Download presentation
Presentation is loading. Please wait.

1
PREVENTING EMBOLIZATION IN INHERITED ARRHYTHMIA DISORDERS Pedro Brugada, MD, PhD. Chairman Cardiovascular Division UZ-Brussel, Brussels.

2
Why this topic? Inherited arrhythmia disorders: An unknown cause of potential embolization. Guidelines on atrial fibrillation give no recommendations at all regarding inherited arrhythmia disorders (exception: HCM, WPW). NOACs may not be refunded for patients that may benefit the most.
. NOACs may not be refunded for patients that may benefit the most..")
3
EMBOLIZATION IN INHERITED ARRHYTHMIA DISORDERS Atrial: ATRIAL FIBRILLATION – Familial atrial fibrillation – Short QT – Long QT – Brugada syndrome – HCM – PRKAG with HCM or CCM – ANP gene mutations

4
EMBOLIZATION IN INHERITED ARRHYTHMIA DISORDERS Ventricular: STRUCTURAL – Left ventricular non-compaction – Post-op right ventricular dysplasia

5
28 cM I:1I:2 11.7 cM 6.6 cM 0.5 cM FAMILIAL ATRIAL FIBRILLATION REGION SHARED ON 10q2 AFFECTED NON AFFECTED DEAD Familial Atrial Fibrillation

6
Mean Age of Diagnosis18 years Range in age Diagnosis1-35 years EchocardiogramNormal Chronic AF 41/42 Asymptomatic36/42 Anticoagulation:0 No embolization known: Future? FAMILIAL ATRIAL FIBRILLATION CLINICAL FEATURES Familial Atrial Fibrillation

7
SHORT QT syndrome. Atrial fibrillation in 40-45% of cases. Youngest reported case: In utero. No known embolization. Gussak, Brugada P, Brugada J, et al. Cardiology 2000

8
LONG QT SYNDROME Atrial fibrillation: Yes, but incidence unknown Embolization: No reports

9
BRUGADA SYNDROME Atrial fibrillation: 20-25% Embolization: Yes Youngest patients: 3-14 y

10
Spontaneous atrial arrhythmias Paroxysmal atrial fibrillation or SSS may be the first manifestation of Brugada syndrome: AJMALINE TEST! Common cause of inappropriate ICD shocks: 14% of ICD recipients had inappropiate ICD shock because of asymptomatic, undiagnosed AF. Marker of higher risk and/or of disease progress ?

11
ATRIAL FIBRILLATION IN CHILDREN WITH BRUGADA SYNDROME 3/8 pts in 1992 paper were children with AF. 3/3 had SSS and were pacemaker dependent. 2/43 children had total atrial standstill. 1/43 with right and left atriomegally. 4/43 (10%) with atrial fibrillation or flutter.
 with atrial fibrillation or flutter..")
12
Transient ischemic attack in a 71 year-old man

13
First consultation Patient comes for second opinion after TIA Admitted at local hospital during his holidays because of speech difficulties Rx: Aspirine, simvastatine Previous history: Appendicectomy. Similar episode 8 years ago.

14
Admission at University Hospital Full neurological examination: Normal. No carotid stenosis. CT, etc: Normal. Cerebral MRI: Multiple microembolisms Cardiological consultation: Normal, including TEE, Holter, troponine, etc. Diagnosis: Cryptogenic TIA

15
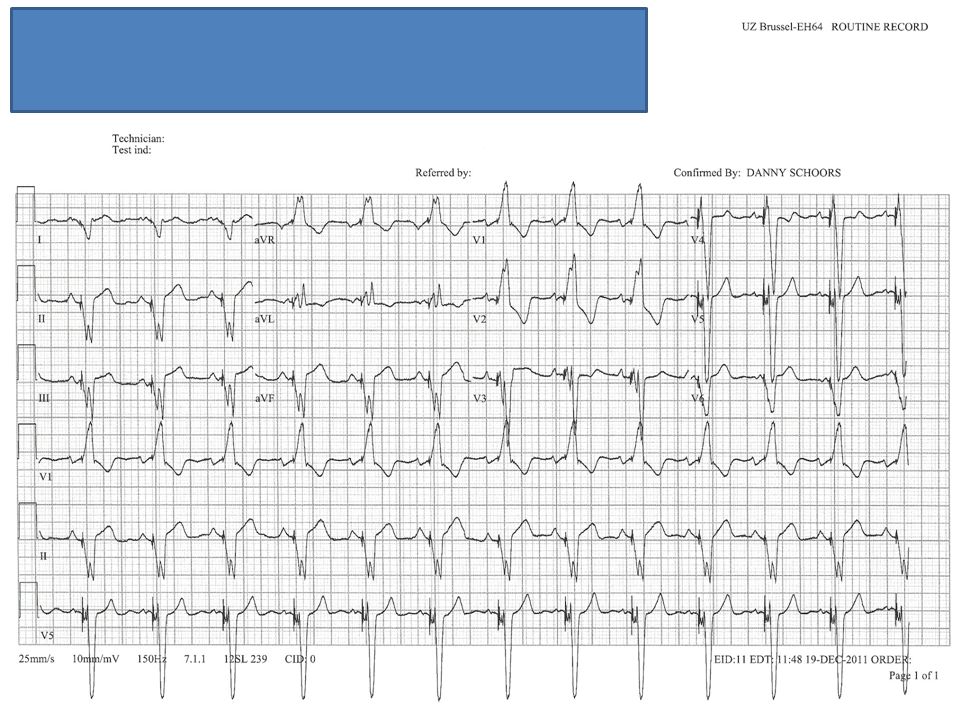
ECG

16
Medical report local hospital

17
ECG

18
ECGs at admission V1

19
Ajmaline test

20
TIA as a first manifestation of Brugada syndrome.

21
Follow-up ECGs

22
Follow-up DDD-ICD implanted. Ablation of cavo-tricuspid isthmus. Anticoagulation, sotalol. No recurrence of AF after 2 years.

23
EMBOLIZATION IN INHERITED ARRHYTHMIA DISORDERS Ventricular: STRUCTURE – Left ventricular non-compaction – Post-op right ventricular dysplasia

24
Left Ventricular Non-compaction.

25
Intratrabecular flow in LVNC

26
Atrial Fibrillation in a 16 year-old boy.

27
AA, born 16-03-1995 1998: diagnosis of left ventricular non-compaction Rx: Metroprolol, asymptomatic. 3/2011: Atrial fibrillation with fatigue and dyspnea Rx: Sotalol (vomiting, low blood pressure) Amiodarone (hyperthyroidism) Verapamil, Lasix, Spirolactone, Warfarine.
 Amiodarone (hyperthyroidism) Verapamil, Lasix, Spirolactone, Warfarine..")
28
Echocardiography DATELA (mm)LVEF (%)SPAP (mmHg) 19-1-2011536340 24-8-2011566170 23-9-2011495970 5-12-2011 (B)573075
LVEF (%)SPAP (mmHg) (B)573075")
29
After optimal medical RX DATELA (mm)LVEF (%)SPAP (mmHg) 19-1-2011536340 24-8-2011566170 23-9-2011495970 5-12-2011 (B)573075 21-12-11- MI 3/4 !4095
LVEF (%)SPAP (mmHg) (B) MI 3/4 !4095")
30
After optimal medical therapy

31
13-12-2011 Severe heart failure with caquexia Persistent atrial fibrillation Diagnosis of LV non compaction confirmed Severe mitral regurgitation with dilatation of the annulus en massive tricuspid insufficiency

32
The longer one waits to initiate a rhythm-control strategy, the harder it is to regain sinus rhythm 1 month P<.02 6 months P<.07 Electrical cardioversion 82% 36% Patients in sinus rhythm (%) 67% 27% <3m
 67% 27% <3m")
33
Electroanatomical mapping

34
CRYOBALLOON ABLATION OF ATRIAL FIBRILLATION

35
Success rate of single procedure catheter ablation PAF ranges from 38% to 78%. Most series > 60%. Persistent AF ranges from 22% to 45%. Most centers < 30%. Success rate of mutiple procedure catheter ablation PAF ranges from 54% to 80%. Most series > 70%. Persistent AF ranges from 37% to 88%. Most centers around 50%. Centre for Heart and Vessel Disease, University Hospital Brussels

36
HYBRID THERAPY FOR ATRIAL FIBRILLATION Simultaneous endo and epicardial ablation. Combination of RF and cryoablation possible. Allows reduction of left atrium dimensions. Allows exclusion of the left atrial appendage. Can be combined with other procedures: Valve repair ICD implantation Success rate in persistent AF of 80-90%.

39
After CRT-D DATELA (mm)LVEF (%)SPAP (mmHg) 19-1-2011536340 24-8-2011566170 23-9-2011495970 5-12-2011 (B)573075 21-12-11- MI 3/4 !4095 14-5-2012- MI 1/46260
LVEF (%)SPAP (mmHg) (B) MI 3/4 ! MI 1/46260")
40
After CRT-D

42
What about the future? Embolization Heart failure Atrial and ventricular arrhythmias.

43
Best strategy to treat AF in inherited arrhythmia disorders? Medical: Disease specific therapies and disease specific pro-arrhythmic drugs. THE MIRROR-IMAGE PATHOPHYSIOLOGY Electrical: Pacing for SSS. Ablation: RF ablation versus cryoablation. Surgical: Hybrid therapy for persistent AF.

44
ISSUES ABOUT ANTICOAGULATION IN INHERITED ARRHYTHMIA DISORDERS. IADs not diagnosed as the cause of AF. Incidence and prevalence of AF in IADs unclear. Indications for anticoagulation in IADs unclear. Role of CHADS2 and CHAD2DS2-VASC scores?

45
With AF, the younger you are the greater the risk? CHADS2y/risky to 100% 0250 1333 2425 3616 4911 5129 6186

46
Conclusions Because of the low embolization score NOACs are not reimbursed for patients with IADs in spite of the high cumulative life-long risk. Studies to understand and guidelines on how to manage AF in IADs are urgently required. In young individuals with AF, and in those with a structurally normal heart, IADs have to be excluded as the cause of AF.

Similar presentations













 -Pt acutely unwell with palpitations -Pt with haemodyanically unstable acute onset AF -2 nd /3 rd heart block -Exercise.>")







