Download presentation
Presentation is loading. Please wait.

2
TO PEE OR NOT TO PEE THAT IS THE QUESTION
URINE TROUBLE TO PEE OR NOT TO PEE THAT IS THE QUESTION Shawn McGlew PA-C, DFAAPA Kennebec County Urology Manchester/Oakland, ME

3
Pre-Test T or F Incontinence is natural part of aging for women not men. Renal ultrasound is the best imaging study for stones. A high sodium diet is the number one reason for stones. Finasteride is a first line treatment for BPH. If CT sees a stone no further imaging is needed. Renal U/S is the most cost effective for hematuria.

4
I can’t pee. I pee to much. It hurts. I’m peeing blood.
Urology Made Easy I can’t pee. I pee to much. It hurts. I’m peeing blood.

6
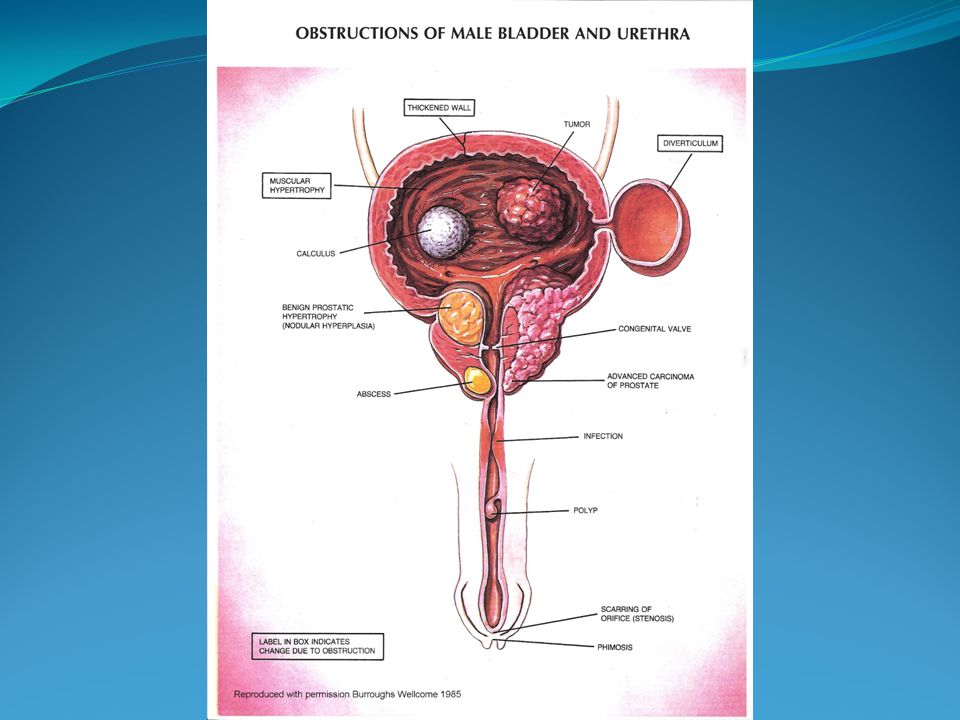
Bladder Outlet Obstruction
Prostate Strictures Poor pelvic floor relaxation Other pathology

8
Bladder Outlet Obstruction
Incomplete bladder emptying Hesitancy Nocturia Urgency with or without leaking Frequency Pelvic pain

9
Bladder Outlet Obstruction
Evaluation: U/A PE / DRE PSA PVR Cysto and/or UDS +\-

10
Bladder Outlet Obstruction
TREATMENT: Conservative – voiding techniques Alpha Blockers 5 Alpha Reductase Inhibitors CIC Foley SP tube

11
Bladder Outlet Obstruction
Alpha Blockers: Tamsulosin (Flomax) Terazosin (Hytrin) Doxazosin (Cardura) Silodosin (Rapaflo) Alfuzosin (Uroxatral)
 Terazosin (Hytrin) Doxazosin (Cardura) Silodosin (Rapaflo) Alfuzosin (Uroxatral)")
12
Bladder Outlet Obstruction
5 Alpha Reductase Inhibitors: Blocks Testosterone conversion to DHT in the prostate. Not first line Consider PSA (getting it and correction) Side effects - breast tender/enlarge, low vol. ejaculate.
 Side effects - breast tender/enlarge, low vol. ejaculate.")
13
Bladder Outlet Obstruction
Others: Combinations – Jalyn (Dutasteride / Tamsulosin Tadalafil (Cialis) low dose daily CIC Foley, SP Tube Surgery - TURP
 low dose daily. CIC. Foley, SP Tube. Surgery - TURP.")
14
CIC Clean Intermittent Catheterization Foley Cath SP Tube

16
I Gotta Peeee!!!

17
Urinary Urgency Incontinence Frequency

19
Urgency w/wo leaking History & physical – voiding history, foods, liquids, stress. PVR, U/A Treatment: AUA Guidelines Behavioral changes, Bladder training, Physical Therapy, Trial ACh medication Work-up if not improved – Cysto, UDS, CT +/- Other treatments: Beta 3 agonist, Neuromodulation, Botox

20
Urgency w/wo leaking Anticholinergics: Oxybutynin (Ditropan)
Tolterodine (Detrol) Fesoterodine (Toviaz) Trospium (Sanctura) Solifenacin (Vesicare) Darifenacin (Enablex) Flavoxate (Urispas)
 Fesoterodine (Toviaz) Trospium (Sanctura) Solifenacin (Vesicare) Darifenacin (Enablex) Flavoxate (Urispas)")
21
Urgency w/wo leaking Beta 3 Agonist: Mirabegron (Myrbetriq) –
Relaxes bladder during filling

22
Urgency w/wo leaking Side Effects: Dizziness Dry mouth Constipation
Urinary retention Contraindicated in narrow angle glaucoma

23
Leaking with cough, sneeze, laughing, getting up.
Stress Incontinence Leaking with cough, sneeze, laughing, getting up.

24
Stress Urinary Incontinence
Treatments: Behavior modification – timed voids, diet, fluids Absorbent pads Kegels Periurethral bulking therapy Surgery

25
Mixed Incontinence

28
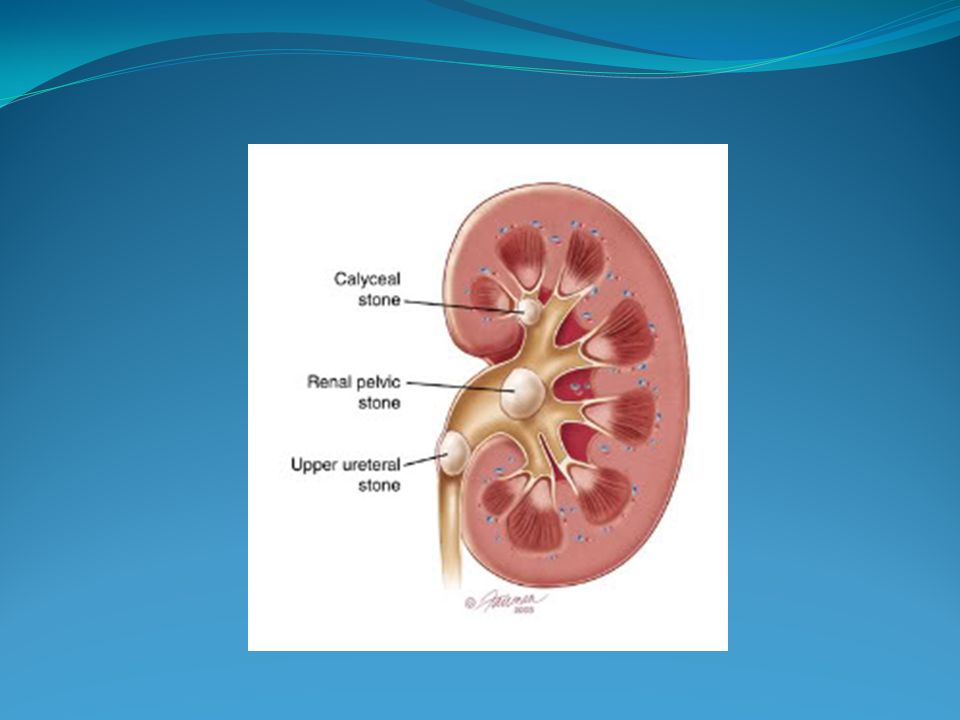
Kidney Stones

30
Kidney stones Presentation: Classic, not so classic
Composition: Ca, Ox, Phosphate, uric acid, struvite (magnesium ammonium phosphate) Prevalence: 1 in 8 will develop stone by age 70 and usually before 50 Think about stone with recurrent UTIs due to: Klebsiella, Proteus, Pseudomonas, Enterococcus. Work up: imaging > CT vs KUB vs RUS Treatment: Flomax, ESWL, Ureteroscopy, PNL, Prevention: 24 hour urines, hydration, low Na, low Ox, hydration.
 Prevalence: 1 in 8 will develop stone by age 70 and usually before 50. Think about stone with recurrent UTIs due to: Klebsiella, Proteus, Pseudomonas, Enterococcus. Work up: imaging > CT vs KUB vs RUS. Treatment: Flomax, ESWL, Ureteroscopy, PNL, Prevention: 24 hour urines, hydration, low Na, low Ox, hydration.")
36
Hydration, Hydration, Hydration….
Kidney Stones Hydration, Hydration, Hydration…. Urine SG > 1.010

37
Hematuria Gross: not disgusting… You can see it.
Microscopic: more than 3 RBC /HPF Smokers: bladder cancer risk x5 Etiology: Stones, infection, kidney disease, prostate, neoplasm. Pathology: benign, malignant. Work up: 3 C’s Follow up for negative evaluation: U/A micro, cytology 3 years

38
THE END

Similar presentations