Download presentation
Presentation is loading. Please wait.

2
In the beginning…….. Diabetic patients were losing limbs, long stays in hospital, no hope of healing chronic ulcers inevitable amputation. No light at the end of the tunnel, only destruction, dismay and death. …But a new era was emerging….

3
Historical Events Launch of Sky TV
Unleaded Petrol was at 38p per litre Inauguration of the 1st President Bush Order of the garter opened to women Terry Waite was kidnapped in Beirut First ever Rugby World Cup kicks off

4
Reduce Amputations by 50%
‘ Where are we – where do we want to be, and how can we get there’?

5
Scotchcast Boot

7
The Greater Team Podiatrist Specialist Care Patients Wards
District Nurses Practice Nurses G.P’s

8
100 boots in Blackburn – 1988 Showed average healing rates of 8 weeks in neuropathic ulceration BUT How do we prevent the first ulcer? How do we keep them healed?

9
Precipitating Factors of Ulcers
Historical Data 1988/1989 Precipitating Factors of Ulcers Kings (n=210) Blackburn (n=100) Shoes 85% 74% Accident 9% 14% Thermal 2% 3% Pressure 4%
 Blackburn. (n=100) Shoes. 85% 74% Accident. 9% 14% Thermal. 2% 3% Pressure. 4%")
12
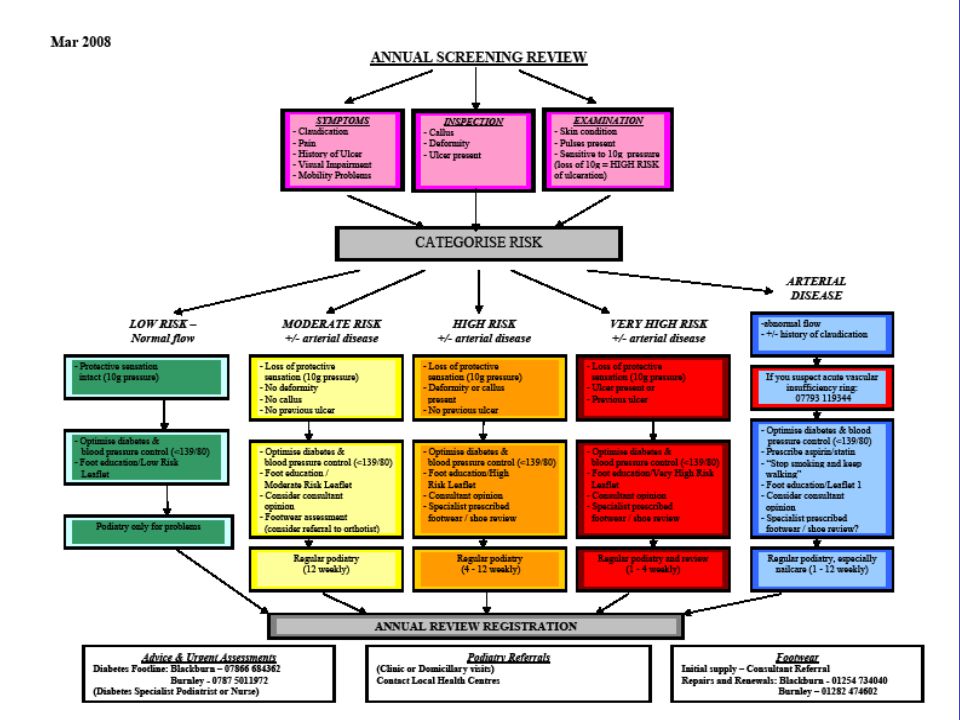
LOW RISK Optimise diabetes and blood pressure control (<139/80)
Protective sensation intact (10g pressure) Optimise diabetes and blood pressure control (<139/80) Foot education/Low risk leaflet Podiatry only for problems
 Optimise diabetes and blood pressure control (<139/80) Foot education/Low risk leaflet. Podiatry only for problems.")
13
MODERATE RISK Loss of protective sensation No deformity No callus
No previous ulcer Foot education/Moderate risk leaflet Consider Consultant opinion Optimise diabetes and blood pressure control (<139/80) Footwear advice and assessment Regular Podiatry (12 weekly)
 Footwear advice and assessment. Regular Podiatry (12 weekly)")
14
Regular Podiatry (4 – 12 weekly)
HIGH RISK Loss of protective sensation Deformity and/or callus present No previous ulcer Optimise diabetes and blood pressure control (<139/80) Foot education/High risk leaflet Consultant opinion Specialist prescribed Footwear/Shoe review Regular Podiatry (4 – 12 weekly)
 Foot education/High risk leaflet. Consultant opinion. Specialist prescribed Footwear/Shoe review. Regular Podiatry (4 – 12 weekly)")
15
Regular podiatry and review
Very High Risk Ulcer present or Previous ulcer Loss of protective sensation (10 g pressure) Foot education leaflets/ very high risk leaflet Consultant opinion Specialist prescribed footwear / shoe review Optimise diabetes & blood pressure control (<130/80) Regular podiatry and review (1-4 weekly)
 Foot education leaflets/ very high risk leaflet. Consultant opinion. Specialist prescribed footwear / shoe review. Optimise diabetes & blood pressure control (<130/80) Regular podiatry and review. (1-4 weekly)")
16
Regular Podiatry especially nail care (1-12 weekly)
Arterial Disease Abnormal flow +/- History of claudication telephone: If you suspect acute vascular insufficiency Optimise diabetes & blood pressure control (>139/80) Prescribe aspirin/statin ‘Stop smoking and keep walking’ Foot education/leaflet Consider consultant opinion Specialist prescribed footwear / shoe review Regular Podiatry especially nail care (1-12 weekly)
 Prescribe aspirin/statin. ‘Stop smoking and keep walking’ Foot education/leaflet. Consider consultant opinion. Specialist prescribed footwear / shoe review. Regular Podiatry especially nail care (1-12 weekly)")
17
Referral Pathways For The Diabetic Foot
Referral for Urgent Problems Referral for Non-urgent Problems Referral for Diabetic Footwear Urgent Patient Non Urgent Patient New patient Existing patient Referral letter, or fax ( ) Dr G.R. Jones, Diabetes unit, RBH Prescribed footwear Same Day Referral Letter of Referral to Dr G.R. Jones, Diabetes unit, RBH Continue treatment until Outpatient Appointment Ring :- Diabetes Hot Foot line Blackburn Burnley Orthotics RBH BGH Orthotics RBH BGH Condition becomes urgent refer via RED Pathway
 Dr G.R. Jones, Diabetes unit, RBH. Prescribed footwear. Same Day Referral. Letter of Referral to. Dr G.R. Jones, Diabetes unit, RBH. Continue treatment until Outpatient Appointment. Ring :- Diabetes Hot Foot line. Blackburn Burnley Orthotics. RBH BGH Orthotics. RBH BGH Condition becomes urgent refer via RED Pathway.")
18
N.I.C.E Guidelines recommend:-
Annual inspection and examination Aggressive intervention to reduce morbidity Primary and secondary care should work together to identify a package of care for at risk feet

19
N.I.C.E. ‘foot ulceration and lower limb amputation can be reduced if people who have sensory neuropathy affecting their feet are identified and offered regular podiatry and protective footwear if required’

20
Do Shoes and Orthoses work?
To look at the precipitating factors responsible for new DFU compared to previous studies. Are shoes still a major factor or have things changed? “Change is inevitable – except from a vending machine!” Robert C. Gallagher

21
Precipitating Factors of Referred Ulcers
Kings 1988 (n=210) Blackburn 1988 (n=100) Blackburn 2004 (n=72) Shoes 85% 74% 47.2% Accident 9% 14% 12.5% Thermal 2% 3% 4.2% Pressure 4% 15.3%
 Blackburn (n=100) Blackburn (n=72) Shoes. 85% 74% 47.2% Accident. 9% 14% 12.5% Thermal. 2% 3% 4.2% Pressure. 4% 15.3%")
22
Diabetic population and Ulcer Frequency
Outcomes Diabetic population and Ulcer Frequency

23
Aetiology of Foot Ulcers in Diabetic Foot Clinic

26
100 boots in Blackburn – 1988 Showed average healing rates of 8 weeks in neuropathic ulceration BUT How do we prevent the first ulcer? How do we keep them healed? 26

27
Stock footwear Bespoke footwear Diabetic specification Custom made insoles Modular footwear

28
(Orthotic & Podiatric)
Continuous follow-up (Orthotic & Podiatric) 2-3 servicable pairs of shoes Long term care (>2yrs) Weaning process Long term healing “A neuropathic patient is a footwear patient for life” (Ulbrect J 15/05/08)
 2-3 servicable pairs of shoes. Long term care (>2yrs) Weaning process. Long term healing. A neuropathic patient is a footwear patient for life (Ulbrect J 15/05/08)")
29
Footwear Follow-up Study
100 consecutive patients recalled after 2 years Then followed up for a further 7 years

30
Results 2 Years 5years 10Years Intact 70% 24% Cracked skin/callus 30%
23% 14% Ulceration 3% 22% Amputation 1 Major 3 Minor 7 Major 5 Minor

31
Conclusion from footwear follow-up study
Prescribed footwear is effective when worn, inspection is a vital part of follow up although this is written into guide lines it is not usually adhered to. The importance of footwear review needs more emphasis at all levels of care

32
That’s ok but is it cost effective?

33
G H Nuttall P/O BSc(hons) MBAPO
I am asked (told) to provide footwear for diabetic patients. 20% of my working week is dedicated to working within the East Lancashire Diabetic Foot Team. I am expected to provide orthosis that will prevent high risk feet from ulcerating & healed ulcerated feet from re-ulcerating. Ensure patients have TWO serviceable pairs of footwear.
 to provide footwear for diabetic patients. 20% of my working week is dedicated to working within the East Lancashire Diabetic Foot Team. I am expected to provide orthosis that will prevent high risk feet from ulcerating & healed ulcerated feet from re-ulcerating. Ensure patients have TWO serviceable pairs of footwear.")
34
Am I of value in treating feet ? (or am I just an expensive accessory?)
Effective? Efficient? Contribution? Cost effective?

35
Cost Savings by Orthotics
of £102,000 Cost saving of £147,000 Cost saving of £282,000 Cost saving of £392,000 30 39 66 88

36
Allied Health Professions input to the Diabetes pathway
The cost on the NHS to heal one ulcer is £3k to £7.5k. Should this progress to amputation the cost is estimated to escalate to £65k. This is much more than the cost of preventative orthoses. For every £1 spent in orthotics the NHS saves £4. Hutton and Hurry 2009, Orthotic Service in the NHS: Improving Service Provision. York Health Economics

40
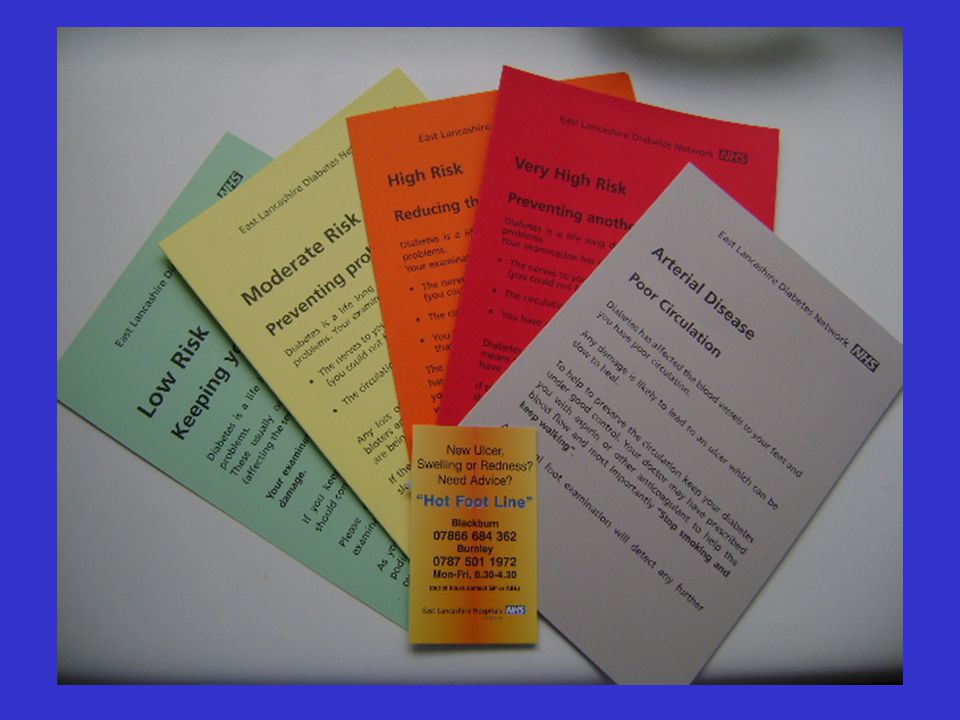
Ulceration/Hot Foot REFER patients to a multidisciplinary foot care team within 24 hours if any of the following occur: new ulceration (wound) new swelling new discolouration (redder, bluer, paler, blacker, over part or all of foot). (NICE Guideline – Type 2 diabetes: prevention and management of foot problems) REFER non-healing wounds from 0 – 4 weeks duration
 new swelling. new discolouration (redder, bluer, paler, blacker, over part or all of foot). (NICE Guideline – Type 2 diabetes: prevention and management of foot problems) REFER non-healing wounds from 0 – 4 weeks duration.")
41
Treatment of Ulceration
Pressure relief (preferably non removable) Medical management (CVS, oedema, diabetes, infection) Debridement and dressings And…….. a team
 Medical management (CVS, oedema, diabetes, infection) Debridement and dressings. And…….. a team.")
42
Pressure Relieving Devices
Aircast Walker DH shoe DARCO walker Padding & strapping Podo-med Half shoe

43
Nothing works like casting

44
Cast Variations Modified TCC Bi-valved cast Focused Rigidity Cast
Heel ulceration

45
Innovations from Diabetic foot Service
Scotchcast Boot Bespoke casting Screening Programme Effective and efficient orthotic service Hot foot line House shoe Charcot data and register

46
HOME? NOT SO SWEET HOME Lomax G McLaughlin C Jones G R Kenwright C
Blackburn Royal Infirmary

47
HOME? NOT SO SWEET HOME “THE GREATEST NUMBER OF STEPS PER DAY
ARE TAKEN IN THE PATIENTS OWN HOME.” David Armstrong et al. (American Podiatric Medicine 2001)
")
48
HOME? NOT SO SWEET HOME PRESCRIBED INSOLES AND FOOTWEAR CAN PREVENT FOOT PATHOLOGY (TOVEY F.I. 1987)
 .")
49
HOME? NOT SO SWEET HOME Footwear is most effective when worn for a minimum of 60% of the day. (Chanteleau, E. Haage, P.) Most effective when worn for 100% of the ambulatory time.

50
HOME? NOT SO SWEET HOME AIM OF STUDY
To assess what proportion of patients who had been prescribed Diabetic footwear were wearing at home.

51
How could we do this study?
HOME? NOT SO SWEET HOME How could we do this study? Ask patients at clinics? A telephone survey? Send patient questionnaires? Knock on patient doors and ask and look? Data collection by Community Podiatrists visiting patients homes on Domiciliary visits. “The sneak approach”

52
HOME? NOT SO SWEET HOME RESULTS
Question No shoes Own shoes Own slippers Prescribed shoes 1. What is patient wearing on entry to house? 19% 8% 52% 21% 2. What does patient apply after treatment? 15% 56%

53
HOME? NOT SO SWEET HOME CONCLUSION
75% of patients visited do not wear prescribed shoes at home. All health care professionals need to be aware of this.

54
“ HOME SAFE HOME”

55
Charcot Foot

56
Care of People with Charcot Osteoarthropathy (NICE 01/04)
“People with suspected or diagnosed Charcot osteoarthropathy should be referred immediately to a specialist multidisciplinary foot care team for immobilisation of the affected joint(s) and for long-term management of offloading to prevent ulceration.”
 and for long-term management of offloading to prevent ulceration.")
57
Definition ? No definitive “test”
Xrays & scans – open to interpretation Diagnosis is primarily clinical & subjective

58
Identification of Charcot Arthropathy
Unified district wide diabetic foot service Centralised referral point Validated district diabetes register

59
Charcot Data (1996-2006) Incidence and Prevalence
Patient Characteristics Diagnostic Presentation Treatment and Outcomes (including the effect of an audit and community education event in 2001)
")
60
Presenting Site Of Charcot Arthropathy
1st. 2nd. 3rd. Midfoot 32(71%) Ankle 9(20%) Forefoot 4(9%)
 Ankle 9(20%) Forefoot 4(9%)")
61
Presentation Charcot 10 (35%) delayed diagnosis on presentation
7 (24%) developed C.N.A on ipsilateral limb 3 (10%) developed C.N.A on contralateral limb. 9 (31%) diagnosed correctly
 developed C.N.A on ipsilateral limb. 3 (10%) developed C.N.A on contralateral limb. 9 (31%) diagnosed correctly.")
62
Local Charcot “Programme” (2001)
Why Delays in diagnosis/ Late Presentations How Education event in community for all HCPs What Road show – staff meetings, lunch hours, training events

63
Presentation

64
Treatment of Charcot Arthropathy
Mean time in casts 2001, weeks (8 - 56) , weeks (range ) (p<0.001) Mean time from active to quiescence 2001, weeks (8 -70) , weeks (range 8 – 40) 39 (87%) 4 (9%) 2 (4%)
 2006, 20.5 weeks (range ) (p<0.001) Mean time from active to quiescence. 2001, 42 weeks (8 -70) 2006, 26.3 weeks (range 8 – 40) 39 (87%) 4 (9%) 2 (4%)")
65
exostectomies and minor amputations
Outcomes n=45 No. of C.N.A Surgery - exostectomies and minor amputations Below Knee Amputation Deaths Healed/ Stable Feet 31 7 Feet with Ulcers 14 5+4 4 2

66
Mortality/Morbidity Charcot v Matched Controls
(p>0.05)
")
67
Summary Charcot Arthropathy IS uncommon (1:500 people with diabetes)
Diagnosis is often initially delayed, but community education and awareness significantly reduces this Poor diabetic control appears to be a prerequisite for CNA

68
Outcome for both limb and life is NOT adversely affected.
Conclusion Earlier recognition and treatment of C.N.A. translates into significantly faster healing & 3/12`s less time in casts! (Charcot “Road shows” work!) Our local surgical practice is conservative & reserved for feet with recurrent or non healing ulcers only Outcome for both limb and life is NOT adversely affected. Larger patient numbers are needed to be studied to ratify these findings and this will demand collaborative working e.g. CDUK
 Our local surgical practice is conservative & reserved for feet with recurrent or non healing ulcers only. Outcome for both limb and life is NOT adversely affected. Larger patient numbers are needed to be studied to ratify these findings and this will demand collaborative working e.g. CDUK.")
69
Grant from DUK The Charcot register
National data base Lead and managed from ELHT

70
The Charcot Register Scotland 6 North East 4 North West 10
Yorkshire & Humberside West Midlands 3 East Midlands Northern Ireland 1 Republic of Ireland 2 Wales East Anglia 5 South West South East 16 We’ve had centres registering patients from as far north as Aberdeen and as far south as Plymouth. The majority of centres have been in the south and north west. We’ve also had interest in the project from America, Argentina, Malta and Australia.

73
Finally Latest Benchmarking Data from the SHA
Lowest non-elective admission rates Shortest length of stay Effective and efficient service

74
Then & now Diabetic Foot Service 1988
People working in isolated pockets Foot clinic inaugurated MDT formed Inadequate referral pathways High amputation rates Long in patient stays Huge NHS costs NOW Foot clinic 23 years old Effective implemented pathways Well established clinics Good interagency and interprofessional relationships Low amputation rates Reduced in patient stay Cost efficient

76
Thank you

Similar presentations