Download presentation
Presentation is loading. Please wait.

1
National Tuberculosis Program NTP

2
WHAT IS TUBERCULOSIS

3
Tuberculosis is an infectious disease caused mainly by Mycobacterium tuberculosis.
It can affect most organs in the body, but the lung is the main organ affected. If left untreated, each person with smear-positive pulmonary TB will infect, on average, between 10 and 15 persons in each year. Those who will be infected with TB will not necessarily get the disease. The immune system “walls off” the TB bacilli, which can lie dormant for years. On average, 10 percent of the infected individuals develop the disease during their lifetime. When someone’s immune system is weakened, chances of developing TB are increased.

4
History of TB

5
2400 BC Spinal columns of Egyptian mummies show definite Evidence of tubercular decay

6
460 BC HIPPOCRATE: Most widespread disease, almost always fatal
1702 MANGET explained miliary TB 1720 BENJAMIN MARTIN (a new theory of consumption) TB could be caused by wonderfully minute living creature 1854 HERMANN BREHMER (TB is a curable disease) Established first sanatorium in Germany , Beginning of sanatorium era. 1882 ROBERT KOCH, discovered the micro-organisms responsible for TB
 TB could be caused by wonderfully minute living creature HERMANN BREHMER (TB is a curable disease) Established. first sanatorium in Germany , Beginning of sanatorium era ROBERT KOCH, discovered the micro-organisms responsible. for TB.")
7
History of anti-TB drugs

8
1944 STREPTOMYCIN 1949 P A S 1952 ISONIAZID 1954 PYRIZINAMIDE
CYCLOSERINE ETHAMBUTOL RIFAMPICIN OTHER DRUGS USED ETHIONAMIDE,THIACETAZONE, QUINILONES

9
TB Infection

10
Source of Infection: The source of infection can be either:
human: Mycobacterium Tuberculosis animal: Mycobacterium Bovis

11
Mode of Infection: Exogenous: Endogenous:
Inhalation: droplet nuclei, 1-5 microns, consisting of two to three viable bacteria surrounded by a layer of moisture. Ingestion: usually contaminated milk Cutaneous transmission: very rare, the organism gain entrance either through broken skin. Congenital transmission: also very rare, the fetus acquires the infection either transplacentally from the diseased mother through umbilical vein, or by aspirating amniotic fluid that contains viable mycobacteria. Endogenous: Activation of a dormant focus.

12
Natural history of untreated TB
Without treatment, after 5 years. 50% of pulmonary TB patients will be dead. 25% will be healthy (self-cured by strong immune defense). 25% will remain ill with chronic, infectious TB.
. 25% will remain ill with chronic, infectious TB.")
13
TB evolution

14
Primary infection Phenomena that take place when an individual comes into contact with the tubercle bacillus for the first time. 95% of all affected individuals remain asymptomatic or present with minimal clinical manifestations similar to those of common cold. Only 5% develop manifest disease. This phenomenon typically takes place in childhood. As a result of which primary infection is often associated with childhood TB.

15
Primary infection, cont.
Upon arrival in the alveolar region, the bacteria encounter three types of cells that potentially oppose infection: the alveolar macrophages within the alveolar lumen, the key cell the natural killer cells, and the / T lymphocytes.

16
Primary infection, cont.
The initial interaction between M. tuberculosis and alveolar Macrophages involves Non-specific phagocytosis of the bacilli. This phase concludes with destruction of the alveolar macrophages by proliferating intracellular bacilli. Attracted blood monocytes ingest the released bacilli. The monocytes have not been activated yet. The tubercle bacilli increase in number, killing host cells and spread locally. In the lung, intense alveolitis takes place at the expense of the young cells of the mononuclear phagocyte system.

17
Primary infection, cont.
Then Mycobacterial spread via lymphatics towards the regional lymph nodes. In this region, the host immune response to tuberculous infection takes place. In some instances, this immune response is sufficient to arrest the progression of infection. In more often times the bacilli escape towards the lymphatic duct and penetrate the pulmonary bloodstream, from where there is hematogenous spreading of the bacilli to the other organs.

18
Primary infection, cont.
The main target zones of such bacterial dissemination are the highly irrigated organs and tissues—the central nervous system, spongy bone, liver, kidneys, and genitals. In each of these zones, the arriving bacilli are phagocytosed by the local cells of the mononuclear phagocyte system. In most cases, this period implies immunologic control of the infection as a result of two mechanisms: cell-mediated immunity and delayed hypersensitivity.

19
Primary infection, cont.
Delayed hypersensitivity is the phenomenon responsible for the destruction of macrophages that contain intracytoplasmic bacteria, thereby forming a characteristic focus of caseous necrosis. Although the bacteria may survive within this necrotic focus for years, they are unable to reproduce due to the prevalent acidosis, the lack of oxygen, and the presence of inhibitory fatty acids. From the clinical point of view, immunocompetent individuals develop a balance between themselves and the mycobacteria, which persists throughout life until some predisposing event is able to reactivate the infectious focus.

20
Progressive pulmonary component:
Primary TB: Pulmonary: Ghon’s focus Glandular: hilar lymph node, draining lymphangitis The infection develops as interplay between virulence of the organism, and immunity of the host. In 80-90% of infected individuals, immunity takes the upper hand leads to spontaneous healing, resolution, fibrosis and calcification. In 10-20% of infected individuals, virulence takes the upper hand (progressive primary =childhood tuberculosis) Progressive pulmonary component: pneumonic bronchopneumonia cavitation pleural effusion Progressive glandular component: hilar lymph node other lymph nodes atelectasis: middle lobe syndrome haematogenous spread
 Progressive pulmonary component: pneumonic. bronchopneumonia. cavitation. pleural effusion. Progressive glandular component: hilar lymph node other lymph nodes. atelectasis: middle lobe syndrome. haematogenous spread.")
21
Adulthood Tuberculosis
Post-primary: Haematogenous: dissemination by blood stream leads to multiple organs affection Intra-thoracic: miliary, idiopathic effusion, tuberculoma, punched out cavity. Extra-thoracic: meningeal, glandular, renal, bone and joint, etc. Bronchogenic: spread, to other part or other lung Adulthood Tuberculosis minimal, advanced or far advanced lung lesion exceptional extra-pulmonary: laryngitis and enteritis late haematogenous dissemination

22
TB epidemiology

23
Global Burden of Tuberculosis:
In 1993 WHO declared TB a global emergency. It is estimated by WHO worldwide that: A nine million new cases of TB occurred/year Three million TB deaths/year. Tuberculosis poses a major problem for developing countries. Deaths from TB comprise 25 % of all avoidable deaths in developing countries. 95 % of all TB cases occur in developing countries 98 % of TB deaths occur in developing countries. 75 % of TB cases in developing countries are in the economically productive age group ( years).
.")
24
22 high-burden countries: 80% of all new cases
10 100 1000 10000 India China Indonesia Bangladesh Nigeria Pakistan Philippines South Africa Russian Federation Ethiopia DR Congo Viet Nam Kenya UR Tanzania Brazil Thailand Myanmar Zimbabwe Uganda Cambodia Afghanistan Mozambique Estimated new TB cases ('000s)
")
25
Why Does the Global Burden of TB Increase?
Inadequate health services. Improper management practices resulting in poor case detection, diagnosis and treatment. Demographic changes: increasing world population and changing age structure. Impact of HIV. The emergence of resistance to the first line drugs used to treat TB.

26
The pulmonary form of tuberculosis (smear positive and smear negative) represents roughly 80 to 85 percent of all cases. The remaining 15 to 20 percent is made up by cases of extra-pulmonary tuberculosis. The expected number of new smear positive cases in Egypt currently about 10,000 per year. For every new smear-positive pulmonary tuberculosis case usually a case of smear-negative pulmonary or extra-pulmonary tuberculosis will also be present.

27
Magnitude Of TB Problem in Egypt

28
In terms of incidence of tuberculosis, Egypt is ranked among the mid-level incidence countries.
Tuberculosis in Egypt is considered an important public health problem.

30
Indicators

31
Case Detection Indicators
SS+ case detection rate: No. of detected new SS+ cases = >70% Estimated No of new SS+ cases SS+ cases in relation to all pulmonary cases No. of detected new SS+ cases = 50 – 70% Total No. of new pulmonary cases SS+ cases in relation to all TB cases No. of detected new SS+ cases = 50 – 60% Total No. of TB cases detected

32
Treatment Outcome

33
Treatment success No. of patient cured + No. of patient completed treatment = > 85% No. of patient registered

34
Diagnosis of tuberculosis refers to the recognition of an active case, i.e. a patient with symptomatic disease due to lesions caused by Mycobacterium tuberculosis. According to the site of the lesion, TB can be classified to Pulmonary or Extra-Pulmonary Tuberculosis. Pulmonary TB can further be classified to smear positive or smear negative types.

35
Identifying TB suspects

36
What is TB suspect A TB suspect is any person, who presents with symptoms or signs suggestive of tuberculosis, in particular cough of long duration.

37
When to Suspect Pulmonary Tuberculosis?
Persistent cough for more than two weeks. Blood tinged sputum. Breathlessness and chest pain. General symptoms such as: loss of appetite; loss of weight; malaise and tiredness; night sweats and fever. A history of contact with a TB patient .

38
What to do when you suspect a case?
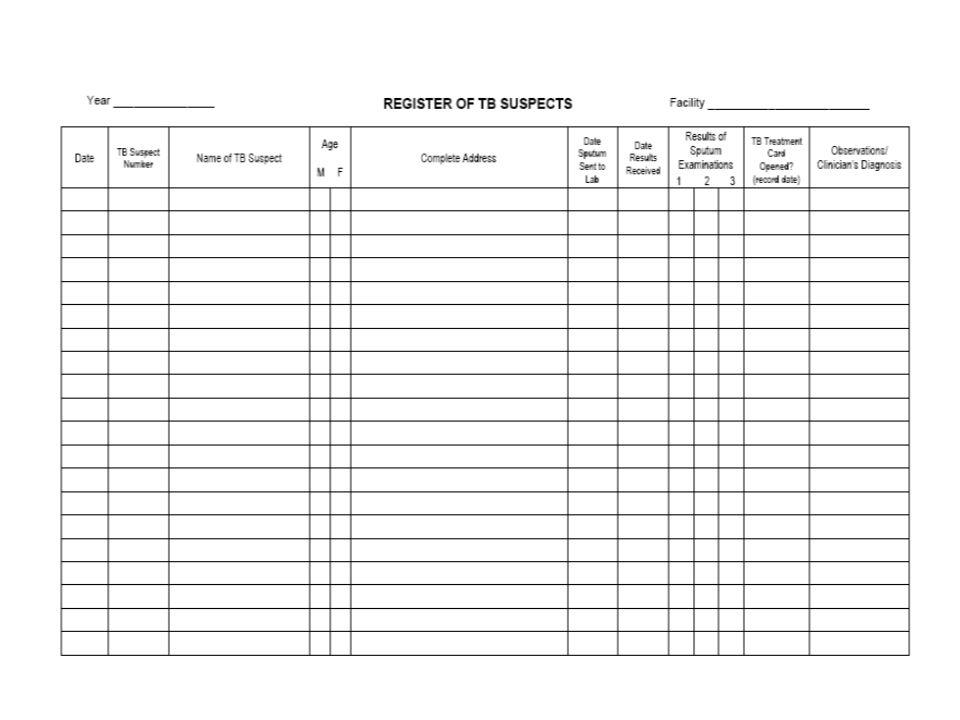
1) List the TB suspect in the Suspect Register The Register of TB Suspects is a record of all patients identified as TB suspects at the health facility, all sputum samples sent to the laboratory & their results.
 List the TB suspect in the Suspect Register. The Register of TB Suspects is a record of all patients identified as TB suspects at the health facility, all sputum samples sent to the laboratory & their results.")
40
2) Collect sputum for smear examination.
3) When the laboratory results are received, record results in the Register. 4) Decide on appropriate action in response to the laboratory results.
 When the laboratory results are received, record results in the Register. 4) Decide on appropriate action in response to the laboratory results.")
41
Diagnosis of TB

42
Diagnosis of Pulmonary TB is A bacteriological one.
Microscopic Direct Smear Examination is an easy and quick procedure. A minimum of three samples must be examined. Cultures: To confirm the diagnosis even in smear negative. To detect drug susceptibility and resistance. To detect the bacilli in any specimen in extra-pulmonary tuberculosis.

43
Sensitivity of sputum smear microscopy
Collection of sputum samples A PTB suspect should submit 3 sputum samples for microscopy. The chances of finding tubercle bacilli are greater with 3 sputum samples than with 2 samples or 1 sample. Secretions build up in the airways overnight. So an early morning sputum sample is more likely than a sample later in the day to contain tubercle bacilli. Sensitivity of sputum smear microscopy Sputum smear microscopy for tubercle bacilli is positive when there are at least 10,000 organisms present per 1 ml of sputum.

44
False positive results of sputum smear microscopy
A false positive result means that the sputum smear result is positive even though the patient does not really have sputum smear-positive PTB. This may arise because of the following: red stain retained by scratches on the slide; contamination of the slide various particles that are acid-fast (e.g. food particles, dye precipitates, other micro-organisms).
.")
45
Causes of false negative results of sputum smear microscopy
EXAMPLE TYPE OF PROBLEM patient provides inadequate sample sputum stored too long before smear microscopy sputum collection faulty smear preparation and staining sputum processing inadequate time spent examining slide inadequate attention during examination sputum smear examination incorrect labeling of sample mistakes in documentation administrative errors

46
TUBERCULIN SKIN TEST Tuberculin is a purified protein derived from tubercle bacilli. Thus, another name for tuberculin is PPD (Purified Protein Derivative). Following infection with M. tuberculosis, a person develops hypersensitivity to tuberculin. Tuberculin injected into the skin of an infected person produces a delayed local reaction after hours. We quantify this reaction by measuring the diameter of skin induration (thickening) at the site of the reaction. Various conditions may suppress this reaction. The reaction only shows that the person has at some time had infection with M. tuberculosis
. Following infection with M. tuberculosis, a person develops hypersensitivity to tuberculin. Tuberculin injected into the skin of an infected person produces a delayed local reaction after hours. We quantify this reaction by measuring the diameter of skin induration (thickening) at the site of the reaction. Various conditions may suppress this reaction. The reaction only shows that the person has at some time had infection with M. tuberculosis.")
47
Tuberculin Skin Test, cont.
A positive test (induration of 10 mm or more) is suggestive for tuberculous infection in children who are not vaccinated with BCG or 5 years or more after vaccination. A positive test (induration of 15 mm or more) is suggestive for tuberculous infection in children who are vaccinated with BCG. A negative test in adults may be suggestive of absence of tuberculous infection. False negative test may be obtained in immunosuppressed individuals.
 is suggestive for tuberculous infection in children who are not vaccinated with BCG or 5 years or more after vaccination. A positive test (induration of 15 mm or more) is suggestive for tuberculous infection in children who are vaccinated with BCG. A negative test in adults may be suggestive of absence of tuberculous infection. False negative test may be obtained in immunosuppressed individuals.")
48
CONDITIONS WHICH MAY SUPPRESS THE TUBERCULIN SKIN TEST
HIV infection Malnutrition Severe bacterial infections, including TB itself Viral infections, e.g. measles, chickenpox, glandular fever Cancer Immunosuppressive drugs, e.g. steroids

49
Tuberculin Testing

50
Chest X-rays in diagnosis
No certain x-ray pattern is specific to TB INDICATIONS FOR CHEST X-RAY Positive sputum smear The first screening test for PTB suspects is sputum smear microscopy. In most cases of sputum smear-positive PTB a chest X-ray is un-necessary. In those few cases of sputum smear-positive PTB when a chest X-ray is necessary, the indications are as follows:

51
a) suspected complications in the breathless patient, needing specific treatment, e.g. pneumothorax, (pericardial effusion or pleural effusion - positive sputum smear is rare); b) frequent or severe haemoptysis (to exclude bronchiectasis or aspergilloma); c) only 1 sputum smear positive out of 3 (in this case, an abnormal chest X-ray is a necessary additional criterion for the diagnosis of sputum smear-positive PTB).
 frequent or severe haemoptysis (to exclude bronchiectasis or aspergilloma); c) only 1 sputum smear positive out of 3 (in this case, an abnormal chest X-ray is a necessary additional criterion for the diagnosis of sputum smear-positive PTB).")
52
Radiological Examination

53
Other methods of diagnosis
Biopsies PCR

54
Childhood Tuberculosis

55
History: Chronic cough
Longer than 2 weeks not improving with ordinary treatment and getting worse Fever Longer than 7 days not responding to antibiotics and treatment of common conditions Antibiotics to be given in such cases Weight loss documented weight loss or failure to thrive. failure to gain weight if on feeding scheme after 1month.

56
SCORE SYSTEM FOR THE DIAGNOSIS OF TB IN CHILDREN
A score system is one way of trying to improve the diagnosis of childhood TB. The basis of a score system is the careful and systematic collection of diagnostic information. A score of 7 or more indicates a high likelihood of TB.

57
No response to nonspecific treatment
score 4 3 2 1 feature General 4w< 2-4w 2w> Duration of illness 60%> 60-80% 80%< Weight for age Proved +VE Reported -VE Family history positive Tuberculin test Not improving After 4 w Malnutrition No response to nonspecific treatment Unexplained fever and night sweats

58
Angle deformity of the spine
Local Lymph nodes Joint or bone swelling Abd. mass or ascites CNS findings Angle deformity of the spine Total score

59
Case definitions

60
A smear-positive pulmonary TB
A patient with at least two sputum specimens positive for AFB; or, A patient with at least one sputum specimen positive for AFB, with culture positive for M. tuberculosis, or with radiological abnormalities consistent with pulmonary TB. A smear-negative pulmonary TB A patient with two sets (taken at least two weeks apart) of at least three sputum specimens that are negative for AFB, radiological abnormalities consistent with pulmonary TB and a lack of clinical response to at least two weeks of a broad spectrum antibiotic Or, A patient who is severely ill with at least three sputum specimens negative for AFB and radiological abnormalities consistent with extensive pulmonary TB N.B. a patient whose initial sputum-specimens were negative and who did have sputum sent for culture initially should be considered a sputum-negative pulmonary TB even if the sputum culture result is positive.
 of at least three sputum specimens that are negative for AFB, radiological abnormalities consistent with pulmonary TB and a lack of clinical response to at least two weeks of a broad spectrum antibiotic Or, A patient who is severely ill with at least three sputum specimens negative for AFB and radiological abnormalities consistent with extensive pulmonary TB. N.B. a patient whose initial sputum-specimens were negative and who did have sputum sent for culture initially should be considered a sputum-negative pulmonary TB even if the sputum culture result is positive.")
61
New case A patient who has never had treatment for TB or who has taken drugs for less than one month
Relapse A patient who is declared cured by a physician, after one full course of chemotherapy, and has become sputum smear-positive Treatment failure A patient who, while on treatment, remained or became again smear-positive 5 months or later after commencing treatment; or, A patient who was initially smear-negative before starting treatment and became smear-positive after the second month of treatment

62
Treatment after interruption
A patient who interrupts his treatment for 2 months or more (defaulter) and returns with smear positive sputum Others A patient who was either smear-negative pulmonary TB or extra-pulmonary TB, completed treatment and returned with symptoms and active disease or chronic cases. chronic case: A patient who remained or became again smear-positive after completing a fully supervised retreatment regimen.
 and returns with smear positive sputum. Others. A patient who was either smear-negative pulmonary TB or extra-pulmonary TB, completed treatment and returned with symptoms and active disease or chronic cases. chronic case: A patient who remained or became again smear-positive after completing a fully supervised retreatment regimen.")
63
TB treatment

64
TB chemotherapy should be based on two important microbiological considerations:
The combination of drugs to avoid the development of resistance. The need for prolonged chemotherapy to prevent disease relapse.

65
All mono-therapeutic regimens (real or masked by combination with drugs to which bacilli are resistant) lead to treatment failure and to the development of resistance. When three or more drugs are administered, the risk of resistance is practically zero.

66
Phases of treatment: The intensive phase The continuation phase
usually covers the first 2 months of treatment. During this phase, most of the bacilli will be killed. The sputum converts from positive to negative in more than 80 % of the new patients within the first 2 months of treatment. The continuation phase usually lasts 4-6 months, depending on the treatment regimen. This phase is intended to eliminate the remaining dormant bacilli. These dormant bacilli decrease constantly as treatment intake progresses. Since it is not possible to identify which patients still have dormant bacilli, all patients should continue their treatment until the end of the prescribed period, to limit the number of relapses.

67
First-line anti-tuberculosis drugs, action and side effects

68
RECOMMENDED DAILY DOSAGE (DOSE RANGE),mg/kg
DRUG RECOMMENDED DAILY DOSAGE (DOSE RANGE),mg/kg Isoniazide (H) 5 (4–6) Rifampicin (R) 10 (8–12) Pirazinamide (Z) 25 (20–30) Streptomycin (S) 15 (12–18) Ethambutol (E) 15 (15–20)
,mg/kg. Isoniazide (H) 5 (4–6) Rifampicin (R) 10 (8–12) Pirazinamide (Z) 25 (20–30) Streptomycin (S) 15 (12–18) Ethambutol (E) 15 (15–20)")
70
Treatment regimens Continuation Initial Patient Category
Treatment category 4/HR 2/SHRZ OR 2/EHRZ New smear +ve PTB. New smear –ve New forms of extra-Pulmonary TB. I

71
Treatment regimens, cont
Continuation Initial Patient Category Treatment category 5/HRE 2/SHRZE then 1/HRZE Sputum smear +ve Relapse. Treatment after failure. Treatment after interruption. II

72
TREATMENT OUTCOME Cure
A patient who is smear-negative in the month of treatment and on at least one previous occasion Treatment completed A patient who has completed treatment but who does not meet the criteria to be classified as a cure or a failure Treatment failure A patient who remains or becomes again smear-positive at five months or later during treatment* Died A patient who dies for any reason during the course of treatment Default A patient whose treatment was interrupted for two months or more Transfer out A patient who has been transferred to another reporting unit outside the Governorate and for whom the treatment outcome is not known

73
DOTS means directly observed treatment with short course chemotherapy
DOTS strategy DOTS means directly observed treatment with short course chemotherapy Principles of DOTS strategy Government commitment to TB control Case detection through sputum-smear microscopy in the general health services Standardized short-course chemotherapy to, at least, all smear-positive TB cases under proper case management conditions Regular, uninterrupted supply of all essential anti-tuberculous drugs Monitoring system for programme supervision and evaluation

74
Role of PHC in DOTS implementation
Provide TB patients with daily supervised treatment with anti-TB drugs according to prescribed regimen, dosage and duration Provide patients, who are unable to attend at the PHC centre on a daily basis (e.g. handicapped patients) with supervised treatment at the patient’s home. DOT at the patient’s home, if necessary Retrieve patients who did not attend the PHC centre for their daily treatment Record daily attendance and anti-TB drug intake in the TB treatment card Health education and counseling to TB patients, their contacts and the community Timely referral of TB patients to the chest clinic for follow up sputum examination Order and collect the required quantity of anti-TB drugs for TB patients Ensure that the anti-TB drugs present in the unit are not expired Refer contacts of TB patients to chest clinic Refer TB suspects to chest clinic
 with supervised treatment at the patient’s home. DOT at the patient’s home, if necessary. Retrieve patients who did not attend the PHC centre for their daily treatment. Record daily attendance and anti-TB drug intake in the TB treatment card. Health education and counseling to TB patients, their contacts and the community. Timely referral of TB patients to the chest clinic for follow up sputum examination. Order and collect the required quantity of anti-TB drugs for TB patients. Ensure that the anti-TB drugs present in the unit are not expired. Refer contacts of TB patients to chest clinic. Refer TB suspects to chest clinic.")
75
DR-Tuberculosis

76
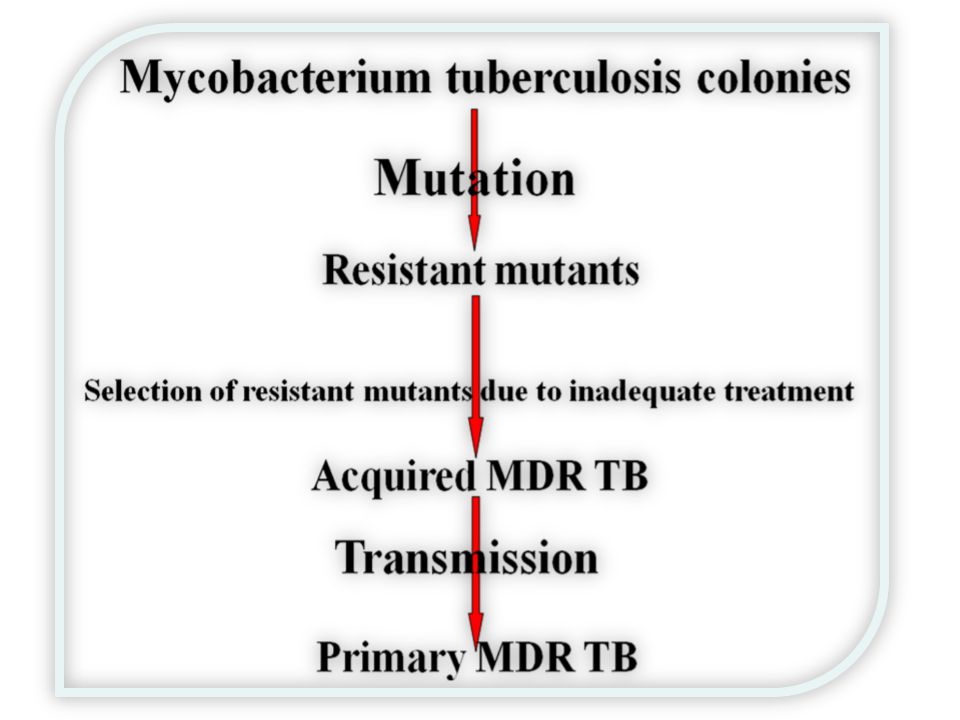
Causes of drug-resistant tuberculosis:
From a microbiological perspective, resistance is caused by a genetic mutation. An inadequate or poorly administered treatment regimen allows a drug-resistant strain to become the dominant strain; hence, TB is essentially a man-made phenomenon.

78
Factors That May Lead To Developing Resistance

79
Factors may include: HEALTH-CARE PROVIDERS through
- INADEQUATE REGIMENS: - Poorly organized or funded TB control programs. - Inappropriate, Absence of or Noncompliance with guidelines - Poor training - No monitoring of treatment.

80
- Lack of information, poor health education - Adverse effects.
2- PATIENTS through INADEQUATE DRUG INTAKE (patient incompliance): - Poor adherence - Lack of information, poor health education - Adverse effects. - Social barriers. - Malabsorption.
: - Poor adherence. - Lack of information, poor health education. - Adverse effects. - Social barriers. - Malabsorption.")
81
3- DRUGS through: Poor quality Stock-outs or delivery disruptions.
Wrong dose. Poor storage conditions

82
Different resistance patterns

83
Mono-resistance, Poly-resistance,
colonies are resistant to only one of the first-line anti-TB drugs. Poly-resistance, colonies are resistant to more than one of the first line anti-TB drugs but do not combine resistance to both Isoniazid and Rifampicin. Examples of poly-resistance may include Streptomycin, Isoniazid and Ethambutol or Streptomycin, Rifampicin and Ethambutol.

84
Multiple drug resistant,
colonies combine resistance to at least Isoniazid and Rifampicin. Extensively Drug Resistant TB (XDR-TB): Colonies are resistant to: 1st Line drugs , at least Rifampicin and Isoniazid, (MDR-TB) A fluoroquinolone One or more of the following injectable drugs: kanamycin Amikacin Capreomycin
: Colonies are resistant to: 1st Line drugs , at least Rifampicin and Isoniazid, (MDR-TB) A fluoroquinolone. One or more of the following injectable drugs: kanamycin. Amikacin. Capreomycin.")
85
Primary resistance and acquired resistance:
“Primary resistance” means that the patient was infected with already resistant bacilli. “Acquired resistance” means that patient was initially infected with sensitive bacilli but developed resistance of any pattern during the course of treatment because of any or a combination of the previously mentioned causes

86
Treatment regimens for DR-TB in Egypt

87
Treatment regimen Patient resistant to Regimen I 3 months: canamycin daily + Ofloxacin + Cycloserine + Ethionamide + PAS then: 6 months canamycin 5 times a week + previous drugs then: 12 months Ofloxacin + Cycloserine + Ethionamide + PAS RHSE Regimen II 3 months: canamycin + Ofloxacin + Ethambutol + Ethionamide + Cycloserine then: 6 months: canamycin 5 times a week + previous drugs then: 12 months: Ofloxacin + Ethambutol + Ethionamide + Cycloserine RHS Regimen III 3 months streptomycin daily + Ethambutol + Pyrazinamide + Ofloxacin + PAS then: 6 months streptomycin 5 times a week + previous drugs then: 12 months: Ethambutol + Pyrazinamide + Ofloxacin + PAS RH

Similar presentations
















 Environmental.>")




