Download presentation
Presentation is loading. Please wait.

1
به نام خدا

2
Immunonutrition: modulate the immune system facilitate wound healing
reduce oxidative stress

3
l-glutamine l-arginine omega-3 fatty antioxidants
contain certain compounds: l-glutamine l-arginine omega-3 fatty antioxidants

4
ASPEN/ESPEN: Immune-modulating enteral formulations (supplemented with agents such as arginine, glutamine, nucleic acid, ω-3 fatty acids, and antioxidants) should be used for the appropriate patient population (major elective surgery, trauma, burns, head and neck cancer, and critically ill patients on mechanical ventilation), with caution in patients with severe sepsis.
 should be used for the appropriate. patient population (major elective surgery, trauma, burns, head and. neck cancer, and critically ill patients on mechanical ventilation), with caution in patients with severe sepsis.")
5
To receive optimal therapeutic benefit from the immune-modulating
formulations, at least 50%–65% of goal energy requirements should be delivered daily.

6
L-ARGININE plays fundamental roles in protein metabolism
polyamine synthesis critical substrate for nitricoxide (NO) production
 production.")
7
stimulates the release ; growth hormone
insulin growth factor and insulin all of which may stimulate protein synthesis and promote wound healing. The enzyme, l-arginase, metabolizes l-arginine to l-ornithine, an amino acid implicated in wound healing.

8
. Normal l-arginine intake is 3 to 5 g/d.
Guidelines for arginine supplementation can be summarized as follows: . Normal l-arginine intake is 3 to 5 g/d. Higher than normal (supraphysiologic) l-arginine supplementation is necessary
 l-arginine. supplementation is necessary.")
9
Dietary supplementation with l-arginine alone should not be used, as only diets
Immunonutrition incorporating supraphysiologic quantities Of l-arginine ideally should be started preoperatively as an oral dietary supplement and continued in the postoperative

10
A clear benefit of l-arginine-containing immunonutrition has
not been observed in medical patients, particularly those with sepsis. All elective surgical patient populations, including patients undergoing operations for head and neck cancer and patients undergoing cardiac or GI surgery, appear to benefit from the useof immunonutrition formulas containing l-arginine.

11
Risk vs Benefit Arginine

12
OMEGA-3 FATTY ACIDS incorporated into phospholipids and thereby influence the structure and function of cellular membranes. as substrates for the enzymes cyclooxygenase, lipoxygenase, and cytochrome P450 oxidase increasing the quantity of omega-3 fatty acids (found in fish oils) in the diet reduces platelet aggregation, slows blood clotting, and limits the production of proinflammatory cytokines. .
 in the diet reduces platelet aggregation, slows blood clotting, and limits the production of proinflammatory cytokines. .")
13
administration of dietary lipids rich in omega-3 fatty acids can modify the lipid profile and favorably affect clinical outcome a mong critically ill patients with ARDS

14
L-GLUTAMINE: The amino acid, l-glutamine, plays a central role in nitrogen transport within the body. used as a fuel by rapidly dividing cells, particularly lymphocytes and gut epithelial cells. substrate for synthesis of the important endogenous antioxidant translocation of enteric bacteria and endotoxins is reduced and infective complications less frequent.

15
l-Glutamine unfortunately is unstable in aqueous solutions.
To overcome this problem, l-glutamine is added to TPN solutions as adipeptide (l-alanyl-l-glutamine). In patients receiving EN, l-glutamine powder can be dissolved into the nutrition formulation.
. In patients receiving EN, l-glutamine powder can be dissolved into the nutrition formulation.")
16
Glutamine (enteral): All: The addition of enteral glutamine to an EN regimen (not already containing supplemental glutamine) should be considered in thermally injured, trauma, and mixed ICU patients.
 should be considered in. thermally injured, trauma, and mixed ICU patients.")
17
is an essential component of the most important
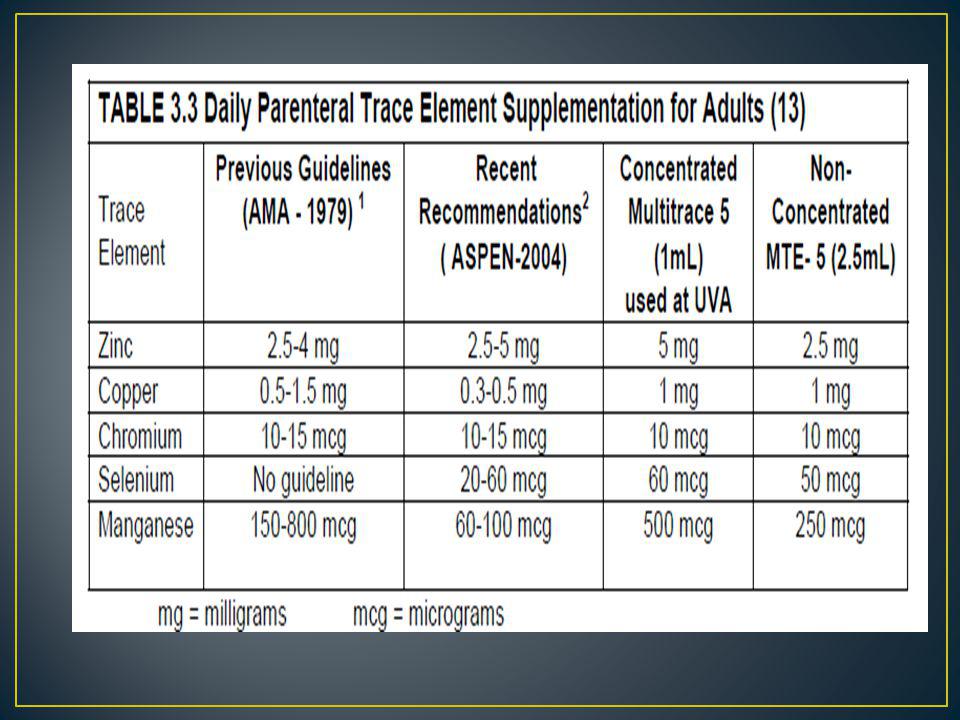
Selenium; is an essential component of the most important extra- and intra-cellular antioxidant enzyme family, the glutathione peroxidases (GPX). doses of 750–1000 mcg/day should probably not be exceeded in the critically ill, and aministration of supraphysiological ddoses should perhaps be administratlimited to 2 weeks. 20-60 mcg
. doses of 750–1000 mcg/day should probably not be. exceeded in the critically ill, and aministration of supraphysiological. ddoses should perhaps be administratlimited to 2 weeks mcg.")
18
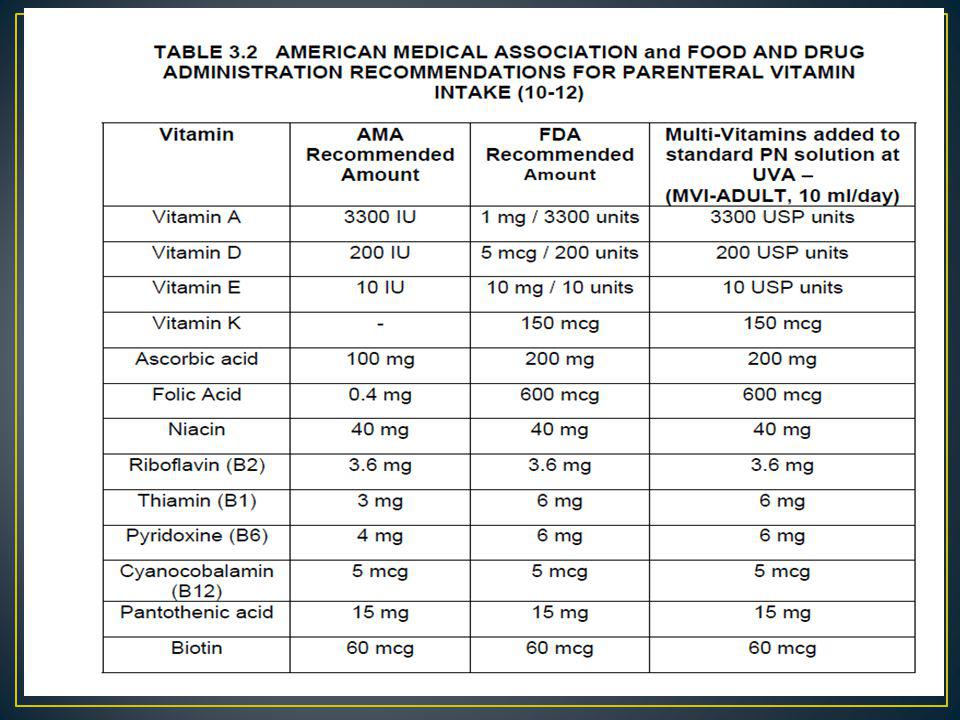
Recommended Daily Intake
Ascorbic acid (C) 200 mg Vitamin A IU Vitamin D mg Vitamin E IU
 200 mg. Vitamin A 3300 IU. Vitamin D 5 mg. Vitamin E 10 IU.")
19
Which Nutrient for Which Population?
Elective Surgery Critically Ill General Septic Trauma Burns Acute Lung Injury Arginine Benefit No benefit Harm(?) (Possible benefit) Glutamine Possible Benefit PN Beneficial Recom-mend … EN Possibly Beneficial: Consider Omega 3 FFA Anti-oxidants Canadian Clinical Practice Guidelines
 (Possible benefit) Glutamine. Possible Benefit. PN Beneficial. Recom-mend. … EN Possibly Beneficial: Consider. Omega 3 FFA. Anti-oxidants. Canadian Clinical Practice Guidelines.")
20
Current nutritional status Current metabolic and disease states
ADULT : NUTRITIONAL REQUIREMENTS The nutritional requirements of each patient will depend upon a number of factors including: Age Activity level Current nutritional status Current metabolic and disease states

21
1)Calorie Requirements:
Metabolic cart predictive equations

22
If available, indirect calorimetry can be used to measure energy expenditure using gas exchange
When indirect calorimetry is not possible, there are many possible predictive equations whichever method (indirect calorimetry or predictive equation) is used, the optimal energy provision for hospitalized patients has yet to be determined
 is used, the optimal energy provision for hospitalized patients has yet to be determined.")
23
Metabolic cart (28, 29): Indirect calorimetry using a “metabolic cart” measures actual energy expenditure by collecting, measuring and analyzing the oxygen consumed (VO2) and the carbon dioxide (VCO2) expired. From these measurements the respiratory quotient (RQ) is calculated
 and the carbon dioxide (VCO2) expired. From these measurements the respiratory quotient (RQ) is calculated.")
24
RQ = VOz/VCOz b. REE = (3.94 [VOz] [VCOz]) (2.17 [UUN])
![RQ = VOz/VCOz b. REE = (3.94 [VOz] [VCOz]) (2.17 [UUN])](http://slideplayer.com/slide/1624177/6/images/24/RQ+%3D+VOz%2FVCOz+b.+REE+%3D+%283.94+%5BVOz%5D+%5BVCOz%5D%29+%282.17+%5BUUN%5D%29.jpg "RQ = VOz/VCOz b. REE = (3.94 [VOz] [VCOz]) (2.17 [UUN])")
25
Note: Patient has to be intubated for the test to be performed FIO2<60%, no air leak chest tube leak.

26
PREDICTIVE EQUATIONS Harris-Benedict Miflin St. Jeor (MSJ)
")
27
Use of Indirect Calorimetry vs. Predictive Equations
PCG: 2013 Recommendation: There are insufficient data to make a recommendation on the use of indirect calorimetry vs. predictive equations for determining energy needs for nutrition or to guide when nutrition is to be supplemented in critically ill patients.

28
Conclusions: The use of indirect calorimetry compared to predictive equations to meet enteral nutrition needs has no effect on mortality.

29
(A.S.P.E.N) Predictive equations should be used with
caution, as they provide a less accurate measure of energy requirements than indirect calorimetry in the individual patient.

30
Calorie Requirements:
CALORIE REQUIREMENTS IN MOST HOSPITALIZED PATIENTS

31
Resting energy expenditure (REE)—the energy expenditure while resting in the supine position with eyes open About 10% greater than BEE

32
Sleeping energy expenditure (SEE)
It is usually 10% to 15% lower than REE Activity energy expenditure (AEE) During maximum exercise it can be 6- to 10-fold greater than the BEE.
 During maximum exercise it can be 6- to 10-fold greater than the BEE.")
33
Total energy expenditure (TEE)
the sum of energy expended during periods of sleep, resting, and activity.

34
eREE = eBEE • stress factor eTEE = eREE • activity factor
estimated resting energy expenditure; eREE = eBEE • stress factor eTEE = eREE • activity factor estimated total energy expenditure

35
Stress Factors COPD: 10%-15% Major surgery: 15%-25% Infection: 20%
Long bone fracture: 20%-35% Malnutrition: Subtract 10%-15% Burns: Up to 120% depending on extent Sepsis: 30%-55% Major trauma: 20%-35% COPD: 10%-15% Sedated mechanically ventilated patients: Subtract 10%-15%.

36
Activity Factors Sedated mechanically ventilated patients: 0-5%
Bedridden, spontaneously breathing nonsedated patients: 10%-15% Sitting in chair: 15%-20% Ambulating patients: 20%-25%

37
Daily Caloric Requirements
Using Measured or Estimated REE Using Body Weight Sedated mechanically ventilated patients • REE 20-24 kcal/kg Unsedated mechanically ventilated patients 1.2 • REE 22-24 kcal/kg Spontaneously breathing critically ill patients • REE 24-26 kcal/kg Spontaneously breathing ward patients (maintenance) 1.3 • REE Spontaneously breathing ward patients (repletion) • REE 25-30 kcal/kg
 1.3 • REE. Spontaneously breathing ward patients (repletion) • REE kcal/kg.")
38
HBE or MSJ x Injury factor
University of Kentucky Medical Center KCAL/Kg HBE or MSJ x Injury factor

39
University of Kentucky Medical Center
KCAL/Kg Wound Healing: kcal/kg, increase to kcal/kg if the pt is underweight or losing weight. Sepsis and Infection: kcal/kg Trauma: kcal/kg Acute Spinal Cord Injury (SCI) 23kcal/kg or HBE w/o stress factor Chronic SCI: 20-23kcal/kg depending on activity Stroke: 19-20kcal/kg or (HBE x ) COPD: kcal/kg
 23kcal/kg or HBE w/o stress factor. Chronic SCI: 20-23kcal/kg depending on activity. Stroke: 19-20kcal/kg or (HBE x ) COPD: kcal/kg.")
40
ARF: kcal/kg Hepatitis: kcal/kg if well-nourished 30kcal/kg), kcal/kg if malnourished Cirrhosis without encephalopathy: kcal/kg Cirrhosis with encephalopathy: 35 kcal/kg Severe Acute Pancreatitis: 35 kcal/kg

41
Organ Transplant: 30-35 kcal/kg
Cancer: Sedentary/normal wt = kcal. Hypermetabolic, need to gain weight, or anabolic = kcal/kg. Hypermetabolic, malabsorption, severe stress: > 35 kcal/kg . Obese = kcal/kg

42
Major Non-elective HBE x 1.3 - 1.5 Minor Elective HBE x 1.2
Estimated Calorie Needs: HBE or MSJ x Injury factor Major Elective HBE x Major Non-elective HBE x Minor Elective HBE x Minor Non-elective HBE x Infection w/temp HBE x

43
Traumatic Brain Injury (CHI) HBE x 1.4
Multiple trauma & CHI HBE x 1.4 – 1.6 Pentobarbital coma HBE x 1.0 – 1.2 Stroke and SAH HBE x Pneumonia (or ARDS) HBE x Neuromuscular Blockade HBE x 1
 HBE x Neuromuscular Blockade HBE x 1.")
44
Energy: ASPEN Use 25-30kcal/kg, or predictive equations, or indirect calorimetry. Consider hypocaloric feeding in critically ill obese (BMI >30kg/m2), e.g % of target energy requirements, or 11-14kcal/kg actual body weight, or 22-25kcal/kg ideal body weight.
, e.g % of target energy requirements, or 11-14kcal/kg actual body weight, or 22-25kcal/kg ideal body weight.")
45
ESPEN : 20-25kcal/kg in acute phase of critical illness.
25-30kcal/kg in recovery phase.

46
Carbohydrates provide 4 kcal/g (IV dextrose = 3.4 kcal/g) with an RQ of 1.0. Between 40% and 60% of total caloric needs (or 70% of nonprotein calories)
")
47
Minimum 2g/kg ESPEN 2009 Maximal glucose oxidation rate is 4-7 mg/kg/minute/24hours. Ideally keep to ≤5mg/kg/minute/24hours

48
Protein Normal patient = 0.8 to 1.0 g/kg
2. Postsurgical, mild trauma = 1.25 to 1.5 g/kg 3. Severe trauma, sepsis, organ failure = 1.5 to 2.0 g/kg 4. Burn (>20%) or severe head injury ~2.0 g/kg
 or severe head injury ~2.0 g/kg.")
49
g protein/kg ESPEN g protein/kg if BMI<30kg/m ASPEN 2g/kg ideal weight if BMI 30-40kg/m2. 2.5g/kg ideal weight if BMI >40kg/m2.

50
caloric requirements (or 30% of nonprotein calories)
Fat provides 9 kcal/g with an RQ of 0.7. Between 20% and 30% of total caloric requirements (or 30% of nonprotein calories) g/kg ESPEN
 g/kg. ESPEN.")
51
ENTERAL NUTRITION

52
1)Oral intake is contraindicated
INDICATIONS FOR INITIATION OF ENTERAL NUTRITION 1)Oral intake is contraindicated Examples Dysphagia, mechanical ventilation, mandibular fractures, head & neck surgery, neurological impairment, demyelinating diseases such as amyotrophic lateral sclerosis, muscular dystrophy, etc.
Oral intake is contraindicated. Examples. Dysphagia, mechanical ventilation, mandibular fractures, head & neck surgery, neurological impairment, demyelinating diseases such as amyotrophic lateral sclerosis, muscular dystrophy, etc.")
53
2)Inability to meet markedly increased nutritional needs with oral intake
Examples Burns, trauma, radiation therapy, chemotherapy, sepsis/infection, closed head injury

54
3)Inability to meet basic nutritional needs with oral intake alone
Examples Anorexia, cancer, head and neck tumors

55
4)Need to bypass part of the GI tract to allow enteral nutrition
Examples Pancreatitis, gastric outlet obstruction, esophageal cancer, gastroparesis

56
5)The need for supplemental nutrition due to decreased absorption
Examples Short bowel syndrome, inflammatory bowel disease, fat malabsorption or other malabsorptive syndromes such as cystic fibrosis

57
Benefits of Enteral Nutrition (compared with Parenteral Nutrition)
Stimulates immune barrier function Physiologic presentation of nutrients Maintains gut mucosa Attenuates hypermetabolic response Simplifies fluid/electrolyte management More “complete” nutrition than parenteral nutrition o iron, fiber, glutamine, etc. are not provided. Less infectious complications (and costs associated with these complications) Stimulates return of bowel function Less expensive
 Stimulates return of bowel function. Less expensive.")
58
Delivery Method: Bolus feeding Continuous or cyclic:
Intermittent feeding Bolus feeding

59
Continuous or cyclic 18-24 h 25cc/h 8-24h double cc/h

60
Intermittent feeding usually 240-480ml, over a 45-60 minute
period 5-8 times per day. Preferred by ambulatory patients. Disadvantage includes: poor tolerance since a larger feeding volume is administered over a short time.

61
Bolus feeding Bolus feeding is discouraged in the ICU.
rapid infusion via syringe through a gastrostomy tube may result in nausea, diarrhea, distention, cramps, or aspiration cc 3-5h 5-10min

62
(glucose and fructose).
Carbohydrate (CHO): Concentration & form of CHO constitute major differences between formulas Forms of CHO include: Simple sugars and monosaccharides (glucose and fructose). Disaccharides (sucrose, lactose, and maltose) require enzymatic conversion to monosaccharides in the intestinalbrush border prior to absorption.
: Concentration & form of CHO constitute major differences between formulas. Forms of CHO include: Simple sugars and monosaccharides. (glucose and fructose). Disaccharides. (sucrose, lactose, and maltose) require enzymatic conversion to monosaccharides in the intestinalbrush border prior to absorption.")
63
Polysaccharides and oligosaccharides
, produced from hydrolysis of starch, result in glucose polymers of intermediate chain lengths. Starch hydrolysis increases the solubility and osmolality of the product

64
Intact protein, found in whole foods, requires complete digestion.
Three major categories are classified by degree of digestion required: Intact protein, found in whole foods, requires complete digestion. Crystalline amino acids – theoretically require minimal digestion. The small particle size increases the osmolality

65
short bowel and Crohn's disease and pancreatic insufficiency.
Hydrolyzed protein –enzymatically hydrolyzed to smaller peptide fragments and free amino acids, partially hydrolyzed protein requires digestion while di and tri-peptides are absorbed directly. Useful in conditions such as: short bowel and Crohn's disease and pancreatic insufficiency.

66
Fat: Increases the caloric density but does not contribute to the osmolality. Most formulas contain long chain triglycerides (LCT) with variable amounts of medium-chain triglycerides (MCT) and mono and diglycerides.
 with variable amounts of medium-chain triglycerides (MCT) and mono and diglycerides.")
67
MCT are transported via the portal system directly
into the blood stream they are oxidized to ketones and carbon dioxide. MCT does not require emulsification for absorption their use is indicated with CF, liver disease, pancreatitis, and other disorders where fat absorption may be impaired.

68
All: EN should be started within the first 24–48 hours following
Timing of enteral nutrition All: EN should be started within the first 24–48 hours following admission

69
PCG 2013 Recommendation: Based on 16 studies, we recommend early enteral nutrition (within hours following admission to ICU) in critically ill patients.
 in critically ill patients.")
70
Conclusions: 1) Early enteral nutrition, when compared to delayed nutrient intake is associated with a trend towards a reduction in mortality in critically ill patients. 2) Early enteral nutrition, when compared to delayed nutrient intake is associated with a significant reduction in infectious complications
 Early enteral nutrition, when compared to delayed nutrient intake is associated with a trend towards a reduction in mortality in critically ill patients. 2) Early enteral nutrition, when compared to delayed nutrient intake is associated with a significant reduction in infectious complications.")
71
3) Early enteral nutrition, when compared to delayed nutrient intake has no effect on ICU or hospital length of stay. 4) Early enteral nutrition, when compared to delayed nutrient intake improves nutritional intake
 Early enteral nutrition, when compared to delayed nutrient intake improves nutritional intake.")
72
PCG Achieving Target Dose of Enteral Nutrition
There were no new randomized controlled trials since the 2009 update and hence there are no changes to the following summary of evidence.

73
ASPEN: The feedings should be advanced toward the patient’s goal
Dosage of enteral feeding ASPEN: The feedings should be advanced toward the patient’s goal over the next 48–72 hours Efforts to provide > 50%–65% of goal energy should be made in order to achieve the clinical benefit of EN over the first week of hospitalisation.

74
No general amount can be recommended as EN therapy has
ESPEN: No general amount can be recommended as EN therapy has to be adjusted according to the progression/course of the disease and to gut tolerance

75
ASPEN/CCPG: If unable to meet energy requirements (100%
of target goal energy) after 7–10 days by the enteral route alone, consider initiating supplemental parenteral nutrition ESPEN: All patients who do not meet their nutritional needs after 2 days should receive supplemental PN.
 after 7–10 days by the enteral route. alone, consider initiating supplemental parenteral nutrition. ESPEN: All patients who do not meet their nutritional needs after 2 days should receive supplemental PN.")
76
Haemodynamically unstable patients
ASPEN: In the setting of haemodynamic compromise : patients requiring significant haemodynamic support including high dose catecholamine agents, alone in combination with large volume fluid or blood product resuscitation to maintain cellular perfusion), EN should be withheld until the patient is fully resuscitated and/or stable.
, EN should be withheld until the patient is fully resuscitated and/or stable.")
77
Immune-modulating enteral formulations
ASPEN/ESPEN: Immune-modulating enteral formulations supplementaed with agents such s arginine, glutamine, nucleic acid, ω-3 fatty acids, and antioxidants) should be used for the appropriate patient population (major elective surgery, trauma, burns, head and neck cancer, and critically ill patients on mechanical ventilation), with caution in patients with severe sepsis
 should be used for the appropriate. patient population (major elective surgery, trauma, burns, head and neck cancer, and critically ill. patients on mechanical ventilation), with caution in patients with severe sepsis.")
78
Complications of overfeeding include (but not limited to):
. Hyperglycemia . Lipogenesis Fluid and fat gain rather than lean body mass gain Fatty liver Immunosuppression (with excessive lipid and linoleic acid intake) Increased minute ventilation (VE) Excessive CO2 production impairing pulmonary status/vent wean
 Increased minute ventilation (VE) Excessive CO2 production impairing pulmonary status/vent wean.")
79
DRUG NUTRIENT INTERACTIONS WITH ENTERAL PRODUCTS
Only administer sucralfate (CarafateR), omeprazole, antacids, iron salts, and ketoconazole (NizoralR) into the stomach
, omeprazole, antacids, iron salts, and ketoconazole (NizoralR) into the stomach.")
80
Stop continuous tube feedings for 1 hour before and 1 hour after each phenytoin (DilantinR) dose to maximize the drug absorption.

81
When diarrhea occurs, determine if any medication contains excessive quantities of sorbitol. Examples include: acetaminophen elixir, codeine solution, diazepam solution, LomotilR, furosemide solution, guaifenesin syrup, lithium citrate syrup, metoclopramide syrup, morphine sulfate solution potassium chloride elixirs, and some theophylline solutions.

82
1)Stop the tube feeding prior to administration of meds.
GENERAL GUIDELINES FOR ADMINISTERING MEDICATIONS WITH ENTERAL FEEDINGS: 1)Stop the tube feeding prior to administration of meds. 2)Flush the feeding tube with ml of warm water or appropriate volume before and after giving medication through the tube.
Stop the tube feeding prior to administration of meds. 2)Flush the feeding tube with ml of warm water or appropriate volume before and after giving medication through the tube.")
83
3)If more than one medication is being given at the same time, give each medication separately and flush the tube with 5-15 ml of warm water between medications. 4)Use liquid preparation if possible (if patient does not have diarrhea).
Use liquid preparation if possible (if patient does not have diarrhea).")
84
7)tube feeding when done giving medications.
5)If a tablet form must be used, be sure it is finely crushed and dispersed in warm water. 6)Do not crush enteric-coated, sublingual, or sustained-release tablets, if in doubt check with PharmD. 7)tube feeding when done giving medications.
If a tablet form must be used, be sure it is finely crushed and dispersed in warm water. 6)Do not crush enteric-coated, sublingual, or sustained-release tablets, if in doubt check with. PharmD. 7)tube feeding when done giving medications.")
85
8)tube feeding when done giving medications.
7)Most liquid medications are hypertonic and should be diluted with 30-60ml of water prior to administration 8)tube feeding when done giving medications.
Most liquid medications are hypertonic and should be diluted with 30-60ml of water prior to administration. 8)tube feeding when done giving medications.")
86
Categories of Enteral Formulas

87
Return up to 250 ml gastric residuals to the patient.
Notify physician if feedings held twice in 24 hours.

88
ASPEN -500ml Holding EN for gastric residual volumes
< 500 mL in the absence of other signs of intolerance should be avoided.

89
For high-risk patients or those shown to be
intolerant to gastric feeding, delivery of EN should be switched to continuous infusion. Agents to promote motility such as prokinetic drugs (metoclopramide and erythromycin) or narcotic antagonists (naloxone and alvimopan) should be initiated where clinically feasible.
 or narcotic antagonists (naloxone and alvimopan) should be initiated where clinically. feasible.")
90
Diverting the level of feeding by post-pyloric
tube placement should be considered. Use of chlorhexidine mouthwash twice a day should be considered to reduce risk of ventilator-associated pneumonia.

91
In the ICU setting, evidence of bowel motility
(resolution of clinical ileus) is not required in order toinitiate EN in the ICU.
 is not required in order toinitiate EN in the ICU.")
92
Critically ill patients should be fed
via an enteral access tube placed in the small bowel if at high risk for aspiration or after showing intoleranceto gastric feeding.

93
Parenteral nutrition is usually indicated in the following situations:
1)Documented inability to absorb adequate nutrients via the gastrointestinal tract Massive small-bowel resection / Short bowel syndrome (at least initially) Radiation enteritis Severe diarrhea
Documented inability to absorb adequate nutrients via the gastrointestinal tract. Massive small-bowel resection / Short bowel syndrome (at least initially) Radiation enteritis. Severe diarrhea.")
94
2)Complete bowel obstruction
3)Severe catabolism with or without malnutrition when gastrointestinal tract is not usable within 5-7 days
Severe catabolism with or without malnutrition when gastrointestinal tract is not usable within 5-7 days.")
95
4)Inability to obtain enteral access
5)Inability to provide sufficient nutrients/fluids enterally 6) Pancreatitis in the setting of intolerance to jejunal delivery of nutrients 7) Persistent GI hemorrhage 8) Acute abdomen/ileus
Inability to provide sufficient nutrients/fluids enterally. 6) Pancreatitis in the setting of intolerance to jejunal delivery of nutrients. 7) Persistent GI hemorrhage. 8) Acute abdomen/ileus.")
96
9)High output enterocutaneous fistula and EN access cannot be obtained distal to the site.
10) Trauma requiring repeat surgical procedures / NPO status
 Trauma requiring repeat surgical procedures / NPO status.")
97
Parenteral nutrition may be indicated in the following situations:
Enterocutaneous fistula as above Inflammatory bowel disease unresponsive to medical therapy Hyperemesis gravidarum when nausea and vomiting persist longer than 5 -7 days and enteral nutrition is not possible Partial small bowel obstruction Intensive chemotherapy /

98
Contraindications for Parenteral Nutrition:
1)Functioning gastrointestinal tract 2)Treatment anticipated for less than 5 days in patients without severe malnutrition 3)Inability to obtain venous access 4)A prognosis that does not warrant aggressive nutrition support 5)When the risks of PN are judged to exceed the potential benefits
Functioning gastrointestinal tract. 2)Treatment anticipated for less than 5 days in patients without severe malnutrition. 3)Inability to obtain venous access. 4)A prognosis that does not warrant aggressive nutrition support. 5)When the risks of PN are judged to exceed the potential benefits.")
99
A. MACRONUTRIENTS 2. PROTEIN 3)FAT COMPONENTS OF PARENTERAL NUTRITION:
1)CARBOHYDRATE 2. PROTEIN 3)FAT
CARBOHYDRATE. 2. PROTEIN. 3)FAT.")
100
CARBOHYDRATE Dextrose contains 3.4 kcal/g (CHO is given as a dextrose monohydrate) Requirements: Minimum: 1 mg/kg/minute mg/kg/24hrs Maximum: 5 mg/kg/minute 7200mg/kg/24hrs OR 7 g/kg/day OR 24 dextrose kcal/kg/day.

101
Consequences of excess CHO administration:
Hyperglycemia Glucosuria Synthesis and storage of fat Hepatic steatosis Increased carbon dioxide production impairing pulmonary status/vent wean

102
Requirements: Approximately 16% of protein or amino acids are nitrogen. The goal should be to provide adequate protein to maintain a positive (2 to 4 g) Requirements range from 0.8 g/kg/day to 2.5 g/kg/day. Generally 15 – 20% of the daily caloric intake should come from protein.
 Requirements range from 0.8 g/kg/day to 2.5 g/kg/day. Generally 15 – 20% of the daily caloric intake should come from protein.")
103
PROTEIN Amino acid = 4 kcal/g
Protein calories should be included when calculating total caloric requirements

104
FAT Minimum: To prevent essential fatty acid deficiency (EFAD), 2% to 4% of the total caloric requirement should come from linoleic acid (25 to 100 mg/kg/day) Maximum: Maximal fat dosage should not exceed 60% of calories OR g/kg/day
, 2% to 4% of the total caloric requirement should come from linoleic acid (25 to 100 mg/kg/day) Maximum: Maximal fat dosage should not exceed 60% of calories OR g/kg/day.")
105
Use with caution in patients allergic to eggs.
Lipids should be used with caution in patients with serum triglycerides (TG) > 400mg/dl. Use with caution in patients allergic to eggs.
 > 400mg/dl. Use with caution in patients allergic to eggs.")
106
Lipids are generally administered over a 24 hour period
Guidelines for rate of infusion are < 0.11 g / kg / hr

107
Consequences of excess lipid administration:
Fat overload syndrome with neurologic, cardiac, pulmonary, hepatic and renal dysfunction Thrombocyte adhesiveness Accumulation of lipid in the reticuloendothelial system (RES), leading to RES dysfunction Impaired immune response
, leading to RES dysfunction. Impaired immune response.")
108
MICRONUTRIENTS:

112
PARENTERAL NUTRITION CALCULATIONS:
CUSTOM PN: Step 1 – Determine protein and calorie needs Step 2 – Subtract protein calories (grams protein x 4) from total calories Step 3 – Subtract lipid calories* from remaining calories Step 4 – remaining will be dextrose calories
 from total calories. Step 3 – Subtract lipid calories* from remaining calories. Step 4 – remaining will be dextrose calories.")
113
Minimum flow rates: Dex/50 + g Pro/ = minimum flow rate Central: [(Dextrose kcals X 0.42) + (grams of protein X 10)] ÷ 24 = minimum hourly flow rate. Add 5 ml/hour for MVI, trace elements, etc. Round up to nearest increment of 5. Peripheral: [(Dextrose kcals x 0.15) + grams of protein] ÷ 2.1 = minimum hourly flow rate. Add 5 ml/hour for MVI, trace elements, etc. Round up to nearest increment of 5.
 + (grams of protein X 10)] ÷ 24 = minimum hourly flow rate. Add. 5 ml/hour for MVI, trace elements, etc. Round up to nearest increment of 5. Peripheral: [(Dextrose kcals x 0.15) + grams of protein] ÷ 2.1 = minimum hourly flow rate. Add 5 ml/hour for MVI, trace elements, etc. Round up to nearest increment of 5.")
114
COMPLICATIONS ASSOCIATED WITH PARENTERAL NUTRITION :
Metabolic complications; hyperglycemia is the most common – tight blood glucose control is optimal. Gastrointestinal complications: steatohepatitis, cholestasis Pharmacological complications Manganese toxicity is possible with prolonged use of PN

115
Infection / sepsis Metabolic bone disease

117
Nutritional modifications in disease
A. Diabetes. Low simple sugar. high fiber. and high fat to minimize hyperglycemia. B. Renal failure. High calorie. low protein. and low electrolytes (phosphorus. potassium) to prevent volume overload. hyperammonemia. and electrolyte imbalance. However, in patients on dialysis. protein requirements may actually increase. C. Liver failure. Low protein. high branch chain amino acids to prevent encephalopathy. D. Respiratory failure. High calorie, high fat (low carbohydrate) to prevent CO2 accumulation. E. Pancreatitis. Enteral. postpyloric (nasojejunal) feeding is superior to TPN. F. Other GI diseases. If nonfunctional GI tract, may require TPN. G. Trauma. Consider immune-enhancing diet.
 to prevent volume overload. hyperammonemia. and electrolyte. imbalance. However, in patients on dialysis. protein requirements. may actually increase. C. Liver failure. Low protein. high branch chain amino acids to prevent. encephalopathy. D. Respiratory failure. High calorie, high fat (low carbohydrate) to prevent CO2. accumulation. E. Pancreatitis. Enteral. postpyloric (nasojejunal) feeding is superior to TPN. F. Other GI diseases. If nonfunctional GI tract, may require TPN. G. Trauma. Consider immune-enhancing diet.")
119
Grade 1 ascites Mild ascites only detectable by ultrasound No treatment
Grade 2 ascites Moderate ascites evident by moderate symmetrical distension of abdomen Restriction of sodium intake and diuretics Grade 3 ascites Large or gross ascites with marked abdominal distension Large-volume paracentesis followed by restriction of sodium intake and diuretics (unless patients have refractory ascites)
")
Similar presentations



 to Nutritional Support Alan Shenkin Department of Clinical Chemistry University of Liverpool.>")








, bypassing the oral.>")









