Download presentation
Presentation is loading. Please wait.

1
Staff and Patient Radiation Protection In The Cath Lab
Andrés Sinisterra Assistant Radiation Safety Officer for Medicine

2
Radiation vs. Radioactivity
Energy in transit in the form of high speed particles and electromagnetic waves. Ionizing Radiation Radiation with enough energy so that during an interaction with an atom, it can remove tightly bound electrons from their orbits, causing the atom to become charged or ionized. Radioactivity Spontaneous transformation of an unstable atom and often results in the emission of radiation. This process is referred to as a transformation, a decay or a disintegration of an atom.

3
External vs. Internal Radiation Exposure
External Exposure – X-rays, Diagnostic Procedures. Internal Deposition – Contamination from nuclear medicine patient undergoing a diagnostic or therapeutic procedure resulting in an ingestion of radioactive materials by the staff. + = T E D E

4
Units of Radiation Exposure
Roentgen Measure of electrical charge produced in air 1,000 mr = 1R SSD ~3-10 R/min Measure of energy absorbed, usually in tissue or bone. 200 rad = transient erythema 1 Gray = 100 Rad Rad (Gray)
")
5
Units of Radiation Exposure
Rem (Sievert) Measure of occupational risk (cancer) from radiation exposure 1,000 mrem = 1 Rem 1 Sievert = 100 Rem 1 R = 1 Rad = 1 Rem
 Measure of occupational risk (cancer) from radiation exposure. 1,000 mrem = 1 Rem. 1 Sievert = 100 Rem. 1 R = 1 Rad = 1 Rem.")
6
A wave is a wave & nothing but a wave!

8
X-RAY SOURCE ROTOR ROTATING ANODE FILAMENT TARGET CATHODE TUBE WINDOW
EVACUATED GLASS TUBE

11
Image Quality Vs Exposure

12
Area of Interest Collimation
Calcification of the vas deferens. These bilateral asymmetric calcifications occur in the lower to middle portion of the male pelvis

15
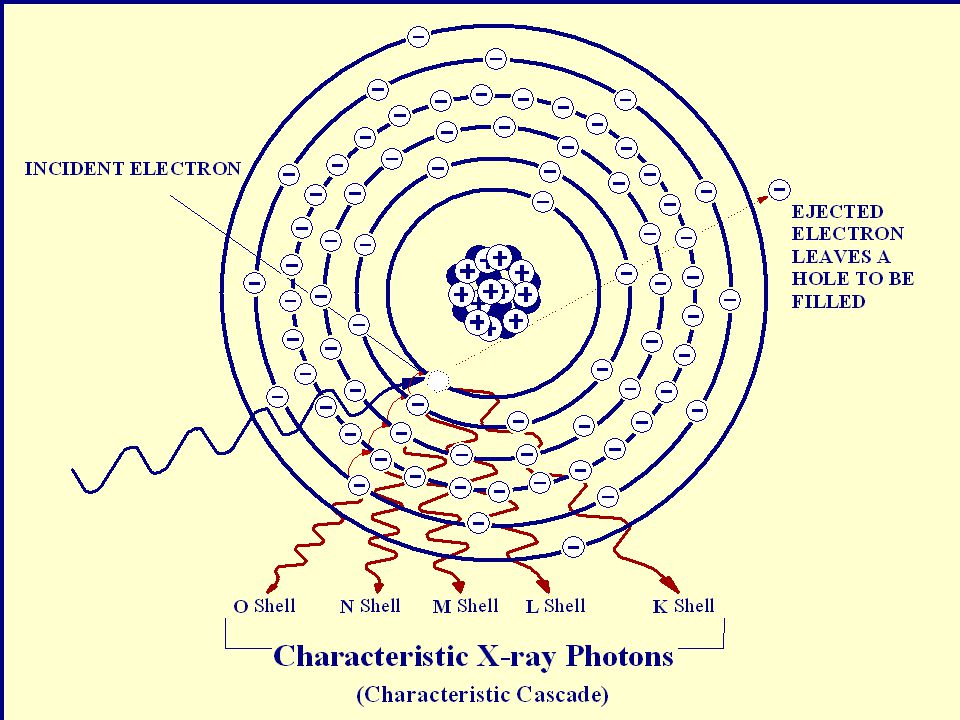
INCIDENT X-RAY PHOTOELECTRON Photoelectric effect occurs when an incident x-ray is totally absorbed during the ionization of the inner-shell electron. The incident photon disappears and the k-shell electron, now called a photoelectron, is ejected from the atom.

18
Primary Beam Scatter Radiation Leakage Radiation X-Ray Tube

19
Know Where Your Head Is At……!!!
Caudal

20
Coronal

22
Maximum Scatter plus Leakage
Minimum Scatter

23
Be aware of critically exposed areas
Head and shoulders knees and toes !!!!!

24
30-cm FOV Image intensifier 70-cm SSD Medium conventional fluoroscopy Setting C for fluorography Floor kVp is 110 Dose = 50 rad 55-cm SSD Medium conventional fluoroscopy Setting C for fluorography Floor kVp is 80 Dose = 140 rad 15-cm air gap Pail of water 28-cm deep 23-cm FOV Image intensifier The effects of an air gap are significant, even if the image is properly collimated Pail of water 28-cm deep

25
Know Where Your Head Is At……!!!
The greater the distance the greater the scatter

26
Mag Mode (Field-Of-View)
The following Table illustrates the effect of changing Field-Of-View, or magnification modes, for a typical fluoroscopy system Mag Mode (Field-Of-View) ESE (R/min) Increase Factor Normal (9 inch) 1.2 1.0 Mag 1 (6 inch) 2.9 2.4 Mag 2 (4.5 inch) 5.2 4.3
 ESE (R/min) Increase Factor. Normal (9 inch) Mag 1 (6 inch) Mag 2 (4.5 inch)")
27
Inverse Square Law (X-Rays & Gamma Rays)
For a point source, the intensity varies inversely as the square of the distance from the source. Scattered X-rays X-Ray Tube 1 cm 10,000 2 cm 2,500 5 cm 400 10 cm 100 20 cm 25 Leakage Radiation

28
Basic Radiation Safety Principles
Time Distance Shielding Contamination Control

29
Radiation Exposure and Monitoring
Whole Body Radiation Badge Worn Underneath Pb Apron Collar Radiation Badge Worn Outside Pb Apron At Neck Level BLACK ICON RED ICON Extremity Radiation Badge Worn on Primary Hand Closest to Radiation Source

30
Whole Body Radiation Badge Collar Radiation Badge
Worn Underneath Pb Apron Collar Radiation Badge Worn Outside Pb Apron At Neck Level

31
So what’s the big deal where I put my &#@% badges ?
D’OH ! At Thyroid ~45 cm At Breast ~30 cm

32
Get The Lead Out but Watch Your Back !!
PROTECTIVE EQUIPMENT Get The Lead Out but Watch Your Back !!

33
As Low As Reasonably Achievable
ALARA Level I > 10% of the maximum quarterly exposure limit (125 mrem) ALARA Level II > 30% of the maximum quarterly exposure limit (375 mrem)
 ALARA Level II. > 30% of the maximum quarterly exposure limit (375 mrem)")
34
ALARA Investigational Level I

36
Reducing Patient Dose During Fluoroscopy (And Yours)
Get off the pedal!! – Fluoro intermittently Collimate and only expose clinical area Use larger fields when possible (Magnification increases patient dose) Use distance of at least 30 cm for mobile units and 38 cm for fixed installations Use appropriate mA and KVp
 Use distance of at least 30 cm for mobile units and 38 cm for fixed installations. Use appropriate mA and KVp.")
37
Reducing Patient Dose During Fluoroscopy (And Yours)
Remember the egg timer!!! Be aware of the 5 minute timer (especially in high level mode) Have sufficient beam filtration > 90 KVp requires 2.5 mm Al to 3.5 mm 130 KVp Fluoro only when necessary Schedule annual QA of equipment
 Have sufficient beam filtration. > 90 KVp requires 2.5 mm Al to 3.5 mm 130 KVp. Fluoro only when necessary. Schedule annual QA of equipment.")
38
Radiation Dose The amount of energy deposited in any substance by ionizing radiation per unit mass of the substance. It is expressed numerically in rads (traditional units) or grays (SI units). Absorbed Dose Dose Equivalent Deep Dose Equivalent Eye Dose Equivalent Shallow Dose Equivalent Effective Dose Equivalent Committed Dose Equivalent Total Effective Dose Equivalent
 or grays (SI units). Absorbed Dose. Dose Equivalent. Deep Dose Equivalent. Eye Dose Equivalent. Shallow Dose Equivalent. Effective Dose Equivalent. Committed Dose Equivalent. Total Effective Dose Equivalent.")
39
Radiation Dose Absorbed Dose - The amount of energy deposited in any substance by ionizing radiation per unit mass of the substance. It is expressed numerically in rads (traditional units) or grays (SI units). Dose Equivalent - The dose equivalent (H) is the product of the absorbed dose in tissue, the quality factor and all other modifying factors at the location of interest. The unit is the rem (R) or the sievert (Sv).
 or grays (SI units). Dose Equivalent - The dose equivalent (H) is the product of the absorbed dose in tissue, the quality factor and all other modifying factors at the location of interest. The unit is the rem (R) or the sievert (Sv).")
40
Radiation Dose Deep Dose Equivalent (Hd) - Applies to external whole body exposure, means the dose equivalent at a tissue depth of 1 cm or greater. Eye Dose Equivalent - The external dose equivalent to the lens of the eye at a tissue depth of 0.3 cm. Shallow Dose Equivalent (Hg) - Applies to the external exposure of the skin or extremity. The dose equivalent at a tissue depth of cm averaged over an area of 1 cm2.
 - Applies to the external exposure of the skin or extremity. The dose equivalent at a tissue depth of cm averaged over an area of 1 cm2.")
41
Radiation Dose Committed Dose Equivalent (HE.50) - The dose equivalent (H) is a given organ or tissue that will be accumulated over 50 years following a single intake of radioactive material. Effective Dose Equivalent (HE) - The sum of the products of the dose equivalent (HT) to each organ or tissue and the weighting factor (WT) applicable to each of the body organs or tissues that are irradiated (HE = ‡” WTHT). Total Effective Dose Equivalent - The sum of the deep dose equivalent for external exposures and the committed effective dose equivalent for internal exposures.
 - The dose equivalent (H) is a given organ or tissue that will be accumulated over 50 years following a single intake of radioactive material. Effective Dose Equivalent (HE) - The sum of the products of the dose equivalent (HT) to each organ or tissue and the weighting factor (WT) applicable to each of the body organs or tissues that are irradiated (HE = ‡ WTHT). Total Effective Dose Equivalent - The sum of the deep dose equivalent for external exposures and the committed effective dose equivalent for internal exposures.")
42
Radiation Exposure Limits
(State of Connecticut Administrative Regulations Sect ) Type of Exposure Rem Per Calendar Quarter Whole body; head and trunk; active blood-forming organs; lens of eyes, or gonads. Hands and forearms; feet and ankles. Skin of whole body. 1.25 18.75 7.5 (1,250 mrem) (5.0 rem/yr) (18,750 mrem) (75 rem/yr) (7,500 mrem) (30 rem/yr) Fetus 500 mrem Total Gestation (0.5 rem)
 Type of Exposure. Rem Per Calendar Quarter. Whole body; head and trunk; active blood-forming organs; lens of eyes, or gonads. Hands and forearms; feet and ankles. Skin of whole body (1,250 mrem) (5.0 rem/yr) (18,750 mrem) (75 rem/yr) (7,500 mrem) (30 rem/yr) Fetus. 500 mrem Total Gestation. (0.5 rem)")
43
Radiation Exposure Limits
(USNRC 10CFR20 - § ) Type of Exposure Rem Per Calendar Year The total effective dose equivalent. 5.0 (0.05 Sv) The sum of the deep-dose equivalent and the committed dose equivalent to any individual organ or tissue other than the lens of the eye 50 (0.5 Sv)
 Type of Exposure. Rem Per Calendar Year. The total effective dose equivalent (0.05 Sv) The sum of the deep-dose equivalent. and the committed dose equivalent to. any individual organ or tissue other. than the lens of the eye. 50. (0.5 Sv)")
44
Radiation Exposure Limits
(USNRC 10CFR20 - § ) Type of Exposure Rem Per Calendar Year An eye dose equivalent and A shallow dose equivalent to the skin or to any extremity. 15 rem ( 0.15 Sv ) 50 rem ( 0.50 Sv ) In Utero exposure to the Fetus 0.5 rem Total Gestation (500 mrem & <50/mo)
 Type of Exposure. Rem Per Calendar Year. An eye dose equivalent. and A shallow dose equivalent to the skin or to any extremity. 15 rem ( 0.15 Sv ) 50 rem ( 0.50 Sv ) In Utero exposure to the Fetus. 0.5 rem Total Gestation. (500 mrem & <50/mo)")
45
Conditions For Exceeding Quarterly Doses To Whole Body
Total Dose For Any Quarter < 3.0 rem Total Whole Body Dose <= 5 (N-18) rem All Previous Whole Body Doses Plus N = Your Age In Years Prior Dose Must Be On a Clear Record ! ! ! ! ALARA PROGRAM EXISTS ! ! ! !
 rem. All Previous Whole Body Doses. Plus. N = Your Age In Years. Prior Dose Must Be On a Clear Record. ! ! ! ! ALARA PROGRAM EXISTS ! ! ! !")
46
Confidential Declaration of Pregnancy
NRC requires a signed declaration of pregnancy for occupational workers to limit exposures to 500 mrem/9months or 50 mrem in any one month.

47
A question of risk

48
Radiation Exposures From ?
Smoking a pack and a half of cigarettes a day will add about 1,300 mrem/year to one's effective dose Flying from New York to London results in the absorption of an extra 2-3 mrem of cosmic radiation 6-8 mrem from NY to Japan

49
Risks which Increase Chance of Death by 1 in 1 million a
a B.L. Cohen and I.S. Lee, “Catalog of Risks Extended and Updated”, Health Physics, Vol. 61, Sept

50
Estimated Loss of Life Expectancy from Health Risks
Health Risk Average Days of Life Expectancy Lost Smoking 20 cigarettes/day (6.5 years) Overweight (by 20%) (2.7 years) All accidents combined (1.2 years) Auto accidents Alcohol consumption Home accidents Drowning Natural background radiation 8 Medical diagnostic x-rays 6 All catastrophes (fire, flood, etc.) 3.5 1,000 mrem (1 rem) occupational radiation dose 1 1,000 mrem (1 rem)/yr for 30 years 30 Note: Average U.S. occupational radiation dose is estimated at rem/year.
 Overweight (by 20%) 985 (2.7 years) All accidents combined 435 (1.2 years) Auto accidents 200. Alcohol consumption 130. Home accidents 95. Drowning 41. Natural background radiation 8. Medical diagnostic x-rays 6. All catastrophes (fire, flood, etc.) ,000 mrem (1 rem) occupational radiation dose 1. 1,000 mrem (1 rem)/yr for 30 years 30. Note: Average U.S. occupational radiation dose is estimated at rem/year.")
51
PROGRAM FOR IMPLEMENTING PATIENT INFORMED CONSENT
AND FOLLOW UP REGARDING HIGH DOSE SPECIAL X-RAY PROCEDURES

52
Purpose: There are certain x-ray guided procedures that could result in the delivery of a radiation dose to an area of a patient’s skin of sufficient magnitude to produce clinical symptoms. This program was developed to inform patients of this potential risk prior to such procedures, determine if a procedure may lead to a large skin dose and to follow up with the patient if there is a possibility of a skin reaction.

53
Policy: This program is applicable to following x-ray guided procedures: Percutaneous Transluminal Angioplasty Radiofrequency Cardiac Catheter Ablation Vascular Embolization Stent and Filter Placement Thrombolytic & Fibrinolytic Procedures Percutaneous Transhepatic Cholangiography and/or Biliary Drainage

54
Policy (continued): Endoscopic Retrograde Cholangiopancreatography
Transjugular Intrahepatic Portosystemic Shunt Percutaneous Nephrostomy Urinary/Biliary Stone Removal Or Any other x-ray guided procedure that could expose the same area of the skin for more than 30 minutes

55
Policy (continued): For such cases, the patient must be informed in writing prior to the procedure of the risks associated with large x-ray skin doses. Appropriate follow up must be made, if after completion of a procedure, a large skin dose is possible.

56
Policy (continued): Connective tissue diseases (e.g. scleroderma, lupus erythematosus, mixed connective tissue disease), diabetes mellitus, hyperthyroidism and the homozygous form of ataxia telangiectasia have been associated with an increased sensitivity to radiation. Some chemotherapy agents are also known to increase radiation effects. To avoid injuries when using an oblique or lateral beam projection, the patient's arm must be secured away from the primary beam. Direct exposure of the female breast, especially entrance-beam exposure, must also be avoided.
, diabetes mellitus, hyperthyroidism and the homozygous form of ataxia telangiectasia have been associated with an increased sensitivity to radiation. Some chemotherapy agents are also known to increase radiation effects. To avoid injuries when using an oblique or lateral beam projection, the patient s arm must be secured away from the primary beam. Direct exposure of the female breast, especially entrance-beam exposure, must also be avoided.")
59
Radiation Biology

60
Radiosensitivity of Cells 1
As cells mature they become less sensitive to radiation As metabolic rate increases cells become more sensitive to radiation As reproductive rate increases cells become more sensitive to radiation Cell types that are most sensitive to radiation include lymphocytes and stem cells Cell types that are least sensitive to radiation include muscle and ganglion cells 1 Adapted from The 1906 Law of Bergonie and Tribondeau

61
Various degrees of sensitivity to radiation exist due to the type of tissue which receives the exposure Radiosensitive Radioresistant Breast tissue Heart tissue Bone marrow cells Large arteries Mucosa lining of small intestines Large veins Sebaceous (fat) glands of skin Mature blood cells Immune response cells Neurons All stem cell populations Muscle cells Lymphocytes
 glands of skin. Mature blood cells. Immune response cells. Neurons. All stem cell populations. Muscle cells. Lymphocytes.")
62
Radiation Induced Skin Injuries
SKIN EFFECT Single-Dose Threshold rad (Gy) Time to Onset Early transient erythema 200 (2) Hours Main Erythema 600 (6) ~10 d Temporary epilation 300 (3) ~3 wk Permanent epilation 700 (7) Dry desquamation 1400 (14) ~4 wk Moist desquamation 1800 (18) Secondary ulceration 2400 (24) >6 wk Late erythema 1500 (15) ~6 – 10 wk Ischemic dermal necrosis >10 wk Dermal atrophy (1st phase) 1000 (10) >14 wk Dermal atrophy (2nd phase) >1 yr Induration (Invasive Fibrosis) Telangiectasia d: day(s); wk: week(s); yr: year(s)
 Time to Onset. Early transient erythema. 200 (2) Hours. Main Erythema. 600 (6) ~10 d. Temporary epilation. 300 (3) ~3 wk. Permanent epilation. 700 (7) Dry desquamation (14) ~4 wk. Moist desquamation (18) Secondary ulceration (24) >6 wk. Late erythema (15) ~6 – 10 wk. Ischemic dermal necrosis. >10 wk. Dermal atrophy (1st phase) 1000 (10) >14 wk. Dermal atrophy (2nd phase) >1 yr. Induration (Invasive Fibrosis) Telangiectasia. d: day(s); wk: week(s); yr: year(s)")
63
Stochastic Effects (by chance)
Health effects that occur randomly. Effects that occur by chance, generally occurring without a threshold level of dose, whose probability is proportional to the dose and whose severity is independent of the dose. . (examples: cancer incidence and genetic effects)
")
64
Stochastic Effects (by chance)
1,000,000 persons buy a lottery ticket for $1,00 each. 999,999 persons will not get the large prize. Only one will win the BIG ONE. Return on scratch tickets is not certain.

65
Nonstochastic (Deterministic) Effects
Health effects that can be induced upon reaching an apparent threshold, and their severity varies with the radiation dose. examples: cataract in the lens of the eye, non- malignant damage to the skin

66
Nonstochastic (Deterministic) Effects
100 persons invest $1,000 at 5% interest Each person will receive $1,050.00 Return is certain

67
So....., how really dangerous is this so called “RADIATION??”

68
Radiation Injuries - Cases

69
Industrial Radiation Accident

70
An example of a skin injury attributable to x-rays from fluoroscopy is shown in Figure 2.
This case, patient A in Table 2, is that of a 40-year-old male who underwent coronary angiography, coronary angioplasty and a second angiography procedure due to complications, followed by a coronary artery by-pass graft, all on March 29, 1990. Source: Thomas B. Shope, Ph.D. (HFZ-140) FDA/Center for Devices and Radiological Health
 FDA/Center for Devices and Radiological Health.")
71
Figure 2(a). Condition of patient's back six to eight weeks following multiple coronary angiography and angioplasty procedures Source: Thomas B. Shope, Ph.D. (HFZ-140) FDA/Center for Devices and Radiological Health
 FDA/Center for Devices and Radiological Health.")
72
Figure 2(b). Appearance of skin injury approximately 16 to 21 weeks following the procedures with small ulcerated area present. Source: Thomas B. Shope, Ph.D. (HFZ-140) FDA/Center for Devices and Radiological Health
 FDA/Center for Devices and Radiological Health.")
73
Figure 2(c). Appearance of skin injury approximately 18 to 21 months following procedures, evidencing tissue necrosis. Source: Thomas B. Shope, Ph.D. (HFZ-140) FDA/Center for Devices and Radiological Health
 FDA/Center for Devices and Radiological Health.")
74
Close-up view of lesion shown in 2(c).
Figure 2(d). Close-up view of lesion shown in 2(c). Source: Thomas B. Shope, Ph.D. (HFZ-140) FDA/Center for Devices and Radiological Health
. Close-up view of lesion shown in 2(c). Source: Thomas B. Shope, Ph.D. (HFZ-140) FDA/Center for Devices and Radiological Health.")
75
Appearance of patient's back following skin grafting procedure.
Figure 2(e). Appearance of patient's back following skin grafting procedure. Source: Thomas B. Shope, Ph.D. (HFZ-140) FDA/Center for Devices and Radiological Health
. Appearance of patient s back following skin grafting procedure. Source: Thomas B. Shope, Ph.D. (HFZ-140) FDA/Center for Devices and Radiological Health.")
76
Transjugular Intrahepatic Portosystemic Shunt
6 month 23 month 10 month 22 month This patient received 3 TIPS procedures within a week 7.5 month Source: Koening, Wagner, et al., University of Texas Health Science Center

77
Radiofrequency Cardiac Catheter Ablation
Tissue necrosis 5 months after procedure, and deep ulceration with exposure of the humerus at 6.5 months Source: Koening, Wagner, et al., University of Texas Health Science Center

78
Radiation-sensitive patients
Both patients with Discoid Lupus Erythematosis received skin doses believed insufficient to cause such effects in normal skin. Reproduced with permission from Gironet et al, 1998, Ann Dermatol Venerol, 125, Reproduced with permission from Wagner et al, 1999, Radiology, 213, Courtesy of IAEA In right photo, G = graft, R = rib

79
Lessons from injured patients
Case #1:Electrophysiological and ablation procedure Three attempts in 4 months, each with more than 100 minutes of fluoroscopy. After first attempt erythema observed by patient, but not recognized as due to procedure. Erythemas on back healed. Arm lesion required grafting. Material used here previously copyrighted by Louis K Wagner 2004 or Partners in Radiation Management LTD Company 2004 and used here by permission. Courtesy of IAEA

80
Lessons from injured patients
If cause of initial erythemas was correctly identified, injury would likely have been avoided because failures of initial ablations would not have been blamed on faulty equipment. Erythemas on back healed. Arm lesion required grafting. Material used here previously copyrighted by Louis K Wagner 2004 or Partners in Radiation Management LTD Company 2004 and used here by permission. Courtesy of IAEA

81
Lessons from injured patients
Case #2: PTCA and stent placement of RCA. Involved 63 minutes of fluoroscopy and nearly 5000 frames of cine in LAO orientation with cranial tilt. Lesion required grafting. Material used here previously copyrighted by Louis K Wagner 2004 or Partners in Radiation Management LTD Company 2004 and used here by permission. Courtesy of IAEA

82
Lessons from injured patients
Case #2: Dose buildup due to long fluoroscopy and fluorography with steep angle through thick chested patient not recognized Lesion required grafting. Material used here previously copyrighted by Louis K Wagner 2004 or Partners in Radiation Management LTD Company 2004 and used here by permission. Courtesy of IAEA

83
Lessons from injured patients
Case #2: Cause of injury initially misidentified as pressure wound due to defibrillator pad. Lesion required grafting. Material used here previously copyrighted by Louis K Wagner 2004 or Partners in Radiation Management LTD Company 2004 and used here by permission.

84
Lessons from injured patients
Case #3: PTCA : 51 minutes high-dose fluoroscopy, 74 seconds cine in 141 kg man. Dose estimated retrospectively at 22 Gy. Lesion required grafting. Courtesy of IAEA

85
Lessons from injured patients
Case #3: Cumulative buildup of dose for steeply angled high-dose beam through large patient not recognized Lesion required grafting. Courtesy of IAEA

86
If you use too much radiation … you will get your ass in trouble
RULE 1 Courtesy of IAEA

87
Excess radiation can sneak up on you and catch you unaware RULE 2
A fluoroscope can be a dangerous beast Courtesy of IAEA

88
Use all protective measures at your disposal to minimize risk
Rule 3 Use all protective measures at your disposal to minimize risk

89
The End

Similar presentations