Download presentation
Presentation is loading. Please wait.

1
Diseases Resulting from Fungi and Yeasts
Kristy P. Gilbert, D.O. February 8, 2005

2
Superficial mycoses AKA dermatophytes
Cause only stratum corneum, hair and nail infection Three genera: Microsporum, Trichophyton, Epidermophyton Division into: 1) tinea capitis, 2) tinea barbae, 3) tinea faciei, 4) tinea corporis, 5) tinea manus, 6) tinea pedis, 7) tinea cruris, 8)onychomycosis
 tinea capitis, 2) tinea barbae, 3) tinea faciei, 4) tinea corporis, 5) tinea manus, 6) tinea pedis, 7) tinea cruris, 8)onychomycosis.")
3
Host factors Immunosuppressed pts- cancer, diabetes
AIDS, connective tissue disorders Genetic susceptibility may be related to types of keratin or degree/mix of cutaneous lipids produced, cutaneous barrier compromise Surface antigens-ABO system-one study of 108 culture proven dermatophytosis pts noted type A blood prone to chronic disease Human steroid hormones can inhibit growth of dermatophytes (androgens like androstenedione) One group believes this high susceptibility of Trichophyton rubrum & Epidermophyton floccosum to intrafollicular androstenedione is a reason why these species do not cause tinea capitis
 One group believes this high susceptibility of Trichophyton rubrum & Epidermophyton floccosum to intrafollicular androstenedione is a reason why these species do not cause tinea capitis.")
4
Imidazoles Clotrimazole, miconazole, sulconazole, oxiconazole, and ketoconazole Mostly used for topical tx Inhibit cytochrome P alpha-demethylase (an essential enzyme in ergosterol synthesis) Ketaconazole has wide spectrum against dermatophytes, yeasts, and some systemic mycoses Ketaconazole has the potential for serious drug interactions and a higher incidence of hepatotoxicity during long-term daily therapy
 Ketaconazole has wide spectrum against dermatophytes, yeasts, and some systemic mycoses. Ketaconazole has the potential for serious drug interactions and a higher incidence of hepatotoxicity during long-term daily therapy.")
5
Allylamines Naftifine, terbinafine, butenafine
Inhibites squalene epoxydation Terbinafine has less activity against Candida species in vitro studies then triazoles, but is effective clinically Terbinafine is ineffective in the oral tx of tinea versicolor but is effective topically Few drug interactions have been reported Bioavailability is unchanged in food Hepatotoxicity, leukopenia, severe exanthems, and taste disturbances uncommon, but should be monitored for clinically and by lab testing if continuous dosing over 6 weeks

6
Polyene Nystatin Irreversibly binding to ergosterol-an essential component of fungal cell membranes

7
Triazoles Itraconazole, Fluconazole Affect P450 system
Numerous drug interactions occur Need to know pt’s current meds Broadest spectrum to dermatophytes and Candida species, and Malassezia furfur Itraconazole is fungistatic- food increases its absorption , antacids and gastric acid secretion suppressors produce erratic or lowered absorption Pulse dosing limits concern over lab abnormalities Fluconazole’s absorption is unaffected by food

8
Tinea Capitis Occurs chiefly in schoolchildren
Boys more frequently than girls; except epidemics caused by Trichophyton tonsurans where there is equal frequency Divided into inflammatory and non-inflammatory Tinea capitis can be caused by all pathogenic dermatophytes except Epidermophyton floccosum and T. concentricum In U.S. most caused by T. tonsurans

9
Tinea Capitis

10
Noninflammatory M. audouinii infections present as the classic form
Characterized by multiple scaly lesions (“gray-patch”), stubs of broken hair Over past 30 yrs, M. audouinii infections are being replaced by increasing numbers of “black-dot” ringworm, caused primarily by T. tonsurans and occasionally by T. violaceum In the U.S. T. tonsurans is the most common cause
, stubs of broken hair. Over past 30 yrs, M. audouinii infections are being replaced by increasing numbers of black-dot ringworm, caused primarily by T. tonsurans and occasionally by T. violaceum. In the U.S. T. tonsurans is the most common cause.")
11
Noninflammatory Tinea Capitis
“Black dot” ringworm, caused by T. tonsurans & occasionally T. violaceum presents as multiple areas of alopecia studded with black dots representing infected hairs broken off at or below the surface of the scalp

13
Black dot tinea

14
Black dot ringworm caused by Trichophyton tonsurans

15
Inflammatory Usually caused by M. canis
Can be caused by T. mentagrophytes, T. tonsurans, M. gypsem, or T. verrucosum M. canis begin as scaly, erythematous, papular eruptions with loose and broken-off hairs, followed by varying degrees of inflammation A localized spot accompanied by pronounced swelling, with developing bogginess and induration exuding pus develops- kerion celsii A delayed type hypersensitivity reaction to fungal elements With extensive lesions fever, pain, and regional lymphadenopathy may occur

16
Kerion Kerion may be followed by scarring and permanent alopecia in areas of inflammation and suppuration Systemic steroids for short periods will greatly diminish the inflammatory response and reduce the risk of scarring

17
Kerion: inflammatory rxn of tinea capitis caused by Microsporum canis or Trichophyton mentagrophytes

18
Permanent scarring alopecia post-kerion

19
Kerion: red, oozing, hairless plaque

20
Favus Rare in the U.S. Most severe form of dermatophyte hair infection
Most frequently cause by T. schoenleinii Hyphae and air spaces seen within hair shaft Bluish white fluorescence under Wood’s light Thick, yellow crusts composed of hyphae and skin debris (‘scutula’) Scarring alopecia may develop
 Scarring alopecia may develop.")
21
Favus with scarring alopecia and scutula

22
Scarring after favus infection

23
Etiology Tinea capitis can be cause by any one of several species: T. tonsurans, M. audouinii (human to human), and M. canis (animals to human) Endothrix types-T. tonsurans (black-dot ringworm) and T. violaceum Ectothrix found on scalp are T. verrucosum & T. mentagrophytes, M. canis
 and T. violaceum. Ectothrix found on scalp are T. verrucosum & T. mentagrophytes, M. canis.")
24
Diagnosis Wood’s light
Ultraviolet of 365 nm wavelength is obtained by passing a beam through a Wood’s filter composed of nickel oxide-containing glass A simple form is the 125-volt purple bulb Fluorescent-positive infections are caused by :T. schoenleinii, M. canis, M. audouinii, M. distortum, M. ferrugineum Hairs infected with T. tonsurans, T. verrucosum, & T. violaceum and others of endothrix do not fluoresce The fluorescent substance is pteridine

25
Diagnosis KOH Scales or hairs cleared with it can still be cultured
Two or three loose hairs are removed Hairs are placed on slide with a drop of 10-20% solution of KOH A cover slip is applied, specimen is warmed until hairs are macerated Examine under low, then high power Scales or hairs cleared with it can still be cultured

26
DTM DTM contains cycloheximide to reduce growth of contaminants and a colored pH indicator to denote the alkali-producing dermatophytes Some clinically relevant nondermatophyte fungi are cycloheximide sensitive (Candida tropicalis, Scopulariopsis brevicaulis, Cryptococcus neoformans, Pseudoallescheria boydii, Trichosporon beigelii and Aspergillus spp.)
")
28
Ectothrix type in Microsporum canis-note small spores around hair shaft

29
Endothrix spores in hair with Trichophyton tonsurans

30
Endothrix in T. scoenleinii showing characteristic bubbles of air

31
Endothrix infection, (low-power KOH mount): arthroconidia noted within hair shaft
Endothrix infection (high-power KOH mount) showing total hair shaft involvement
 showing total hair shaft involvement.")
33
T. tonsurans This microoraganism grows slowly in culture to produce a granular or powdery yellow to red, brown, or buff colony Crater formation with radial grooves may be produced Microconidia may be seen regularly Dx confirmed by the fact that cultures grow poorly or not at all without thiamine

34
T. mentagrophytes Culture growth is velvety or granular or fluffy, flat or furrowed, light buff, white, or sometimes pink Back of the culture can vary from buff to dark red Round microconidia borne laterally and in clusters confirm dx within 2 weeks Spirals are sometimes present Macroconidia may be seen

35
T. verrucosum Growth is slow and cannot be observed well for at least 3 weeks Colony is compact, glassy, velvety, heaped or furrowed, and usually white, but may be yellow or gray Chlamydospores (round swellings along the hyphal structures) are present in early cultures Microconidia may be seen
 are present in early cultures. Microconidia may be seen.")
36
M. audouinii Gross appearance shows a slowly growing, matted, velvety, light brown colony Back of which is reddish brown to orange Under microscope a few large multiseptate macroconidia (macroaleuriospores) are seen Microconidia (microaleuriospores) in a lateral position on hyphae are clavate Racquet mycelium, chlamydospores, and pectinate hyphae are seen sometimes
 are seen. Microconidia (microaleuriospores) in a lateral position on hyphae are clavate. Racquet mycelium, chlamydospores, and pectinate hyphae are seen sometimes.")
37
M. canis Culture shows profuse, fuzzy, cottony, aerial mycelia tending to become powdery in the center Color is buff to light brown Back of colony is lemon to orange-yellow Numerous spindle-shaped multiseptate microconidia and thick-walled macroconidia are present Clavate microconidia are found along with chlamydospores and pectinate bodies

39
Treatment Griseofulvin of ultramicronized form, 10 mg/kg/day, is the daily dose recommended for children Grifulvin V is the only oral suspension available for children unable to swallow tablets-dose is 20 mg/kg/day Tx should continue for 2-4 months, or for at least 2 weeks after negative microscopic and culture examinations are obtained Griseofulvin does not primarily affect the delayed type hypersensitivity reaction responsible for the inflammation in kerion For this, systemic steroids, to minimize scarring, can be given simultaneously

40
Treatment Terbinafine -effective for Trichophyton infections
-3-6mg/kg/day for 1 to 4 weeks -Microsporum infections may require larger doses and longer courses of therapy Itraconazole Fluconazole Selenium Sulfide or Ketoconazole shampoo as an adjunct

42
Tinea Barbae AKA Tinea sycosis, barber’s itch Uncommon
Occurs chiefly among those in agriculture Involvement is mostly one-sided on neck or face Two clinical types are: deep, nodular, suppurative lesions; and superficial, crusted, partially bald patches with folliculitis

43
Tinea Barbae Superficial crusted type
mild pustular folliculitis with broken-off hairs (T. violaceum) or without broken-off hairs (T. rubrum) Affected hairs are loose, dry, and brittle When extracted bulb appears intact
 or without broken-off hairs (T. rubrum) Affected hairs are loose, dry, and brittle. When extracted bulb appears intact.")
44
Tinea Barbae Deep type Caused mostly by T. mentagrophytes or T. verrucosum Swellings are usually confluent and form diffuse boggy infiltrates with abscesses Pus may be expressed Lesions are limited to one part of face or neck in men

45
Diagnosis-Tinea Barbae
Clinical Confirmed by microscopic findings and by standard culture techniques Rarely, Epidermophyton floccosum may cause widespread verrucous lesions known as verrucous epidermophytosis

46
Verrucous epidermophytosis from Epidermphyton floccosum

47
Complete resolution after 48 days of Griseofulvin

48
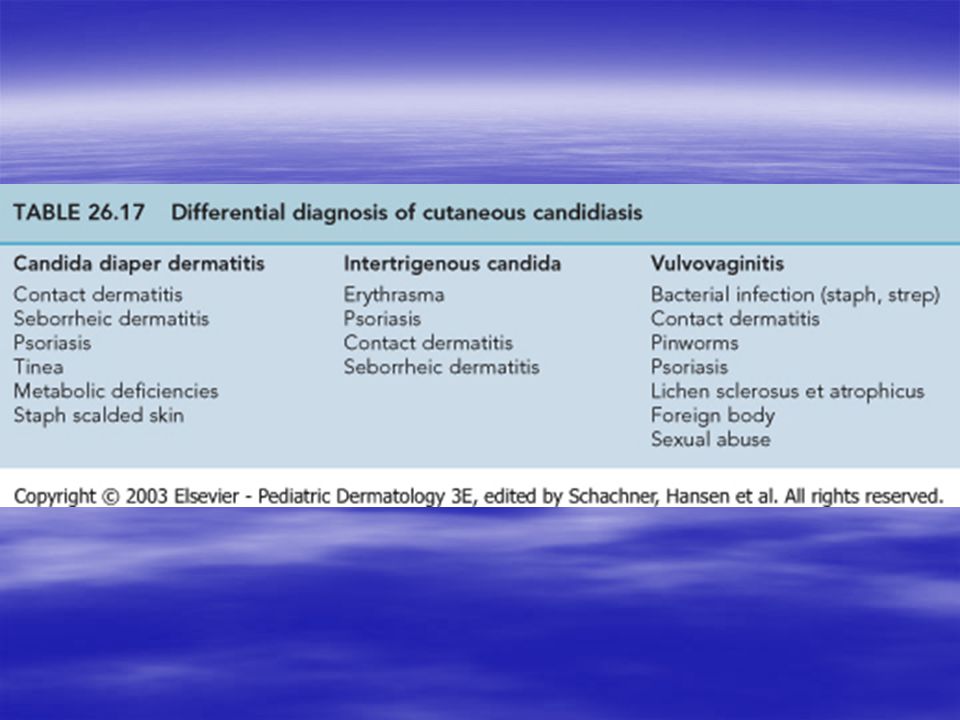
Differential Diagnosis
Sycosis vulgaris (staphlococcal folliculitis)-lesions are pustules and papules, pierced in the center by a hair, which is loose and easily extracted after suppuration has occurred Contact dermatitis Herpes infections
-lesions are pustules and papules, pierced in the center by a hair, which is loose and easily extracted after suppuration has occurred. Contact dermatitis. Herpes infections.")
49
Tinea barbae-Trichophyton mentagrophytes

52
Treatment-Tinea Barbae
Oral antifungals are required Topical agents as adjunctive therapy Micronized or ultramicronized griseofulvin orally: dosage of 500–1000 mg or mg respectively Tx usually for 4-6 weeks

53
Treatment-Tinea Barbae
Other orals that have been effective: ketoconazole, fluconazole, itraconazole, and terbinafine Topical antifungals should be applied from the beginning of tx Affected parts should be bathed thoroughly in soap and water Healthy areas that are not epilated may be shaved or clipped When kerion is present a short course of systemic steriod therapy may help reduce inflammation and risk of scarring

54
Tinea Faciei Fungal infection of the face (apart from the beard)
Must have high index of suspicion Mistaken for seborrheic dermatitis, contact dermatitis, lupus, or photosensitive dermatosis Erythematous, slightly scaling, indistinct borders are usually seen (best location for KOH scrapings) Typical annular rings are usually lacking & lesions are exquisitely photosensitive Usually caused by T. rubrum, T. mentagrophytes, or M. canis
 Typical annular rings are usually lacking & lesions are exquisitely photosensitive. Usually caused by T. rubrum, T. mentagrophytes, or M. canis.")
55
Tinea faciei (Microsporum canis) in a child
 in a child")
56
Treatment Topical antifungals
If fungal folliculitis is present, oral medication is required Oral griseofulvin administered for 2-4 weeks, as well as fluconazole, itraconazole, or terbinafine are all effective particularly in combination with topical therapy

57
Tinea Corporis(Tinea Circinata)
All superficial dermatophyte infections of the skin except the scalp, beard, face, hands, feet, and groin Sites of predilection are neck, upper and lower extremities, and trunk Characterized by one or more circular, sharply circumscribed, slightly erythematous, dry, scaly, usually hypopigmented patches Advancing scaling edge is usually prominent

58
Tinea corporis in a child, caused by Microsporum canis

59
Tinea corporis (Trichophyton rubrum)
Note sharp margins and central clearing

60
Tinea Corporis In some cases concentric circles form rings in one another, making intricate patterns (tinea imbricata) Widespread tinea corporis may be the presenting sign of AIDS

61
Tinea corporis: large gyrate plaque with advancing border, perhaps worsened by diapering

62
Histopathology Better ways to make diagnosis
But if compact orthokeratosis is found in a section, a search for fungal hyphae should be performed This is diagnostic

63
Etiology-Tinea Corporis
Microsporum canis, T. rubrum, T. mentagrophytes- most common T. rubrum is is the most common dermatophyte in the U.S. and worldwide T. tonsurans has experienced a dramatic rise as a cause of tinea corporis as it has for tinea capitis In children, M. canis is the cause of the “moist” type of tinea circinata

64
Epidemiology Tinea corporis is frequently seen in children-particularly those exposed to animals with ringworm (M. canis), especially CATS, dogs and less commonly, horses and cattle In adults excessive perspiration is the most common factor Personal history or close contact with tinea capitis or tinea pedis is another important factor Incidence is especially high in hot, humid areas of the world
, especially CATS, dogs and less commonly, horses and cattle. In adults excessive perspiration is the most common factor. Personal history or close contact with tinea capitis or tinea pedis is another important factor. Incidence is especially high in hot, humid areas of the world.")
65
Treatment-Tinea Corporis
When tinea corporis is caused by T. tonsurans, M. canis, T. mentagrophytes, or T. rubrum; griseofulvin, terbinafine, itraconazole, and fluconazole are all effective The ultra-micronized form may be used at a dose of mg once/day for 4-6 weeks This dose may be increased to twice daily if needed Terbinafine, itraconazole, and fluconazole are effective Terbinafine at 250 mg/day for two weeks Itraconazole 200 mg B.I.D. for one week Fluconazole 150 mg once/week for 4 weeks

66
Treatment When only 1-2 patches occur, topical tx is effective
Most are between 2-4 weeks with twice daily use Econazole, ketaconazole, oxiconazole, and terbinafine may be used once daily With terbinafine the course can be shortened to 1 week

67
Treatment Creams are more effective than lotions
Sulconazole may be less irritating in folded areas Castellani paint (which is colorless if made without fuchin) is very effective Salicylic acid 3-5%, or half-strength Whitfield’s ointment, both standbys 30 yrs ago, are rarely used today Addition of a low-potency steroid cream during the initial 3-5 days of therapy can decrease irritation rapidly without compromising the effectiveness of the antifungal
 is very effective. Salicylic acid 3-5%, or half-strength Whitfield’s ointment, both standbys 30 yrs ago, are rarely used today. Addition of a low-potency steroid cream during the initial 3-5 days of therapy can decrease irritation rapidly without compromising the effectiveness of the antifungal.")
68
Other Forms of Tinea Corporis
Trichophytic Granuloma or Perifollicular Granuloma or Majocchi’s Granuloma or Tinea Incognito A deep, pustular type of tinea circinata resembling a carbuncle or kerion observed on the glabrous skin A circumscribed, annular, raised, crusty, and boggy granuloma Follicles are distended with viscid purulent material Most frequently on the shins or wrists

69
Majocchi’s granuloma H&E pale blue-staining fungal hyphae within hair shaft

70
Majocchi’s granuloma: PAS reveals multiple organisms that have replaced a fragment of hair shaft embedded in a sea of neutrophils

71
Tinea Imbricata (Tokelau)
Superficial fungal infection limited to southwest Polynesia, Melanesia, Southeast Asia, India, and Central America Characterized by concentric rings of scales forming extensive patches with polycyclic borders Small macular patch splits in center and forms large, flaky scales attached at the periphery Resultant ring spreads peripherally and another brownish macule appears in the center and undergoes the process again

72
Tinea Imbricata When fully developed the eruption is characterized by concentrically arranged rings or parallel undulating lines of scales overlapping each other like shingles on a roof (imbrex means shingle) Causative fungus is T. concentricum TOC is griseofulvin- in same form as for tinea corporis Other options are terbinafine, fluconazole, and itraconazole Several courses of therapy may be needed May need to remove patient from hot, humid environment
 Causative fungus is T. concentricum. TOC is griseofulvin- in same form as for tinea corporis. Other options are terbinafine, fluconazole, and itraconazole. Several courses of therapy may be needed. May need to remove patient from hot, humid environment.")
73
Tinea imbricata in New Guinea native

74
Tinea imbricata: concentric rings of scale caused by T. concentricum

75
Tinea Cruris AKA jock itch Most common in men
On upper and inner thighs Begins as a small erythematous and scaling or vesicular and crusted patch Spreads peripherally and partly clears in the center Penoscrotal fold or sides of scrotum are seldom involved; penis not involved

76
Tinea cruris in a man

77
Tinea cruris in a woman

79
Etiology-Tinea Cruris
T. mentagrophytes & E. floccosum & T. rubrum usual cause Frequently associated with tinea pedis b/c of contaminated clothing Heat and high humidity Tight jockey shorts!

80
Treatment Reduce perspiration and enhance evaporation from crural area
Keep as dry as possible by wearing loose underclothing Plain talcum powder or antifungal powders Specific topical and oral treatment is same as that described under tinea corporis

81
Tinea in diaper area

82
Tinea Pedis AKA athlete’s foot Most common fungal disease(by far)
Primary lesions often are macerated with occasional vesiculation, and fissures between the toes Extreme pruritus

83
Tinea pedis showing interdigital scalping
T. mentagrophytes

84
Interdigital scaling with vesiculation caused by T. mentagrophytes

85
Dermatophytosis of the soles
Trichophyton mantagrophytes

86
Acute vesiculobullous eruption on sole caused by Trichophyton mentagrophytes

87
TP-Trichophyton rubrum
T. rubrum causes the majority of cases Produces a relatively noninflammatory type of dermatophytosis characterized by a dull erythema and pronounced scaling involving the entire sole and sides of feet Producing a moccasin or sandal appearance

88
Tinea pedis and onychomycosis in father/son pair.
Father shows classic moccasin distribution of tinea pedis and son shows distal subungual onychomycosis

89
Tinea manus Tinea infection of hands that is dry, scaly, and erythematous may occur Suggestive of infection with T. rubrum Other areas are frequently affected at the same time

90
Trichophyton rubrum infections

91
Differential diagnosis
Allergic contact or irritant dermatitis-especially occupational Pompholyx Atopic dermatitis Psoriasis Lamellar dyshidrosis Eczematoid or dyshidrotic lesions of unknown cause on hands should prompt a search for clinical evidence of dermatophytosis of feet etc.

92
Fungus filaments under KOH mount

93
Mosaic fungus

94
Prophylaxis Hyperhidrosis is a predisposing factor
Dry toes after bathing Tolnaftate powder or Zeasorb medicated powders for feet Plain talc, cornstartch, or rice powder may be dusted into socks and shoes to keep feet dry

95
Treatment Topical antifungals
With significant maceration wet dressings or soaks with solutions such as aluminum acetate, one part to 20 parts of water Anti-inflammatory effects of corticosteroids are markedly beneficial Topical antibiotic ointments effective against gram-negative organisms (gentamicin), in tx of the moist type of interdigital lesions In ulcerative type of gram-negative toe web infections, systemic floxins are needed
, in tx of the moist type of interdigital lesions. In ulcerative type of gram-negative toe web infections, systemic floxins are needed.")
96
Treatment Keratolytic agents, such as salicylic acid, lactic acid lotions, and Carmol are therapeutic when fungus is protected by a thick layer of overlying skin (i.e. soles) Griseofulvin is only effective against dermatophytes When infection is caused by T. mentagrophytes, griseofulvin does not decrease inflammatory reaction
 Griseofulvin is only effective against dermatophytes. When infection is caused by T. mentagrophytes, griseofulvin does not decrease inflammatory reaction.")
97
Treatment- dosing Griseofulvin in ultramicronized particles taken orally in doses of mg daily Dosage for children is 10 mg/kg/day Period of treatment depends on response Repeated KOH scrapings and culture should be negative Recommended adult doses for newer agents: terbinafine, 250 mg/day for 2 weeks; itraconazole, 200 mg twice daily for 1 week; fluconazole, 150 mg once weekly for 4 weeks

98
Onychomycosis (Tinea Unguium)
Onychomycosis encompasses both dermatophyte and non-dermatophyte nail infections Represents up to 30% of diagnosed superficial fungal infections Etiologic agents are: Epidermophyton, Microsporum, and Trichophyton fungi

99
Onychomycosis Four classic types:
1) distal subungual onychomycosis: primarily involves distal nail bed and hyponychium, with secondary involvement of underside of nail plate of fingernails and toenails
 distal subungual onychomycosis: primarily involves distal nail bed and hyponychium, with secondary involvement of underside of nail plate of fingernails and toenails.")
100
Onychomycosis caused by Trichophyton rubrum

101
Trichophyton mentagrophytes
2) white superficial onychomycosis (leukonychia trichophytica.) This is an invasion of the toenail plate on the surface of the nail It is produced by T.mentagrophytes, species of Cephalosporium and Aspergillus, and Fusarium oxysporum fungus
 white superficial onychomycosis (leukonychia trichophytica.) This is an invasion of the toenail plate on the surface of the nail. It is produced by T.mentagrophytes, species of Cephalosporium and Aspergillus, and Fusarium oxysporum fungus.")
102
Onychomycosis 3) Proximal subungual onychomycosis: involves the nail plate mainly from proximal nail fold It is produced by T. rubrum & T. megninii and may be an indication of HIV infection 4) Candida onychomycosis involves all the nail plate; it is due to Candida albicans and is seen in patients with chronic mucocuataneous candidiasis Associated paronychia Adjacent cuticle is pink, swollen, and tender Fingernails > toenails
 Candida onychomycosis involves all the nail plate; it is due to Candida albicans and is seen in patients with chronic mucocuataneous candidiasis. Associated paronychia. Adjacent cuticle is pink, swollen, and tender. Fingernails > toenails.")
103
Onychomycosis caused by Candida albicans in mucocutaneous candidiasis

104
Onychomycosis Onychomycosis caused by T. rubrum is usually a deep infection Disease usually starts at distal corner of nail and involves the junction of nail and its bed First a yellowish discoloration occurs, which may spread until entire nail is affected Beneath discoloration nail plate becomes loose from nail bed

105
Gradually entire nail becomes brittle and separated from its bed due to piling up of keratin subungually Nail may break off, leaving an undermined remnant that is black and yellow from dead nail and fungi that are present

106
B: Superficial white onychomycosis
A: Distal subungal, onychomycosis occurring simultaneously with superficial white onychomycosis B: Superficial white onychomycosis

107
Differential Allergic contact dermatitis Psoriasis Lichen planus
20 nail dystrophy Darier’s disease Reiter’s disease Norwegian scabies Non-dermatophyte onychomycosis

108
Treatment PO terbinafine, fluconazole, and itraconazole
Griseofulvin continued until nails are clinically normal Low success rates 15-30% for toenails and 50-70% for fingernails Griseofulvin does not tx nail disease caused by candida 3% Thymol in EtOH

110
Candidiasis Candida proliferates in both budding and mycelial forms in outer layers of the stratum corneum where horny cells are desquamating It does not attack hair, rarely involves nail, and is incapable of breaking up the stratum corneum It is largely an opportunisitic organism Moisture promotes its growth Lip corners Body folds

111
Diagnosis Demonstration of the pathogenic yeast C. albicans establishes the diagnosis Under microscope KOH prep may show spores and pseudomycelium Culture on Sabouraud’s glucose agar shows a growth of creamy, grayish, moist colonies in about 4 days In time colonies form small, root-like penetrations into agar

113
Mycelium and spores of Candida albicans

114
KOH mount from infant with thrush showing pseudohyphae and yeast forms
Candidiasis KOH mount from infant with thrush showing pseudohyphae and yeast forms

115
Topical Anti-candidal Agents
These include, but are not limited to: clotrimazole (Lotrimin, Mycelex), econazole (Spectazole), ketaconazole (Nizoral), miconazole (MonistatDerm Lotion, Micatin), oxiconazole (Oxistat), sulconazole (Exelderm), naftifine (Naftin), terconazole (vaginal candidiasis only), cicloprox olamine (Loprox), butenafine (Mentax), nystatin, and topical amphotericin B lotion Terbinafine has been reported to be less active against Candida species by some authors
, econazole (Spectazole), ketaconazole (Nizoral), miconazole (MonistatDerm Lotion, Micatin), oxiconazole (Oxistat), sulconazole (Exelderm), naftifine (Naftin), terconazole (vaginal candidiasis only), cicloprox olamine (Loprox), butenafine (Mentax), nystatin, and topical amphotericin B lotion. Terbinafine has been reported to be less active against Candida species by some authors.")
116
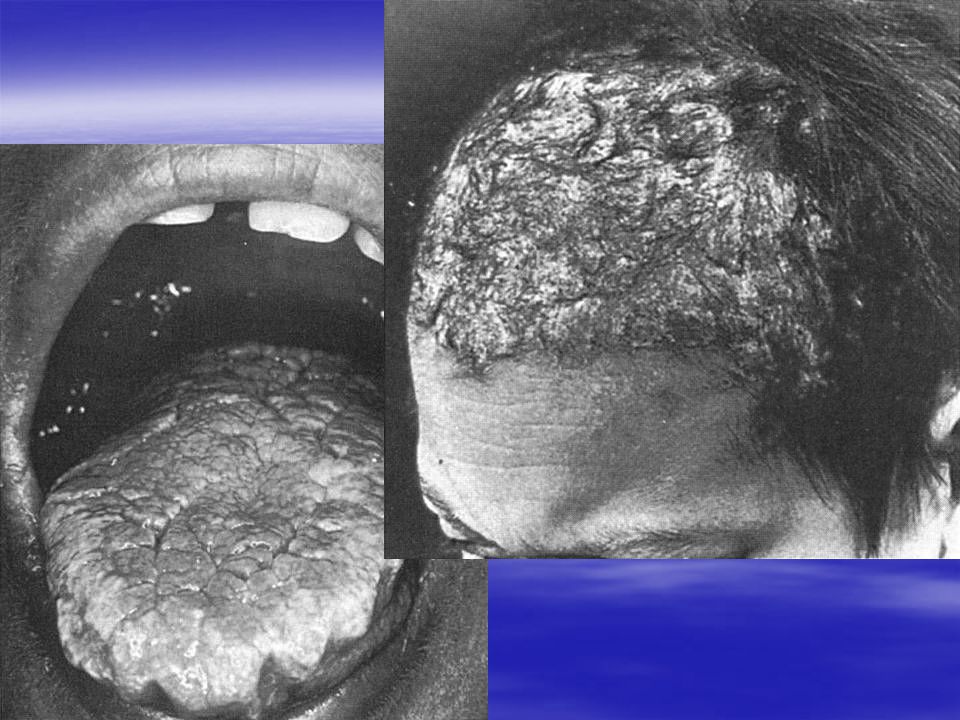
Oral Candidiasis (Thrush)
Newborn infection may be acquired from contact with vaginal tract of mother Grayish white membranous plaques are found on surface Base of plaques are moist, reddish, and macerated Diaper areas is especially susceptible to this Most of intertriginous areas and even exposed skin may be involved

117
Oral candidiasis (Thrush)
Frequently infection extends onto angles of the mouth to form perleche (seen in elderly, debilitated, and malnourished patients, and diabetics) It is often the first manifestation of AIDS Is present in nearly 100% of all untreated patients with full-blown AIDS “Thrush” in an adult with no known predisposing factors warrants a search for other evidence of infection with HIV, such as lymphadenopathy, leukopenia, or HIV antibodies in serum
 It is often the first manifestation of AIDS. Is present in nearly 100% of all untreated patients with full-blown AIDS. Thrush in an adult with no known predisposing factors warrants a search for other evidence of infection with HIV, such as lymphadenopathy, leukopenia, or HIV antibodies in serum.")
118
Thrush with extension to vermilion border

119
Treatment Babies with thrush may be allowed to suck on a clotrimazole suppository inserted into the slit tip of a pacifier four times a day for 2-3 days An adult can let tablets of clotrimazole or Mycelex troches dissolve in the mouth Fluconazole, mg/day for 5-10 days with doubling the dose if it fails, or Itraconazole, 200 mg daily for 5-10 days with doubling the dose if it fails-both are available in liquid forms

121
Perleche AKA angular cheilitis
Maceration with transverse fissuring of oral commissures Soft, pinhead-sized papules may appear Involvement is bilateral-usually

122
Perleche

123
Perleche Analogous to intertrigo elsewhere
Similar changes may be seen in riboflavin deficiency, and iron deficiency anemia Identical fissuring occurs in persons with malocclusion caused by ill-fitting dentures and in the aged whom atrophy of alveolar ridges has occurred Seen in children who drool, lick their lips, or suck their thumb

124
Treatment If due to C. albicans, anti-candidal creams and lotions can be used Glycemic control in diabetes Antibiotic topical meds are used when a bacterial; infection is present If due to vertical shortening of lower third of the face, dental or oral surgical intervention may help Injection of collagen into depressed sulcus at the oral commissure may be helpful Vytone!!

125
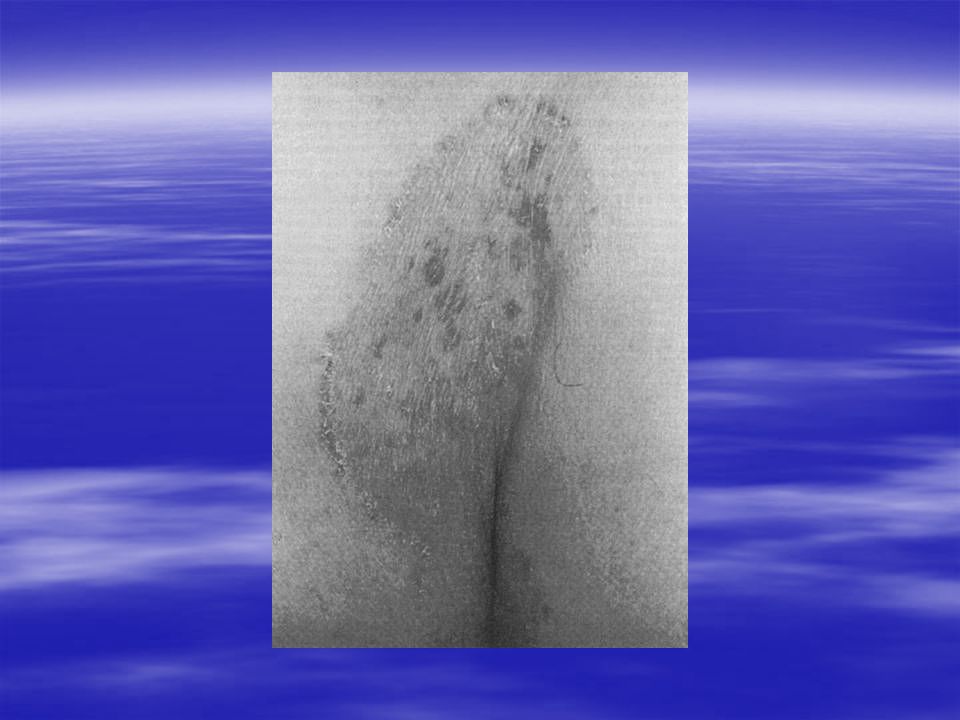
Candidal Vulvovaginitis
Pruritus, irritation, and extreme burning Labia may be erythemtous, moist, and macerated and cervix hyperemic, swollen, and eroded, showing small vesicles on its surface Vaginal discharge is not usually profuse but is frequently thick and tenacious May develop during pregnancy, in diabetes, or secondary to therapy with a broad- spectrum antibiotic Recurrent vulvovaginal candidiasis has been associated with long-term tamoxifen tx

126
Candidal Vulvovaginitis
Candidal balanitis may be present in an uncircumcised sexual partner If not recognized, repeated reinfection of a partner may occur Diagnosis is by clinical symptoms and findings as well as demonstration of fungus via KOH microscopic exam & culture Tx is frustrating & disappointing due to recurrences Oral fluconazole 150 mg times 1 dose; Fluconazole, 100mg/day for 5-7 days, itraconazole, 200 mg/day for 2-3 days are other options

128
Treatment Topical options include miconizole (Monistat cream), nystatin vaginal suppositories or tablets (Mycostatin), or clotrimazole (Gyne-Lotrimin or Mycelex G) vaginal tablets inserted once daily for 7 days
, nystatin vaginal suppositories or tablets (Mycostatin), or clotrimazole (Gyne-Lotrimin or Mycelex G) vaginal tablets inserted once daily for 7 days.")
129
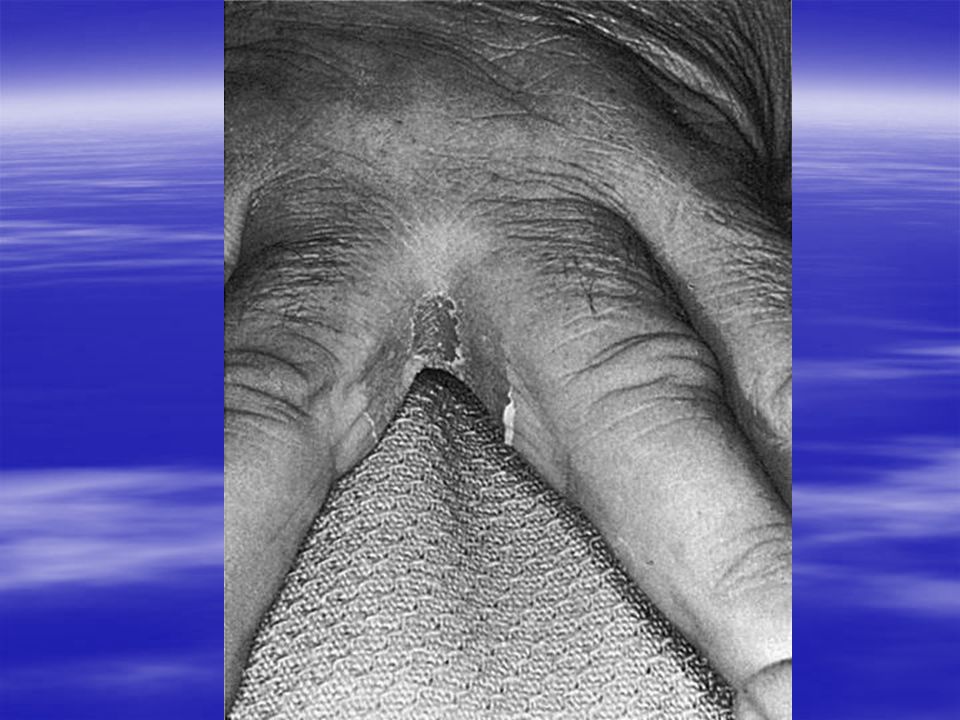
Candidal Intertrigo Pinkish intertriginous moist patches are surrounded by a thin, overhanging fringe of somewhat macerated epidermis (“collarette” scale) May resemble tinea cruris, but usually there is less scaliness and a greater tendency to fissuring Topical anti-candidal preparations are usually effective Recurrence is common
 May resemble tinea cruris, but usually there is less scaliness and a greater tendency to fissuring. Topical anti-candidal preparations are usually effective. Recurrence is common.")
131
Pseudo Diaper Rash In infants, C. albicans infection may start in perianal region and spread over entire area Dermatitis is enhanced by maceration produced by wet diapers Diaper friction may contribute to skin irritation and compromised function of stratum corneum Suspected by finding involvement of folds and occurrence of many small erythematous desquamating “satellite” or “daughter” lesions scattered around edges

132
Congenital Cutaneous Candidiasis
Infection of an infant during passage through birth canal Eruption usually noted within first few hrs of delivery Erythematous macules progress to thin-walled pustules, which rupture, dry, and desquamate within a week Lesions are usually widespread, involving trunk, neck, and head, at times palms and soles, including nail folds Oral cavity and diaper area are spared

133
Congenital Cutaneous Candidiasis
Differential dx: listeriosis, syphilis, staphylococcal and herpes infections, ETN, transient neonatal pustular melanosis, miliaria rubra , drug eruption, congenital icthyosiform erythroderma (neonatal pustular disorders) If suspected early amniotic fluid, placenta, and cord should be examined for evidence of infection Infants with disease limited to skin have favorable outcomes
 If suspected early amniotic fluid, placenta, and cord should be examined for evidence of infection. Infants with disease limited to skin have favorable outcomes.")
134
Congenital Cutaneous Candidiasis
Disseminated infection is suggested by (1) birth weight <1500g (2) evidence of respiratory distress or labs indicating neonatal sepsis (3) tx with broad-spectrum antibiotics (4) extensive instrumentation during delivery or invasive procedures in neonatal period (5) positive systemic cultures, or (6) evidence of an altered immune response Infants with congenital cutaneous candidiasis with any of these 6 criteria would be considered for systemic antifungal therapy
 birth weight <1500g (2) evidence of respiratory distress or labs indicating neonatal sepsis (3) tx with broad-spectrum antibiotics (4) extensive instrumentation during delivery or invasive procedures in neonatal period (5) positive systemic cultures, or (6) evidence of an altered immune response. Infants with congenital cutaneous candidiasis with any of these 6 criteria would be considered for systemic antifungal therapy.")
137
Perianal Candidiasis Frequently entire GI tract is involved
Can be precipitated by oral antibiotic therapy Perianal dermatitis with erythema, oozing, and maceration is present Psychogenic etiology is more common than is candidiasis Differential dx: psoriasis, seborrheic dermatitis, streptococcal and staphylococcal infections, contact dermatitis, and extramammary Paget’s disease Fungicides, meticulous cleansing of perianal region after bowel movements, topical corticosteroids and antipruritics (Atarax)
")
139
Candidal Paronychia Cushion-like thickening of paronychial tissue, slow erosion of lateral borders of nails, gradual thickening and brownish discoloration of nail plates, and development of pronounced transverse ridges Frequently only one nail A secondary mixed bacterial infection can occur with those who frequently have hands in water or who handle moist objects; cooks, dishwashers, bartenders, nurses, canners, etc

140
Candidal Paronychia Manicuring nails sometimes is responsible for mechanical or chemical injuries leading to infection Ingrown toenails with chronic paronychia Seen in pts with diabetes Avoid chronic moisture exposure; get diabetes under control Oral fluconazole once weekly or pulse dose itraconazole should be effective Topical therapy should continue for 2-3 months to prevent recurrence

141
Erosia Interdigitalis Blastomycetica
Oval-shaped area of macerated white skin on web between and extending onto sides of fingers With progression macerated skin peels off, leaving painful, raw,denuded area surrounded by a collar of overhanging white epidermis Nearly always affects third web Moisture beneath rings macerates skin and predisposes to infection Also seen in diabetics, those who do housework, launderers, and others exposed to macerating effects of water and strong alkalis

143
Chronic Mucocutaneous Candidiasis
A heterogeneous group of patients whose infection with Candida is chronic but superficial Onset before age 6 Onset in adult life may herald the occurrence of thymoma When inherited an endocrinopathy is often found Most cases have well-defined limited defects of cell-immunity Oral lesions are diffuse and perleche and lip fissures are common

146
Systemic Candidiasis High risk pts: pts with malignancies, AIDS, transplant pts requiring immunosuppressive drugs, pts on oral cortisone, pts who have had multiple surgical operations especially cardiac, pts with indwelling catheters, and heroin addicts Initial sign is varied: FUO, pulmonary infiltrates, GI bleeding, endocarditis, renal failure, meningitis, osteomyelitis, endophthalmitis, peritonitis, or a disseminated maculopapular eruption

147
Systemic Candidiasis Cutaneous findings are erythematous macules that become papular, pustular, and hemorrhagic, and may progress to necrotic, ulcerating lesions resembling ecthyma gangrenosum Deep abscesses may occur Trunk and extremities are usual sites of involvement Proximal muscle tenderness is a common finding

148
Systemic Candidiasis If candida is cultured within the first week of life there is a high rate of systemic disease There is a 50% chance of systemic disease if 1 or more cultures is positive Mortality has declined from 80% in the 1970’s to 40% in the 1990’s because of early empiric antifungals and better prophylaxis

149
THE END

Similar presentations
















>")






 can be both superficial and systemic. Superficial infections (Oral and vulvovaginal candidiasis, Dermatophytosis,>")










