Download presentation
Presentation is loading. Please wait.

1
Evaluating Running Injuries in Clinic
Jim Chesnutt, M.D. OHSU Sports Medicine Program OHSU Orthopaedics and Rehabilitation and Family Medicine

2
Common Running Injuries
Look at biomechanics of running Consider factors leading to overuse injury Identify common running injuries Learn treatment and prevention strategies

3
Biomechanics of Running
1000 steps per mile load is 2-3x body weight per stride running shoes absorb shock but need new shoes each miles shoes: cushion, support, traction biomechanical abnormalities translate forces up and down kinetic chain Pelvis-hip-knee-ankle-foot

4
Biomechanics of Running
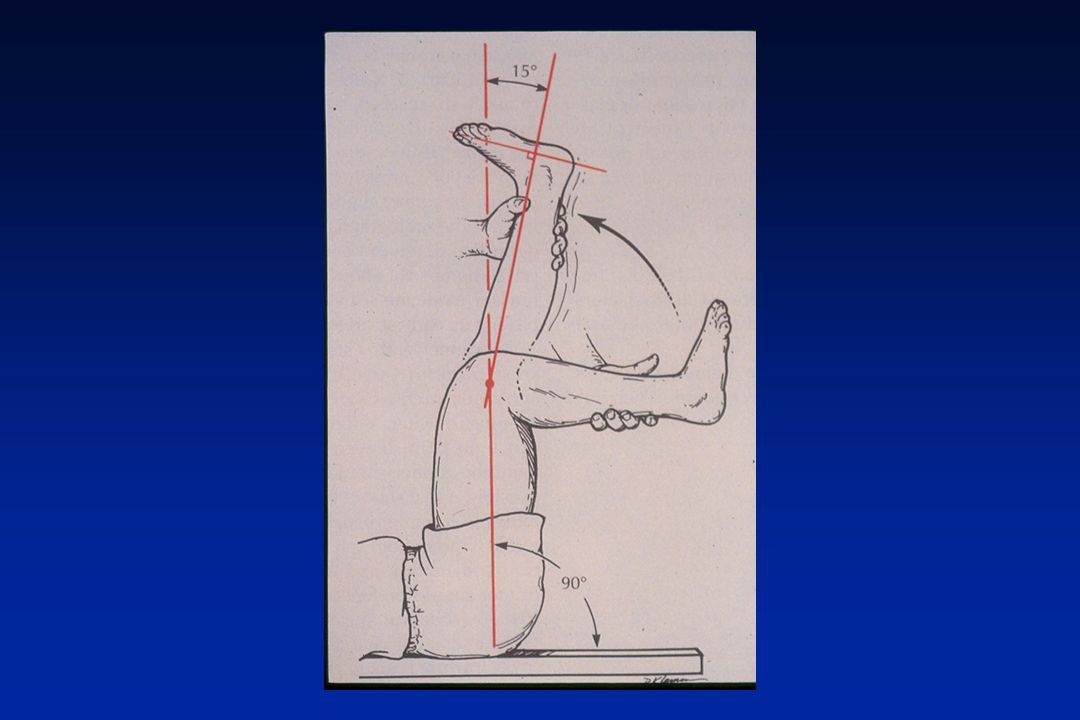
The Two Phases of Gait I. Support Phase- shock absorption 1. contact stage (25%) -hip extended, knee flexed, foot supinated 2. midstance stage (50%) -rapid pronation, shock absorption 3. take-off stage (25%) -supinated, rigid foot, contracted gastrocs II. Recovery Phase- airborne swing
 -hip extended, knee flexed, foot supinated. 2. midstance stage (50%) -rapid pronation, shock absorption. 3. take-off stage (25%) -supinated, rigid foot, contracted gastrocs. II. Recovery Phase- airborne swing.")
5
Common Overuse Syndromes
Mechanisms of Injury 1. repetitive motion/ stress 2. microtrauma 3. stress or trauma >> adaptation or repair 4. chronic or progressive pain and dysfxn or mechanical failure (macrotrauma) 5. phases of healing : I. inflammatory( 1-5 days) II. regeneration( days) III. remodeling( 14+ days)
 5. phases of healing : I. inflammatory( 1-5 days) II. regeneration( days) III. remodeling( 14+ days)")
6
Common Overuse Syndromes
Stages 1 : pain after activity only 2 : pain during activity but not affecting performance 3 : pain during activity causing restricted performance 4 : chronic pain, even at rest

7
Common Overuse Syndromes
Factors A. Intrinsic 1. Anatomical malalignment or defect - e.g. flat foot, osteoporosis 2. Biomechanical dysfxn - e.g. tibial torsion, over-pronation, inflexibility, muscle imbalance

8
Common Overuse Syndromes
Factors B. Extrinsic 1. Activity- related functional overload - e.g. improper technique and training errors ( too fast, too long, too many) 2. Poor equipment or environment - e.g. inadequate support or shock absorption or surface too hard
 2. Poor equipment or environment. - e.g. inadequate support or shock absorption or surface too hard.")
9
Overuse Injuries: 5 Step Treatment
Overuse Injuries: 5 Step Treatment (O’Connor FG et al, Phys and Sports Med 1992 ;21(7): ) Patho-anatomic Diagnosis (First step) A. Principle of Transition(Leadbetter) Hx: change in mode or use of involved part B. Principle of “victims ( injured site) and culprits(primary dysfunction)”(Macintyre) PE: biomechanical exam to find injury/cause
: ) Patho-anatomic Diagnosis (First step) A. Principle of Transition(Leadbetter) Hx: change in mode or use of involved part. B. Principle of victims ( injured site) and culprits(primary dysfunction) (Macintyre) PE: biomechanical exam to find injury/cause.")
10
Running Injuries Risks: 1) >40 miles/ wk 2) previous injury
3) >10% increase mileage per wk 4) foot, knee, and hip malalignment (hyper-pronation, weak hip flexor)
 >10% increase mileage per wk. 4) foot, knee, and hip malalignment. (hyper-pronation, weak hip flexor)")
11
Common Running Injuries
Most common: 1) Patellofemoral Pain Syndrome 2) Medial Tibial Stress Syndrome (“shin splints”) 3) Iliotibial Band Friction Syndrome 4) Plantar Fasciitis 5) Achilles’ Tendinitis
 Patellofemoral Pain Syndrome. 2) Medial Tibial Stress Syndrome. ( shin splints ) 3) Iliotibial Band Friction Syndrome. 4) Plantar Fasciitis. 5) Achilles’ Tendinitis.")
12
Common Running Injuries
6. Stress Fracture of Tibia 7. Stress Fracture of Femur 8. Exertional Compartment Syndrome 9. Female Athlete Triad 10. Iron Deficiency

13
Patellofemoral Pain Syndrome
Combination of various syndromes including patellar subluxation, pain and “chondromalacia” More common in females Classical anterior knee pain, crepitance, and occ. swelling as well as “positive theater sign”

14
Patellofemoral Pain Syndrome
Anatomical Predisposing Factors wide pelvis femoral anteversion tight hamstrings*** weak vastus medialis obliques( VMO)** weak hip flexor and abductors*** over-pronation of foot*** externally rotated tibia lateral tib tubercle (large “Q- angle”) lateral patella (subluxable)
** weak hip flexor and abductors*** over-pronation of foot*** externally rotated tibia. lateral tib tubercle (large Q- angle ) lateral patella (subluxable)")
15
Runner’s Exam Inspect fro atrophy/ effusion/red Squat double leg
Squat single leg Sitting extension Knee ligament meniscus exam Hamstring flexibility Ober’s Test: tight ITB or hip flexor Hip abduction resistance

21
Patellofemoral Pain Syndrome
Treatment modify activity ( less flexion stress) ice and NSAIDs (+/-) bracing or taping (+/-), chopat strap strengthen VMO and hip flexor/abductor stretch hamstrings orthotics surgery (rare)
 ice and NSAIDs (+/-) bracing or taping (+/-), chopat strap. strengthen VMO and hip flexor/abductor. stretch hamstrings. orthotics. surgery (rare)")
22
Iliotibial Band Syndrome
lateral knee pain during flexion( 30deg) worse with banked or downhill running over-pronation with int. tibial rotation ITB tightness--pos. Ober test*** RX: NSAIDs (1 wk) or steroid injection stretch, ice, friction rub, US fix pronation(orthotic) or hip mobility
 worse with banked or downhill running. over-pronation with int. tibial rotation. ITB tightness--pos. Ober test*** RX: NSAIDs (1 wk) or steroid injection. stretch, ice, friction rub, US. fix pronation(orthotic) or hip mobility.")
23
“Shin Splints” Exercise- related lower leg pain syndromes
Medial Tibial Stress Syndrome pain medial-posterior tibia diffusely soleus insertion periostitis plantar flexor and invertor x-ray: neg or diffuse periosteal reaction bone scan: diffuse late- phase only

24
Medial Tibial Stress Syndrome
Factors runner, hard surface, poor cushion poor conditioning, sudden increased intensity and duration ( > 10% per week) excessive and rapid pronation, tight Achilles
 excessive and rapid pronation, tight Achilles.")
25
Medial Tibial Stress Syndrome Treatment
relative rest (5-7d) ice massage NSAIDs Achilles stretch better shoes medial stabilizer cushioning not surgery
 ice massage. NSAIDs. Achilles stretch. better shoes. medial stabilizer. cushioning. not surgery.")
26
Lateral Tibial Periostitis
pain lat-ant tibia diffusely tibialis anterior insertion dorsiflexor, evertor x-ray/ bone scan : same factors: tight Achilles*** increased hills/dorsiflexion Rx: same

27
Exertional Compartment Syndrome
pain increases with activity resolves after rest, not immediate no bone pain muscle herniation is diagnostic elevated compartment pressure(>30mm hg) anterior % deep posterior 20-30% all others 20% factors: non-traumatic, unknown Rx: fasciotomy or limit activity
 anterior 50-60% deep posterior 20-30% all others 20% factors: non-traumatic, unknown. Rx: fasciotomy or limit activity.")
28
Nerve and Vascular Entrapment
Peroneal Nerve Lateral post knee pain Lateral calf / foot pain and numbness Peroneal weakness and foot drop Posterior Tibial Artery Compressed in the popliteal region May be positional May cause pain and numbness

29
Tibial Stress Fracture
focal tibial pain (esp with 3 pt bending) medial or lateral (different types) bending force from muscle tension tension: ant-lat, mid compression: post-med, distal/ prox pain despite rest/ treatment for 2 wks
 medial or lateral (different types) bending force from muscle tension. tension: ant-lat, mid. compression: post-med, distal/ prox. pain despite rest/ treatment for 2 wks.")
30
Tibial Stress Fracture
xray: medial: focal periosteal thickening (post-med) lateral: “dreaded black line” fracture (ant-lat) bone scan: focal uptake( all phases) positive 3-5d post pain increase key study to diagnose
 lateral: dreaded black line fracture (ant-lat) bone scan: focal uptake( all phases) positive 3-5d post pain increase. key study to diagnose.")
31
Imaging in Stress Fracture
bone scan: ( $500) focal uptake( all phases) positive 3-5d post pain increase key study to diagnose Sensitive but not specific MRI: ( $1500+) Early-( 1-3 days) focal T2 increase signal in area of edema in marrow and bone Later- low T1 signal indicates feacture line Sensitive and specific and anatomic detail
 focal uptake( all phases) positive 3-5d post pain increase. key study to diagnose. Sensitive but not specific. MRI: ( $1500+) Early-( 1-3 days) focal T2 increase signal in area of edema in marrow and bone. Later- low T1 signal indicates feacture line. Sensitive and specific and anatomic detail.")
32
Tibial Stress Fracture
Factors hard surface, poor shoes anatomical malalignment foot pronation leg length, rotation, or hip problem abrupt training increase osteoporosis jumping sports (esp ant-lat tibia fx )
")
33
Tibial Stress Fracture
Ant-lateral: caution!! higher rate nonunion 20% to full fx average 1 yr off sport consider bone stimulator, IM rod Medial: more common heals with 4-6 wks rest, slow progress **Often bilateral and recurrent**

34
Tibial Stress Fracture
Treatment improve shock absorbing or reduce stress - shoes , surface, rest, modified activity long air casts orthotic augment bone healing No NSAIDs calcium 1200 mg/day estrogen status/eating disorder/ osteoporosis

35
Orthotics Have been shown to treat 75% of injured runners successfully
Mechanism: limitation of abnormal pronation and subtalar motion Off -the -shelf models can be as effective, less costly as custom

36
Stress Fractures Incidence: track( 13-52%)- tibia, navic
ballet( 22-45%)- MT, fibula Most common sites: tibia( 30-50%), fibula, metatarsal, femur, tarsal (navicular). Female > male by 3-10x High risk in amenorrhea, high mileage 37% of college women, 50% amenorrheic - Female Athlete Triad -anorexia, amenorrhea, osteoporosis
- MT, fibula. Most common sites: tibia( 30-50%), fibula, metatarsal, femur, tarsal (navicular). Female > male by 3-10x. High risk in amenorrhea, high mileage. 37% of college women, 50% amenorrheic. - Female Athlete Triad. -anorexia, amenorrhea, osteoporosis.")
37
Female Athlete Triad Low energy balance/ Eating disorder Amenorhea
Overtraining Undereating of calories Amenorhea Fewer that 4 menstrual periods/ yr Osteoporosis

38
Low Iron: Runners Anemia
Runners consume more iron that general public Low iron effects performance Screen females/?men with ferritin Level above is probably best Iron is best taken as food items: meats, fish, legumes, greens, tofu, eggs ,nuts, dried fruits Supplement if low: caution for overload

39
High Risk Stress Fractures
Femoral neck Anterior cortex tibia Tarsal navicular Base of 5th metatarsal -Often delay in diagnosis -Poor outcomes if not treated with proper immolization and non-wt bearing

40
Femoral Neck Stress Fractures
Vague anterior thigh or groin pain Pain with extreme IR/ER or hopping on leg Average 3 month delay in diagnosis, AVN risk Lateral -superior, tension side -- serious Medial, compression---less serious MRI superior to bone scan 1: edema only 2: fracture line less than 50% 3: fracture line > 50%

41
Femoral Neck Stress Fractures
Non-wt bearing until asymptomatic Usually 4-8 weeks initially Progressive functional rehabilitation Re image if not progressing as expected Refer to orthopaedic surgeon if fracture line is >50% to consider immediate pinning

42
Stress Fractures Healing- average 3-6 weeks
2 wks: metatarsal and fibula 6-8 wks: most other bones 4+ months: anterior tibia, navicular, Jones fx Localized SF heals 2x rate of complete SF Recurrence: 50% overall (13% at 1yr)
")
43
Plantar Fasciitis most common cause of heal pain
medial calcaneal tubercle, origin of central band of plantar fascia painful first step of the morning relieved with exercise, pain resting no pain with lateral compression xray rarely useful, spur irrelevant

44
Plantar Fasciitis Factors excess pronation or high, rigid arch
women > men overweight and/or overtraining poor arch support or cushion tight heel cords

45
Plantar Fasciitis Treatment modify activity and weight
orthotics, arch support, or heel cups ice and NSAIDs stretch Achilles and calves cortisone shot (caution fat pad atrophy) nite splints (83% effective if used right)
 nite splints (83% effective if used right)")
46
Achilles Tendinitis 15% of all running injuries mostly males
Achilles takes highest force in the body- up to 8x body wt , running combined gastrocs and soleus occurs 2-6 cm above calcaneus at site of low blood flow usually tendinosis when chronic

47
Achilles Tendinitis Factors 1. poor body mechanics
- poor flexibility or alignment 2. training errors 3. environmental factors 4. athletic shoes

48
Achilles Tendinitis Treatment Physical therapy
specialized stretch program ice and/or ultrasound NSAIDs but no cortisone injections Orthotics and initial heel lift Surgery- 90% to full activity and 75% to high level

49
Running Shoe Prescription
Evaluate shoe wear pattern and foot type Rigid foot Normal foot Floppy Foot Shoe type

50
Running Shoes Rigid foot: lateral tilt and wear Cushion shoe
Normal foot: lateral heal strike with minimal excess motion Stability shoes Floppy foot: rolls to midline with wt bearing; medial tilt and wear pattern Motion control shoe, anti-pronation Goal: Happy Feet = Happy Runner

51
References Asplund C, Brown D. The Running Shoe Presciption. The Phys and Sportsmed. Vol. 33 (1), Jan 2005. Cole C, Seto C, Gazewood J. Plantar Fasciitis: Evidenced-Based Review of Diagnosis and Therapy. Am Fam Phys. , Vol 72 ( 11), Dec 2005. Hreljac A. Impact and Overuse Injuries in Runners. Med Sc in Sports & Exercise. Vol 36 (5), 2004. Hurwitz S. Athletic Foot and Ankle Injuries. Clinics in Sports Medicine. Vol 23 (1), Jan 2004.
, Dec Hreljac A. Impact and Overuse Injuries in Runners. Med Sc in Sports & Exercise. Vol 36 (5), Hurwitz S. Athletic Foot and Ankle Injuries. Clinics in Sports Medicine. Vol 23 (1), Jan")
52
References Kennedy J, et al. Foot and ankle injuries in the adolescent runner. Current Opinion in Pediatrics. Vol 17,2005. Lun V, Meeuwisse WH, et al. Relation between running injury and static lower limb alignment in recreational runners. Br. J. Sports Med. Vol 38, 2004. Mellion M,et al. The Team Physician’s Handbook, 2nd ed. Hanley and Belfus Niemuth P et al. Hip Muscle Weakness and Overuse Injuries in Recreational Runners. Clin J Sports Med. Vol 15 (1), Jan 2005.
, Jan")
Similar presentations