Download presentation
Presentation is loading. Please wait.

1
Lower limb orthosis by Marwa abo el Hawa Assist. Lect. Rheum. & Rehab
Lower limb orthosis by Marwa abo el Hawa Assist. Lect. Rheum. & Rehab. Dep. Faculty of Medicine Tanta University

2
Def . Exoskeleton devices applied to lower body segments in pt. with neuromuscular or skeletal disorders to enhance normal movement and increase walking efficiency.

3
indication 1-Assist motion. 2-Correct flexible deformity.
3-Prevent progression of fixed deformity. 4- Stabilize gait. 5-Decrease pain. 6-Decrease energy expenditure. 7-Transferring weight.

4
Characters of device Simple Light Strong Durable
Cosmetically acceptable Low coast Temporarily [during recovery from injury or illness] Definitive [ with permanent disabilities]

5
BIOMECHANICAL PRINCIPLE
1-3 point pressure 2-Circumferential pressure 3-Axial unloading 4- Translation control 5- Serial correction 6- GRF( ground reaction force) control
 control.")
6
MATERIALS METALS PLASTIC
- Thermosetting (molded by heat –permanent figure -not return to consistency by reheating) - Thermoplastic ( soften when heated hardened when cooling - Types low temp & high temp ) LEATHER RUBBER Synthetic materials COMBINATIONS
 - Thermoplastic ( soften when heated hardened when cooling - Types low temp & high temp ) LEATHER. RUBBER. Synthetic materials. COMBINATIONS.")
7
Lower Extremity Orthosis:
FO foot orthosis AFO ankle foot orthosis KO knee orthosis KAFO knee ankle foot orthosis HKAFO hip knee ankle foot orthosis HO hip orthosis

8
STANDARD METAL DOUBLE UPRIGHT
SHOES STIRRUP UPRIGHTS ANKLE JOINTS KNEE JOINTS HIP JOINTS CALF BAND THIGH BAND PELVIC BAND

9
SHOES Function Characters - Protect foot - Warm foot
- Modified to transfer body weight during walking from sensitive area to pain free area Characters Comfortable Fit : correspond shape of foot proper room for foot expanding during wt bearing longer 1cm than longest toe

10
Arches of the Foot Foot has three important arches
Medial and lateral longitudinal arch Transverse arch Arches are maintained by: Interlocking shapes of tarsal Ligaments and tendons Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings 10

11
Arches of the Foot Figure 8.12 11
Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings 11

12
Bones of the Foot Figure 8.11b 12
Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings 12

13
Bones of the Foot Figure 8.11c 13
Copyright © 2005 Pearson Education, Inc., publishing as Benjamin Cummings 13

15
modifications A- medial longitudinal arch support - Deformity:
Pes planus , pes cavus ,pes valgus - Modification: Internal Steel shank(0.5 inch back to planter apex of calcaneus to 0.25 inch post to break of shoes) Cookie insert or insole ( rigid leather 1.25 inch behind heel breast line to 0.5 inch behind 1st metatarsal head) Navicular pad (scaphoid pad) as cookie insert but made of sponge material used when patient cannot tolerate rigid cookie insert Longitudinal arch support ( for broader area of support to shift body weight laterally) ( plastic ,metal, leather) Long counter (leather sandwiched between shoes layers form rigid wall medially to 0.5 inch forward to heel breast line
 Cookie insert or insole ( rigid leather 1.25 inch behind heel breast line to 0.5 inch behind 1st metatarsal head) Navicular pad (scaphoid pad) as cookie insert but made of sponge material used when patient cannot tolerate rigid cookie insert. Longitudinal arch support ( for broader area of support to shift body weight laterally) ( plastic ,metal, leather) Long counter (leather sandwiched between shoes layers form rigid wall medially to 0.5 inch forward to heel breast line.")
16
External Thomas heel ( orthopedic heel , key stone heel or s-shaped heel) anterior projection of medial breast line 0.5 inch Thomas heel wedge ,wedge sandwiched between base of Thomas heel &outsole Medial wedging (for medial arch support & shift body weight laterally) (height of wedging is height need to place calcaneus in near vertical position) Midway between medial breast line &break of shoes To front end of sole Tarsal & metatarsal Sole wedging Heel layer Talocalcaneal & talonavicular joint Heel wedging Severe valgus deformity Sole& heel wedging medial heel wedging& lateral sole wedging Flat feet Weak foot Cross wedging
 (height of wedging is height need to place calcaneus in near vertical position) Midway between medial breast line &break of shoes. To front end of sole. Tarsal & metatarsal. Sole wedging. Heel layer. Talocalcaneal & talonavicular joint. Heel wedging. Severe valgus deformity. Sole& heel wedging. medial heel wedging& lateral sole wedging. Flat feet. Weak foot. Cross wedging.")
17
Medial shank filler: from medial breast line to head of 1st metatarsal
Valgus strap: in spasticity & valgus contracture applied medially to prevent foot & ankle from assuming a valgus attitude B-Lateral longitudinal arch support Deformity: Pes varus, pes planus Modification: Internal Long counter laterally Lateral heel wedge insert External Reverse Thomas heel: anterior projection of lateral breast line 0.5 inch Lateral wedging: (heel, sole, sole &heel wedging) Medial shank filler: from Lateral breast line to head of 5th metatarsal
 Medial shank filler: from Lateral breast line to head of 5th metatarsal.")
18
Lateral flaring of shoes : to discourage varus deformity
Heel flaring, sole flaring (1.5 inch post to 5th metatarsal base to end of out sole), Heel &sole flaring . Varus strap : applied laterally C- Metatarsal arch support Indication: Bursitis,metatarsalgia ,fracture of metatarsal bone, planter warts, hallux valgus & hallux rigidus, Morton's toe (short 1st MT& phalanges or amputated ). Modification: Internal Metatarsal pad:( elevate inner sole just behind Metatarsal head) Dancer pad:( feathered edge under surface of Metatarsal head) Metatarsal corset:( removable arch support, above types with elastic strap over dorsum of foot) Levy inlay: wedge shaped pad made of foam or rubber placed between hallux & 2nd toe to realign 1st MTP joint Morton's toe extension: extend from heel to tip of toe supporting medial longitudinal arch to restore 3point wt distribution.
, Heel &sole flaring . Varus strap : applied laterally. C- Metatarsal arch support. Indication: Bursitis,metatarsalgia ,fracture of metatarsal bone, planter warts, hallux valgus & hallux rigidus, Morton s toe (short 1st MT& phalanges or amputated ). Modification: Internal. Metatarsal pad:( elevate inner sole just behind Metatarsal head) Dancer pad:( feathered edge under surface of Metatarsal head) Metatarsal corset:( removable arch support, above types with elastic strap over dorsum of foot) Levy inlay: wedge shaped pad made of foam or rubber placed between hallux & 2nd toe to realign 1st MTP joint. Morton s toe extension: extend from heel to tip of toe supporting medial longitudinal arch to restore 3point wt distribution.")
20
External Metatarsal bar: behind & parallel to line from 1st to 5th MT head, in out sole so after heel strike wt borne to behind Metatarsal head. Rocker bar: as Metatarsal bar but extend to toe end. Denver bar: directly beneath transverse arch of foot at tarsometatarsal joints NB: all above as same height of heel D-Heel modification Heel elevation: to compensate for fixed equinus deformity or any leg discrepancy of 1.5 to 3 cm (if > 3cm so elevate heel & sole) Heel cushion relief: soft pad may filled with compressible material placed under painful part of heel.
 Heel cushion relief: soft pad may filled with compressible material placed under painful part of heel.")
27
FO (foot orthosis) When foot cannot attain neutral, FO may shim the gap to that fixed position-Accommodative FO May help the foot attain a neutral position-Corrective FO Either may unload compromised tissue; or may provide total contact May be full custom or Off The Shelf (OTS)
")
28
HEEL CUP: rigid plastic insert, cover planter surface of heel ,extend post, med, lat up the side of heel, to prevent lateral calcaneal shift in flexible flat foot. SESAMOID INSERT:0.75 inch length insert ,under hallux to transfer pressure off the short 1st MT head onto its shaft. LONGITUDINAL ARCH SUPPORT: applied med or lat.

30
UCBL University of California at Berkeley Laboratory (UCBL)
Rigid plastic total contact design formed over cast of foot held in maximal manual correction. Hind foot / mid foot correction Heel cup extends proximal to inframalleolar area and distally to the metatarsal heads

31
STIRRUP SOLID SPLIT ROUND CALIPER
SOLID STIRRUP ATTATCHED WITH FOOT PLATE

32
UPRIGHTS site:1 to t.5 cm from skin in short leg brace end at level of calf band in long leg brace med1.5 inch below pubic tubercle& lat at lower end of GT METALS OR PLASTIC ROUNDED OR FLAT Single (post or lat) OR double (med &lat) Fixed or telescoping DISTALLY WITH ANKLE AND PROXIMALLY TO CUFF BAND
 OR. double (med &lat) Fixed or telescoping. DISTALLY WITH ANKLE. AND PROXIMALLY TO CUFF BAND.")
33
ANKLE JOINTS site: opposite to malleoli upwards from medial to lateral(just below med malleolus & 0.5 inch above tip of lat malleolus) 1- FREE MOTION 2-PLANTER FLEXION ANKLE STOP 3- DORSIFLEXION ANKLE STOP 4-LIMITED MOTION ANKLE STOP 5-DORSIFLEXION ASSISTSPRING JOINT(klenzak) 6-Fixed ankle joint
 6-Fixed ankle joint.")
35
CALF AND THIGH BAND LEATHER LEVEL calf 1-2 inch below fibular head
Lower thigh band 4inch from calf band upper thigh band 1.5 inch below ischium WIDE TO DISTRIBUTE FORCE CALF BAND WITH PLANTER FLEXION STOP INCREASE KNEE FLEXION MOMENT SO USED IN GENU RECURVATUM

36
KNEE JOINTS SINGLE OR POLYCENTRIC
LEVEL at anatomical knee joint 0.5 inch above tibial plateau SINGLE AXIS 1-FREE MOTION 2-OFFSET KNEE JOINT 3-DROP RING 4-SWISS LOCK 5-ADJUSTABLE KNEE LOCK (DIAL LOCK)
")
38
HIP JOINTS AND LOCKS opposite to GT
1- MOVING HIP JOINT 2- SINGLE AXIS 3- TWO POSITION LOCK 4- DOUBLE AXIS

39
PELVIC BAND site midway between iliac crest >
CONTROL ROTATION AND ADDUCTION 1-BILATERAL PELVIC BAND Ant: ASIS, Post: middle of sacrum In unilateral: from ASIS to PSIS 2-PELVIC GIRDLE 3-SILESIAN BELT

40
AFO (ankle foot orthosis)
Most common orthosis Metal bars Total Contact Floor reaction Unweighting Immobilizing Most AFO’s can be articulating or non-articulating

41
SMO Supra Maleolar Orthosis
Low profile design that crosses the ankle Less invasive trim lines than a standard AFO

42
Total Contact AFO’s provide intimate fit with total contact to provide better control light weight ( gms); more common today

43
Floor Reaction AFO- Uses floor reaction force through toe aspect of foot plate to prevent forward tibial progression & subsequent knee collapse; May be articulated

44
Unweighting AFO May be patella tendon bearing (PTB), specific weight bearing or total surface bearing, TSB (inverted cone with lace closure) to unweight the ankle foot using prosthetic principles
, specific weight bearing or total surface bearing, TSB (inverted cone with lace closure) to unweight the ankle foot using prosthetic principles.")
45
Immobilizing AFO Commonly used with a lower extremity deficiency when ankle immobilization is desired distal tibia/ fibula fracture foot bone fractures tendocalcaneus rupture Diabetic Foot (Charcot Foot)
")
46
Non-Articulating (Solid Ankle)
Articulated or Non-articulated May be designed for progressive increases or decreases in sagittal plane ROM and control An articulating option may be available in many designs of AFO’s Non-Articulating (Solid Ankle) Articulating
 Articulating.")
50
KO (knee orthosis) Useful for malalignment
genu varum, valgum, recurvatum, to protect knee structures from undue loading/stress may be preventative or corrective may be permanent treatment for repaired/compromised knee structures

51
Several Types of KO’s: Athletic KO- Non-articulated KO-
Custom or OTS KO-

52
Athletic KO- Preventative.
Controversial as short lever arms may not be sufficient to diminish realistic damaging forces. Proprioception thought to play a role.

53
non-articulated KO- usually for short term use
difficult to transfer with

54
Off-the-Shelf KO- Offers limited control of the knee.
Restricts gross motion

55
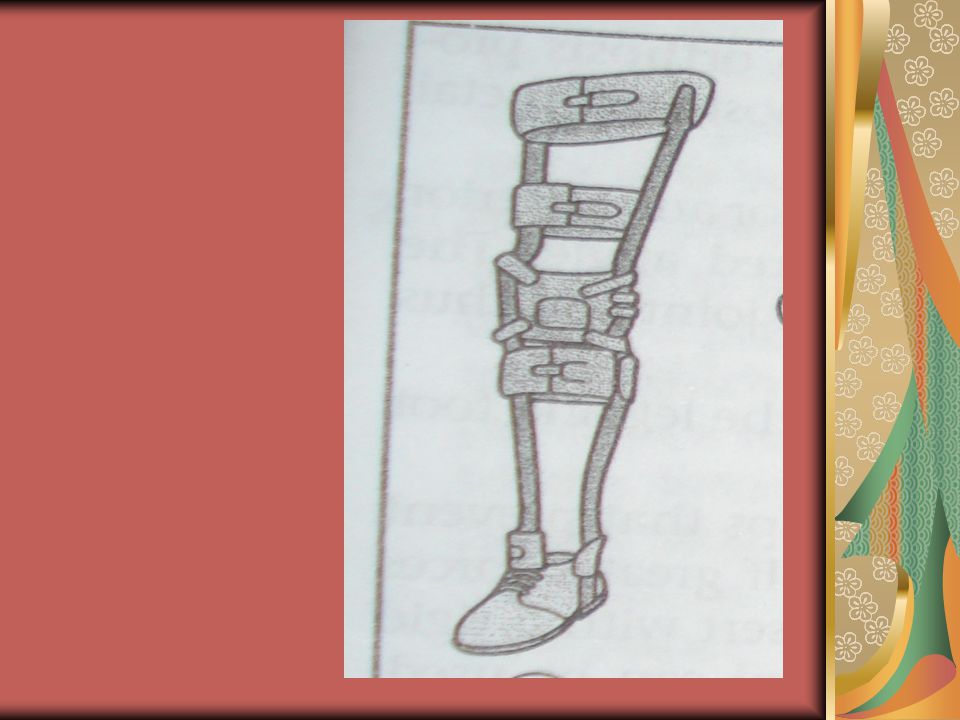
KAFO Knee Ankle Foot Orthosis
Indicated when lesser devices are biomechanical insufficient; Combines KO & AFO

56
Subtypes: Single/Double bar (upright) KAFO- Total contact KAFO-
Ischial Weight Bearing (unweighting) KAFO-
 KAFO-")
57
Single/Double Bar KAFO-
Accommodates volume fluctuation, Cooler than total contact, Highest material strength. Several lock options. Lock for ambulation, unlock for sitting. May incorporate hyperextension stops. Various knee joints are available e.g. Weight activated stance control, locking,

58
Total Contact KAFO- More customizable. Better load distribution.

59
Ischial Weight Bearing (unweighting) KAFO-
Ischial containment or Quadrilateral style brims with high trimlines. Generally used with paralytic limbs. Not as effective with larger or obese individuals.

60
HKAFO Hip Knee Ankle Foot Orthosis
Very restrictive and laborious to swing-to or through in gait causing high rejection rates Includes Reciprocating Gait Orthoses (RGO), total contact, leather and metal upright
, total contact, leather and metal upright.")
61
Specific HKAFO: Reciprocating Gait Orthosis (RGO)
Used in spinal cord injury. Combines flexion of one hip with extension of the opposite hip. The flexion power of one hip is utilized to extend the opposite hip.

62
Hip Abduction Orthosis
Commonly used post-operatively to position the femoral head optimally within the acetabulum Hip Abduction orthoses can be an HO only or can have a KAFO extension.

63
Specific Case Hip Orthosis (HO): S.W.A.S.H Orthosis
Standing Walking And Sitting Hip Orthosis Maintains femoral abduction in standing, walking and sitting

64
Thank you

Similar presentations














>")





>")










 (Lower) Leg Foot The lower appendages are attached to the axial skeleton via the pelvic girdle.>")
