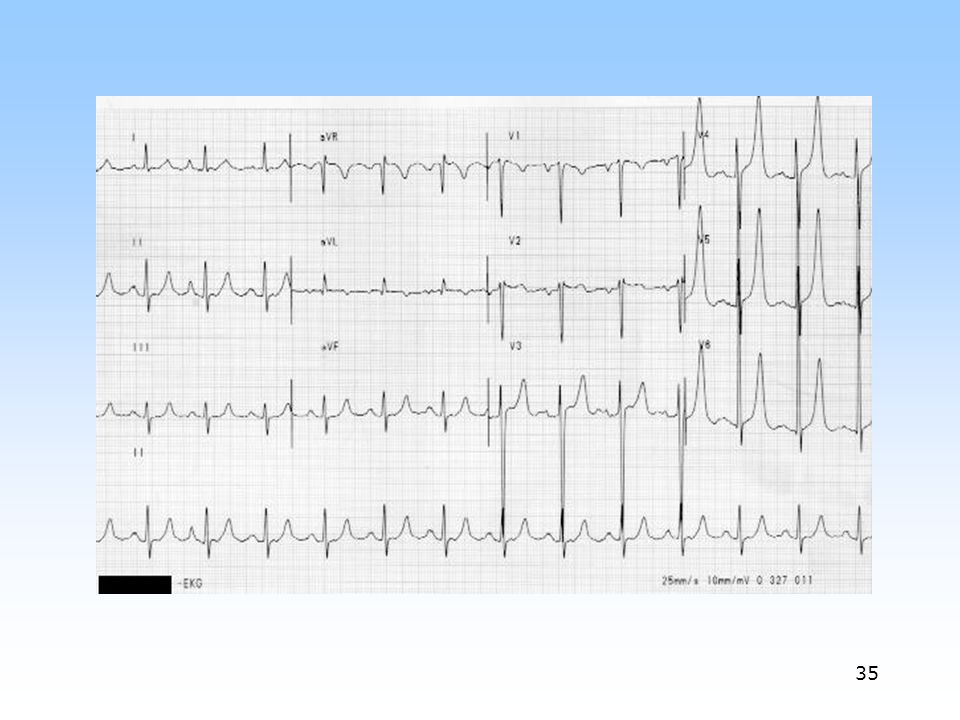
Emergency Treatment [K] > 6 mEq/L
“STAT” ECG “STAT” repeat [K+] Give IV Calcium
![Emergency Treatment [K] > 6 mEq/L](http://slideplayer.com/slide/1661765/7/images/39/Emergency+Treatment+%5BK%5D+%3E+6+mEq%2FL.jpg "STAT ECG. STAT repeat [K+] Give IV Calcium.")
40
Additional Rx More IV Calcium Glucose and Insulin Bicarbonate
Inhaled Beta-2 agonists Sodium polystyrene sulfonate (Kayexalate®)
")
41
Severe hyperkalemia is usually preceded by moderate, uncorrected hyperkalemia

42
Differential Dx Renal Failure (GFR < 10 ml/min) Extra Renal Causes
Metabolic acidosis Cell lysis (chemotherapy, trauma) Salt substitutes, ACE-I/ARB, Addison’s Disease Pseudo (coagulated RBC’s/platelets)
 Salt substitutes, ACE-I/ARB, Addison’s Disease. Pseudo (coagulated RBC’s/platelets)")
43
Hyperkalemia: Key Points
K>4.5: caution with medications, & monitor K>5.5: intervene Calcium (not kayexalate) is 1st line Check ECG
 is 1st line. Check ECG.")
44
SUMMARY Construct your differential Know the complications of therapy
Know the implications of lack of therapy Calculate water/electrolyte needs … But repeated and frequent monitoring is most important. Electrolyte disorders may be a diagnostic clue or an expected consequence of therapy

Similar presentations






>")

>")












