Download presentation
Presentation is loading. Please wait.

1
What’s New in Resuscitation
VOMA VOMA What’s New in Resuscitation Greg Christiansen DO, MEd, FACOEP VCU Department of Emergency Medicine

2
Disclosure No Industry or Third Party Affiliation No Conflict of Interest Credits: Dr. Kevin Ward Dr. Joe Ornato VOMA VOMA

3
Goals Recognize processes to follow in an emergent cardiac arrest as part of a resuscitation effort Be familiar with acute resuscitation concepts guiding acute cardiac care

4
Perceptions and Reality
Television drama demonstrate 75 % survival rate Correlates with public perception of CPR success Adams found 81% of elderly admitted to a hospital believed there was a > 50% chance of their own survival if they had CPR Derrick Adams How mispercetpions among elderly pt regarding survival outcomes…JAOA 106 July 2006 Diem Cardiopulmonary resuscitation on TV: miracles & misinformation NEJM 1996:

5
Myths & Reality Successful field resuscitation rates 2-5%
Long held belief… out of hospital cardiac arrest efforts are futile

6
Some Myths Die Hard

7
Flatliners ..\..\..\Image File\recorded video\video\resuscitation\Flatlinev2.mpg The future is changing

8
Question: Brain Heart Kidney Intestines
Which One of these Organs are Primarily Perfused During Diastole? Brain Heart Kidney Intestines

9
Question: Brain Heart Kidney Intestines
Which One of these Organs are Primarily Perfused During Diastole? Brain Heart Kidney Intestines

10
ABP: 120/20, CVP: 20 ABP: 160/10, CVP: 30 ABP: 60/30, CVP: 0
Which Patient has the Highest Chance of ROSC During CPR? ABP: 120/20, CVP: 20 ABP: 160/10, CVP: 30 ABP: 60/30, CVP: 0

11
CPP = end diastolic atrial pressure – Right atrial pressure ( CVP)
Which Patient has the Highest Chance of ROSC During CPR? ABP: 120/20, CVP: 20 ABP: 160/10, CVP: 30 ABP: 60/30, CVP: 0 CPP = end diastolic atrial pressure – Right atrial pressure ( CVP) 30 – 0 = 30 CCP
 30 – 0 = 30 CCP.")
12
PetCO2: 6 mmHg: ABP 100/30 PetCO2: 9 mmHg: ABP 120/20
Which Patient has Highest Likelihood of ROSC During CPR? PetCO2: 6 mmHg: ABP 100/30 PetCO2: 9 mmHg: ABP 120/20 PetCO2: 20 mmHg: ABP 70/20

13
CPP > 15 tend to have higher ROSC
Which Patient has Highest Likelihood of ROSC During CPR? PetCO2: 6 mmHg: ABP 100/30 PetCO2: 9 mmHg: ABP 120/20 PetCO2: 20 mmHg: ABP 70/20 CPP > 15 tend to have higher ROSC

14
Increase Cardiac output Decrease Cardiac Output
What effect will Epinephrine or Vasopressin have during CPR? Lower PetCO2 levels Increase PetCO2 levels Increase Cardiac output Decrease Cardiac Output

15
Increase Cardiac output Decrease Cardiac Output
What effect will Epinephrine or Vasopressin have during CPR? Lower PetCO2 levels Increase PetCO2 levels Increase Cardiac output Decrease Cardiac Output Vasopressors ↑ after load, ↓CO↓CPP ↓ETCO2

16
Rosamond et al. , Heart Disease & Stroke Statistics, 2008 Update
Rosamond et al., Heart Disease & Stroke Statistics, 2008 Update. Circulation 2008; 117:e1-e122

17
Case: MR Ve Thach – 46 yo male collapsed on the tread mill Full arrest CPR ALS medication 10 minute down time

18
My First Case Fluid resuscitation ROSC Coma Decorticate Posturing Sent to CT Instituted therapeutic hypothermia

19
Were not making vegetables

20
Lessons learned What it is & why it works … sometimes

21
Cardiac Arrest Final common pathway: Everyone has it once
A symptom or finding of a disease process Myocardial ischemia, profound hypoxia, conduction defects, toxicologic, hemorrhage, etc The ultimate state of shock: Global ischemia Neurologic outcomes better than commonly believed

22
Goals (when appropriate)
Return of Spontaneous Circulation (ROSC) and reversal of underlying causes. What is the best therapy for the brain during CPR? Restart the Heart
 and reversal of underlying causes. What is the best therapy for the brain during CPR Restart the Heart.")
23
Methods Electrical Therapy Pharmacological Therapy
Mechanical perfusion

24
Ischemia: The Problem ATP ATP ATP Failure OER : Oxygen extraction
VO2: oxygen consumption SVO2 mix venous saturation ATP Failure

25
Importance of Myocardial ATP
Myocardial Cell 100% ATP Myocardial Cell <10% ATP Myocardial Cell 30-40% ATP

26
Cardiac Image No CPR Courtesy of Dr. Stig Steen
University Hospital Lund, Sweden

27
Cardiac Resus image with CPR

28
Coronary Perfusion Pressure (CPP) Key to Successful Resuscitation
Aod RAd CPP = Aod - RAd

29
Effect of Chest Compression Pauses on Coronary Perfusion Pressure
Aorta RA CPP

30
The Higher the CPP the Better

31
Mechanism for Cardiac Compression
Direct Compression of Chambers Functional Aortic Valve Trend for higher CPP

32
Thoracic Pump Mechanism
Global changes in intrathoracic pressure Heart is passive conduit Harder to achieve CPP Maybe better CePP Beware of Chest tubes

33
Not mutually exclusive Body habitus dependent?
Which Pump? Not mutually exclusive Body habitus dependent? Both markedly deteriorate over time as valves become less functional.

34
Palpating Pulses to Monitor CPR Effectiveness …..
Driving Blindly: Rule #1: Palpating Pulses to Monitor CPR Effectiveness ….. Is for Those Who Don’t Know What to Do.

35
Vasopressors: Epinephrine vs. Vasopressin
How to Improve CPP? Pharmacologically Vasopressors: Epinephrine vs. Vasopressin Mechanically Type of CPR: Regular, new and improved, delux

36
Effects of Epinephrine

37
Summary Many critical components to Successful Resuscitation (Neurological Recovery) Limiting Total Arrest time is Key!!! Obtain ROSC ASAP (5-10 minutes) After ROSC….Real work begins Similar to Trauma Care…Should be one with Cardiology/Pulmonary Critical Care
 After ROSC….Real work begins. Similar to Trauma Care…Should be one with Cardiology/Pulmonary Critical Care.")
38
Improving Blood Flow during Resuscitation

39
Quality of Chest Compressions in OOH-CA Wik et al
Quality of Chest Compressions in OOH-CA Wik et al. JAMA 2005: 293: 176 adult patients Sweden, Norway, England ROSC 35% These data come from new technology that allows measurement of the quality of CPR. Even with allowance for advanced procedures, analysis, etc…, the NFR was 42%. Elevated No Flow Ratios may be responsible for the dismal outcomes from cardiac arrest and the failure for multiple promising new therapies to demonstrate efficacy in human trials.

40
Minimally Interrupted CPR Experience
Wisconsin & Arizona: Emphasis on compression quality and quantity New protocol 200 pre shock compression before defibrillation 200 post shock compression. Delays endotracheal intubation and eliminates pulse checks. Bobrow, B.J. et.al., Minimally Interrupted Cardiac Resuscitation by Emergency Medical Services for Out-of-Hospital Cardiac Arrest. JAMA; 2008; 299: pp

41
Minimally Interrupted Cardiopulmonary Resuscitation (MICR) by EMS Bobrow et al. JAMA 2008; 299: Peberdy MA, Ornato JP: JAMA 2008; 299: 62 EMS agencies in Arizona 75% of state population 200 CCs first Rhythm check Single DF 200 CCs post-DF Early epinephrine Delayed intubation

42
CPR Prior to Defibrillation Christenson J et al. AHA ReSS 2007
ROC Epistry N= 7,963 Male 81% Byst CPR 51%

43
Compression Rate vs. ROSC Abella BS. Circulation 2005; 111:428-34
This study demonstrates that in very few of the 30-second time intervals was the optimal chest compression rate observed. Most of the time, the rates were low, probably due to time spent off the chest.

44
Effect of Incomplete Chest Decompression On
Coronary and Cerebral Perfusion Pressures Yannopoulos D et al. Resuscitation 2005;64:363-72 ǂ n=9 instrumented swine 6 minutes untreated VF standard CPR* x 3 min CPR with 75% recoil (residual 1.2 cm sternal end decompression) x 1 min standard CPR* x 1 min defib x 3 ACLS Critical pressure for ROSC (Paradis, JAMA 1990;263:3257-8) % Chest Wall Decompression
 x 1 min standard CPR* x 1 min defib x 3 ACLS. Critical pressure for ROSC. (Paradis, JAMA 1990;263:3257-8) % Chest Wall Decompression.")
45
Median Frequency (VF “Coarseness”)
“Hands-Off” Interval vs. DF Success Eftestol T et al. Circulation 2002; 105:2270-3 156 OOH cardiac arrest 868 DF attempts 0% 20% 40% 60% % ROSC High Medium Low Median Frequency (VF “Coarseness”) 5 10 15 20 "Hands-off Interval" [sec] from Stop CPR to DF shock
 Hands-off Interval [sec] from Stop CPR to DF shock.")
46
CPR Fraction prior to DF Christenson J et al. AHA ReSS 2007
ROC Epistry N= 7,963 Male 81% Byst CPR 51%

47
Improving Blood Flow During Resuscitation
Summary CPR necessary to provide coronary perfusion Must restart the heart for survival Conclusion – focus of the heart! What’s the evidence to support this focus?

48
Therapeutic hypothermia during or immediately after resuscitation

49
Today 500 of 5,000 hospitals use therapeutic hypothermia
Capturing on 20% of all eligible patients If the patient can’t walk out of the hospital then… A hospital bed is a parked taxi with the meter running - Groucho Marx

50
BRAIN INJURY is the most common cause of death after initial resuscitation from sudden cardiac arrest HIPPA

51
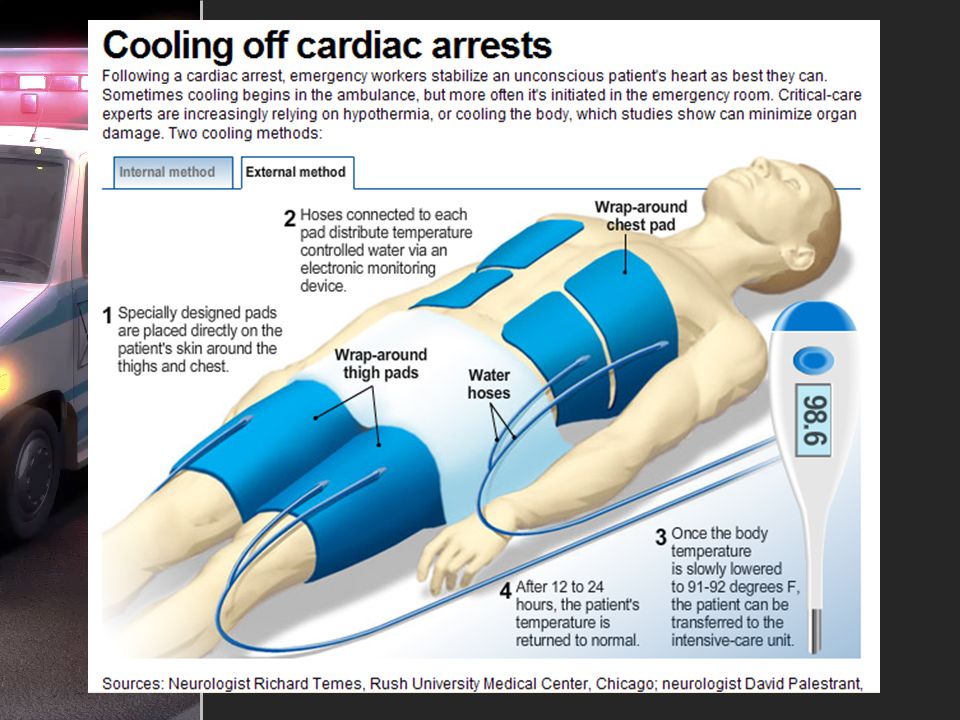
Contemporary Headlines
Cooling off cardiac arrests When heart stops, hypothermia helps- Sunday Gazette Charleston WV More Hospitals Offering Therapeutic Hypothermia For Comatose Survivors Of Cardiac Arrest.

52
Public blogs say…

53
Public Commentary

54
Metabolic Chain of Events in Cardiac Arrest
Cell Damage No Blood Flow Cerebral Ischemia CPR / Pulse Free Radicals O2 Reperfusion Cell Death and Cerebral injury 54

55
Induced Hypothermia (32-34º C) The Hypothermia after Cardiac Arrest Study Group N Engl J Med 2002; 346 : 7 European EDs 275 VT/VF pts with ROSC Cooled to 32-34º C using an external cooling device +/- ice packs for 24 h Sedated with midazolam and fentanyl, paralysed with pancuronium 6 month follow-up

56
Induced Hypothermia (33º C) Bernard SA et al
Induced Hypothermia (33º C) Bernard SA et al. N Engl J Med 2002; 346 : Australian study 73 OOH-CA pts with ROSC Cooled to 33º C for 12 h
 Bernard SA et al. N Engl J Med 2002; 346 : Australian study. 73 OOH-CA pts with ROSC. Cooled to 33º C for 12 h.")
59
Cooling Techniques

60
Cooled IV Fluid Infusion

61
Pilot Randomized Trial of Prehospital Induction of Hypothermia in OOH-CA with Rapid Infusion of 4ºC Saline Kim et. al. Circ 2007;115: p= .15 p= .13

62
Specialized Post-Resuscitation Centers

63
Resuscitation Care ROSC 63

64
In-Hospital Factors Associated with Improved Outcome from OOH-CA Langhelle A et al. Resuscitation 2003; 56:247-63 4 regions in Norway

65
Implementation of a Standardized Treatment Protocol for Post Resuscitation Care After OOH-CA Sunde K, et al. Resuscitation, 2007 Before and after study on the effects of a comprehensive post resuscitation treatment protocol on neurologically intact survival to hospital discharge Early reperfusion with PCI Therapeutic hypothermia Standardized treatment protocol for glucose control, hemodynamic and ventilator management, seizure treatment Before group: 26% neuro intact survival After group: % neuro intact survival

66
Richmond Strategic Approach to Resuscitation
Pre-arrival (phone CPR) Autopulse™ CPR (≥2 min) before DF 1 medic makes 1 attempt at ET, then use King LTS™ device 1 medic makes 1 attempt at IV, then insert EZ-IO™ device Vasopressin 40u IV alternating with epinephrine 1 mg IV every 5 min 2 L NS at 4º C IV started during CPR All pts brought to single center
 Autopulse™ CPR (≥2 min) before DF. 1 medic makes 1 attempt at ET, then use King LTS™ device. 1 medic makes 1 attempt at IV, then insert EZ-IO™ device. Vasopressin 40u IV alternating with epinephrine 1 mg IV every 5 min. 2 L NS at 4º C IV started during CPR. All pts brought to single center.")
67
RAA Field Hypothermia Induction Indications
Initial VF or Witnessed arrest w/ PEA or asystole Initial core temperature >34 ºC No contraindications to cooling (e.g., terminal illness, DNAR, obvious signs of biological death)
")
68
RAA Field Hypothermia Induction Protocol Summary
EMS Supervisor carries iced saline Expose patient; icepacks to neck, axilla, groin 4 ºC saline 30 ml/kg (up to 2 L) IV with pressure bag 18F orogastric tube Novotemp™ orogastric probe
 IV with pressure bag 18F orogastric tube Novotemp™ orogastric probe")
69
Significant improvement with protocol change
Citywide ROSC & Survival to Discharge Richmond, VA: vs N= 1,233 p= .0001 Significant improvement with protocol change p= .002

70
Richmond Ambulance Field Hypothermia Induction
Tdelta= -1.9 [95% CI -4.3, 0.4] ROSC= 86%

71
Advanced Resuscitation Cooling Therapeutics Intensive Care

72
ARCTIC 24/7 post-resuscitation team that can initiate endovascular cooling w/in 30 min of ED arrival Trained, dedicated support team of ED and CCU physicians and nurses ED team responsible for primary patient care CCU/cath team responsible for cooling Catheters placed by interventional cardiologist Alert initiated by EMS, activated by EM attending physician

73
Relative Contraindications to Continued Cooling After ED Arrival
Persistent hypotension MAP <60 despite IVF and stable doses of vasopressors Known coagulopathy or thrombocytopenia Active bleeding Existing DNAR status Known end-stage terminal illness pre-arrest Severe neurological dysfunction pre-arrest

74
Goal-Directed Protocols
Tight glucose control Cortisol screening for relative adrenal insufficiency Immediate neurology and critical care specialty consultation Continuous EEG monitoring with aggressive seizure management

75
Continuous EEG Monitoring Rossetti AO et al. Neurology 2007; 69:255-60
EEG monitoring in 166 adult comatose cardiac arrest pts 59% therapeutic hypothermia 33% survival Status epilepticus associated with poor survival

76
Consistent MD Direction
Attending physicians experienced in post-resuscitation hypothermia care involved in every case 72h moratorium on offering withdrawal of life support Detailed neuropsychiatric testing

77
ARTIC Program Survival 2008

78
ARCTIC Cases 42 F arrest at church 50 M lawyer arrest at YMCA
28 M Marfan’s arrest at home 55 M prisoner arrest at City jail 16 F MVP arrest at cheerleading

79
Summary Reviewed the latest information on what occurs physiologically during cardiac arrest Discussed ways to improve blood flow during resuscitation Described techniques to initiate therapeutic hypothermia during or immediately after resuscitation Discussed the importance of specialized post-resuscitation centers

80
Questions Thank you to Dr. Ornato & Dr. Ward for providing the slides & data support for this lecture

Similar presentations











>")



>")




