Download presentation
Presentation is loading. Please wait.

1
CRRT Continue Renal Replacement Therapy
CVVH CVVHD CVVHDF

2
Indications In critically ill patients with renal failure and hemodynaemic instability For patients in whom continuous removal of volume or toxic substance is desirable ( as in septic shock , AMI , severe GI bleeding ,ARDS or condition with or at risk for cerebral edema ….)
")
3
Procedure共同處 Driving force : external pump Circuit : Venovenous
Dialysis solutions :一般使用1.5% PD solution Replacement fluid : several types of replacement fluid can be used , depending on patient requirements ,一般使用 pre-dilution 方式.

4
Anti-coagulation 的方式 STANDARD HEPARIN TYPICAL REGIMEN IN CRRT :
Priming of the circuit ( 5000 IU / L ) Initial Heparin Bolus : IU / kg Infuse Heparin at : 5 to 12 IU / kg / hr ACT on post filter : Adjust heparin rate to keep ACT between 1.5 & 2.0 times
 Initial Heparin Bolus : IU / kg. Infuse Heparin at : 5 to 12 IU / kg / hr. ACT on post filter : Adjust heparin rate to keep ACT between 1.5 & 2.0 times.")
5
STANDARD HEPARIN ADVANTAGES Easy to perform Useful method Inexpensive
DISADVANTAGES Occasional Thrombocytopenia Hemorrhagic Risk with Bleeding patient

6
LOW MOLECULAR WEIGHT (LMW) HEPARIN
TYPICAL REGIMEN IN CRRT : Priming of the circuit : 20 mg in 1 L Maintenance dose : 10 to 40 mg q6 hrs Monitor anti- factor Xa (aXa) units . Adjust between 0.1 and 0.4 µ/ml Different Dosages for LMW heparin
 units . Adjust between 0.1 and 0.4 µ/ml. Different Dosages for LMW heparin.")
7
LOW MOLECULAR WEIGHT (LMW) HEPARIN
DISADVANTAGES Expensive Special and difficult monitoring With low doses frequent filter clotting ADVANTAGES Decreased Risk of Bleeding

8
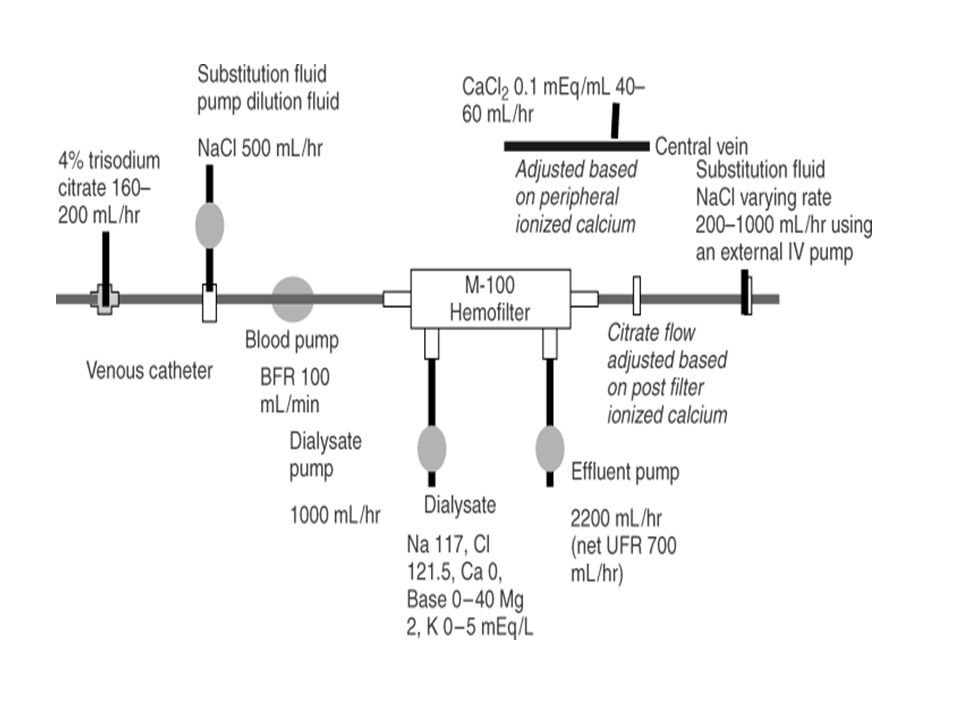
Regional Citrate Anticoagulation
TYPICAL REGIMEN : Citrate anticoagulation is always regional Citrate infusion (4%) at 170 ml/hr initially Special Dialysate at 1 liter/hr ( Na+ 117 , K+ 4 , Mg , Cl , dextrose % , no Ca++ , no base ) CaCL2 (0.75%) by central I.V at ml/hr, Maintain ionized Ca++ at mmol/L
 at 170 ml/hr initially. Special Dialysate at 1 liter/hr ( Na+ 117 , K+ 4 , Mg , Cl , dextrose % , no Ca++ , no base ) CaCL2 (0.75%) by central I.V at ml/hr, Maintain ionized Ca++ at mmol/L.")
9
Citrate ADVANTAGES : No Bleeding No Thrombocytopenia
Improved Filter Life and Efficacy DISADVANTAGES : Complex for the set up Ca++ monitoring needed Occasional Alkalosis

11
Heparin- free methos Normal saline flush Used in patients with
1. Severe liver disease 2. Acitve or recent bleeding 3. Heparine-induced thrombocytopenia 4. Post-op patients

12
Dialysis modalities in the ICU

13
CVVH配置簡圖 CVVH Continuous Veno-Venous Hemofiltration CVVH 模式下, 置換液流速
P R I S M A CVVH Continuous Veno-Venous Hemofiltration CVVH 模式下, 置換液流速 最高可達4500ml/hr

14
CVVH order l Prepare Heparin 2cc + N/S 3cc, then inject 1.6cc into each femoral cath. l For AK priming: (GAMBRO, Polyarylethersulfone, 6S) *1st N/S 1000cc. *2nd Heparin 2,500U. *3rd N/S 500cc. l *Prepare Heparin 25,000U + N/S 500cc IVD 10cc/hr with pump to keep aPPT 1.5-2 and adjust as followed: aPPT bolus hold dose(cc/hr) <1.0 U min >2.5 min
 <1.0 2000U - 30min -2. >2.5 - 60min -4.")
15
CVVH order If non-heparin , N/S 200cc q ½ hr to rinse the AK
Predilution run 500cc/hr alternately as followed via artery end 1st bottle N/S 500cc + Sinca 1amp 2nd bottle N/S 500cc + 10% MgSO4 4cc 3rd bottle N/S 500cc 4th bottle D5W 500cc + NaHCO3 5amp Warm dialysate to 37C Record I/O and BP q1hr UF target I-O ( ) cc/hr Check BUN,Crea,Na,K,Cl,aPPT q6hr for 1 day & then q8hr. Check Ca,P,Mg qd.
 cc/hr. Check BUN,Crea,Na,K,Cl,aPPT q6hr for 1 day & then q8hr. Check Ca,P,Mg qd.")
16
CVVHD配置簡圖 CVVHD Continuous Veno-Venous Hemodialysis P R I S M A

17
CVVHD order l Prepare Heparin 2cc + N/S 3cc, then inject 1.6cc into each femoral cath. l For AK priming: (GAMBRO, Polyarylethersulfone, 6S) *1st N/S 1000cc. *2nd Heparin 2,500U. *3rd N/S 500cc. l *Prepare Heparin 25,000U + N/S 500cc IVD 10cc/hr with pump to keep aPPT 1.5-2 and adjust as followed: aPPT bolus hold dose(cc/hr) <1.0 U min >2.5 min
 <1.0 2000U - 30min -2. >2.5 - 60min -4.")
18
CVVHD order If non-heparin , N/S 200cc q ½ hr to rinse the AK
1.5% PD solution 500cc/hr run as dailysate Warm dialysate to 37C Record I/O and BP q1hr UF target I-O ( ) cc/hr Check BUN,Crea,Na,K,Cl,aPPT q6hr for 1 day & then q8hr. Check Ca,P,Mg qd.
 cc/hr. Check BUN,Crea,Na,K,Cl,aPPT q6hr for 1 day & then q8hr. Check Ca,P,Mg qd.")
19
CVVHDF配置簡圖 P R I S M A CVVHDF Continuous Veno-Venous Hemodiafiltration

20
CVVHDF order l Prepare Heparin 2cc + N/S 3cc, then inject 1.6cc into each femoral cath. l For AK priming: (GAMBRO, Polyarylethersulfone, 6S) *1st N/S 1000cc. *2nd Heparin 2,500U. *3rd N/S 500cc. l *Prepare Heparin 25,000U + N/S 500cc IVD 10cc/hr with pump to keep aPPT 1.5-2 and adjust as followed: aPPT bolus hold dose(cc/hr) <1.0 U min >2.5 min
 <1.0 2000U - 30min -2. >2.5 - 60min -4.")
21
CVVHDF order If non-heparin , N/S 200cc q ½ hr to rinse the AK
Predilution run 500cc/hr alternately as followed via artery end 1st bottle N/S 500cc + Sinca 1amp 2nd bottle N/S 500cc + 10% MgSO4 4cc 3rd bottle N/S 500cc 4th bottle D5W 500cc + NaHCO3 5amp 1.5% PD solution 500cc/hr run as dailysate Warm predilution and dialysate to 37C Record I/O and BP q1hr UF target I-O ( ) cc/hr Check BUN,Crea,Na,K,Cl,aPPT q6hr for 1 day & then q8hr. Check Ca,P,Mg qd.
 cc/hr. Check BUN,Crea,Na,K,Cl,aPPT q6hr for 1 day & then q8hr. Check Ca,P,Mg qd.")
Similar presentations


>")













>")


