Download presentation
Presentation is loading. Please wait.

1
Dr. Hoori Mir Mohammad Sadeghi
Functional appliance Dr. Hoori Mir Mohammad Sadeghi

2
Class III

8
Class II

9
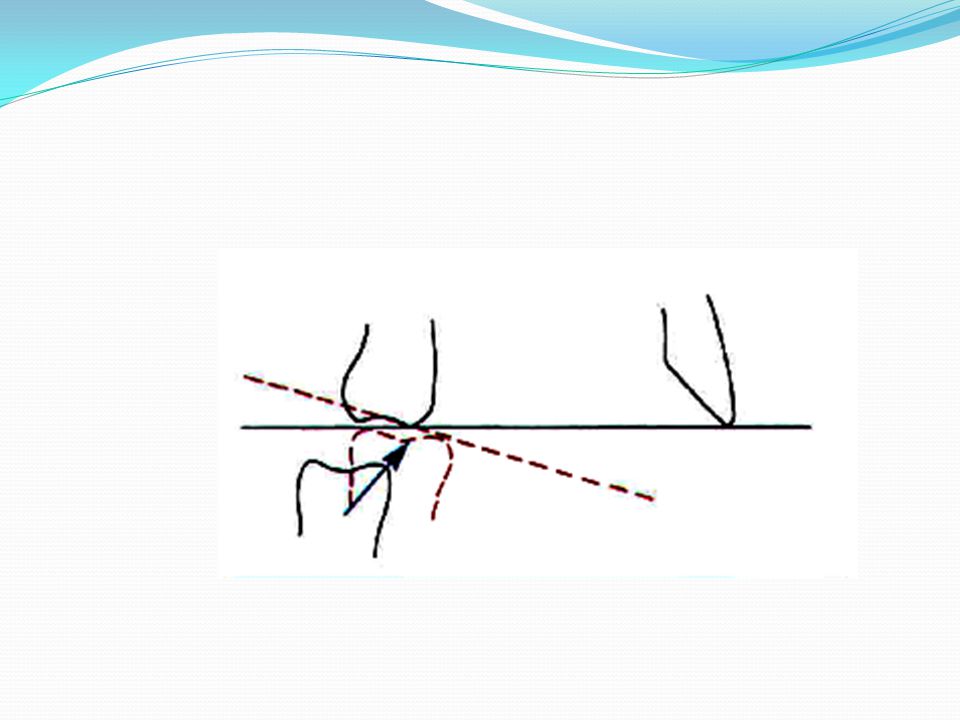
Functional appliance side effects
The most desirable and variable effect is for the mandible to increase in length as shown by the open possibly repositioning the TM fossa by apposition. The "headgear effect" restrains the maxilla and the maxillary teeth. Mandibular repositioning often creates forces against the lower teeth that cause anterior movement of the mandibular dentition. The direction in which mandibular growth is expressed, forward and/or inferiorly, is most related to the eruption of the molars. If the molars erupt more than the ramus grows in height the forward mandibular change will be negated and the Class ll malocclusion will not improve.

11
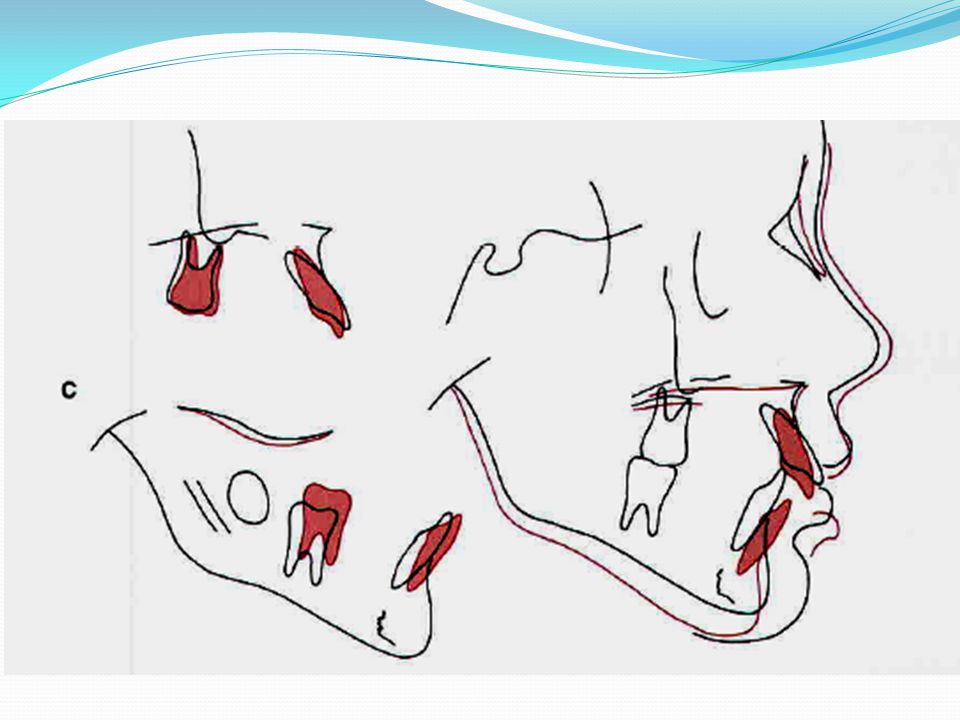
To facilitate Class ll correction
Mesial and vertical eruption of the mandibular molars. Upward and forward movement of the mandibular posterior teeth will improve the molar relationship. Establish the posterior occlusal plane at the higher level.

12
A poor response to Class ll functional appliance treatment.

14
Cervical headgear which uses a cervical neck-strap and a face-bow to produce distal force on the maxillary teeth and maxilla, is aimed at controlling maxillary size and position but is only effective if spontaneous mandibular growth also occurs.

16
Treatment Procedures With Functional Appliances

17
1.Pretreatment Alignment
The incisor position and relationships should be carefully examined. patient's ability to posture forward at least 4 to 6mm Most mandibular deficient children have a large overjet and can do this readily but in some cases incisor interferences prevent the mandible from being advanced to the correct position for the bite registration

18
The problem can be either:
Lingual displacement of the upper incisors (a Class II, division 2 incisor pattern) Irregular and crowded incisors in either arch. Either fixed or removable appliances can be used for this purpose, depending on the type and magnitude of tooth movement required.
 Irregular and crowded incisors in either arch. Either fixed or removable appliances can be used for this purpose, depending on the type and magnitude of tooth movement required.")
20
2.Impression Impression technique depends on the appliance components : Good reproduction of the teeth An accurate representation of the area lingual pads or flanges & If buccal shields or lip pads, It is important not to overextend the impressions so that tissue is displaced, location of the components leads tit long-term soft tissue irritation, discomfort, difficulty in appliance adjustment, and poor patient compliance

21
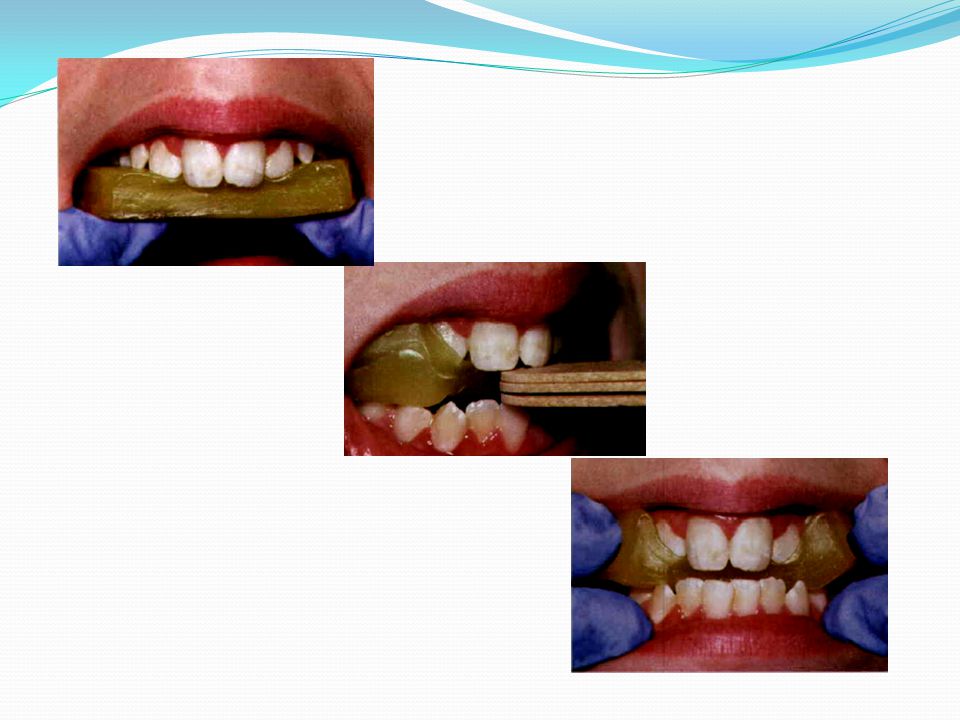
3.working bite Multiple layers of a wax hard enough
Not covering the anterior teeth or contacting the retro-molar areas (avoid any soft tissue interference with the wax). Patient's preliminary record casts
. Patient s preliminary record casts.")
22
Does not move the incisors past an edge-to edge.
Advanced symmetrically (pretreatment midline) We recommend a 4 to 6 mm advancement, but always one that is comfortable. Does not move the incisors past an edge-to edge. Quite large? Modest? relatively small?
 We recommend a 4 to 6 mm advancement, but always one that is comfortable. Does not move the incisors past an edge-to edge. Quite large Modest relatively small")
24
Opening The minimal posterior opening to achieve the vertical space is about 3 to 4 mm (Frankel appliance) There must be enough space for the laboratory technician to place wire and plastic between the teeth to connect major components of the appliance and construct occlusal & incisor stops. Interocclusal stops or facets to guide eruption, usually require 4 to 5 mm of posterior separation (Activators and Bionators) If eruption of upper and lower posterior teeth is to be limited, 5 to 6 mm total opening in the molar region ( a child with excessive vertical face height )
 If eruption of upper and lower posterior teeth is to be limited, 5 to 6 mm total opening in the molar region ( a child with excessive vertical face height )")
26
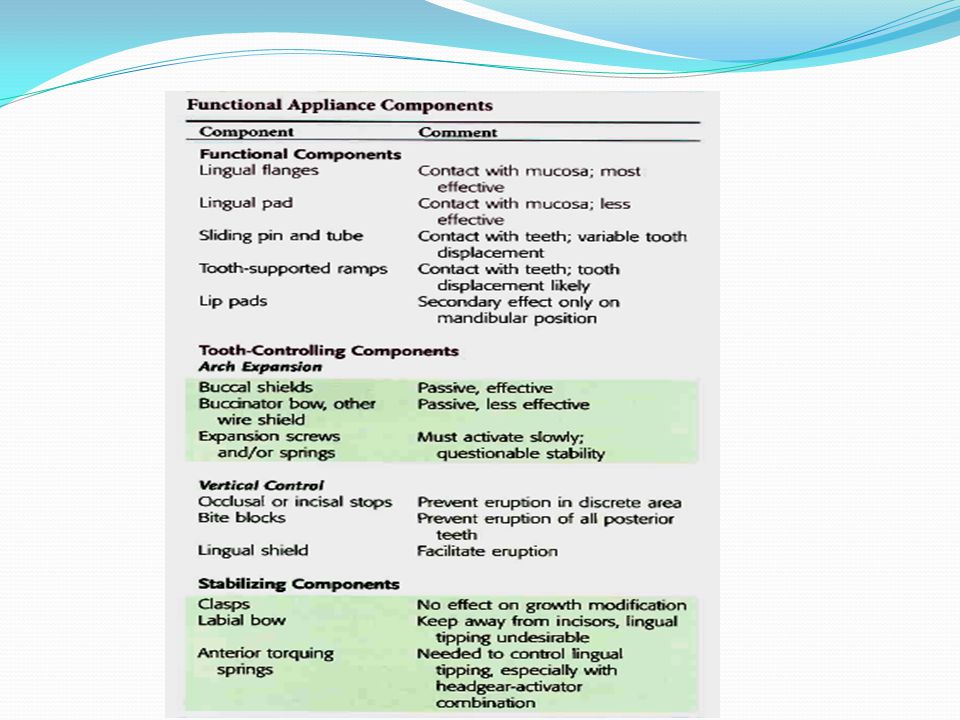
Components for Functional Appliances
Components to Advance the Mandible. Arch Expansion Components. Vertical Control Components. Stabilizing Components. Active Components.

28
Functional Components
Lingual flanges Contact with mucosa ;most effective Lingual pad Contact with mucosa; less effective Sliding pin and tube contact with teeth ;variable tooth displacement Tooth-supported ramps Contact with teeth; tooth displacement likely Lip pad Secondary effect only on mandibular position

29
Arch Expansion Buccal shields Passive effective Buccinator bow, wire shield Passive less effective Expansions crews Must activates lowly; questionable stability spring

30
Vertical Control Occlusal or incisal stops Prevent eruption in discrete area Bite blocks Prevent eruption fall posterior teeth Lingual shield Facilitate eruption

31
Stabilizing Components
Clasps No effect on growh modification Labial bow Keep away from incisors lingual tipping undesirable Anterior torquing Needed to control lingual tipping, especially with headgear-activator

33
Tooth-Borne Appliances.

34
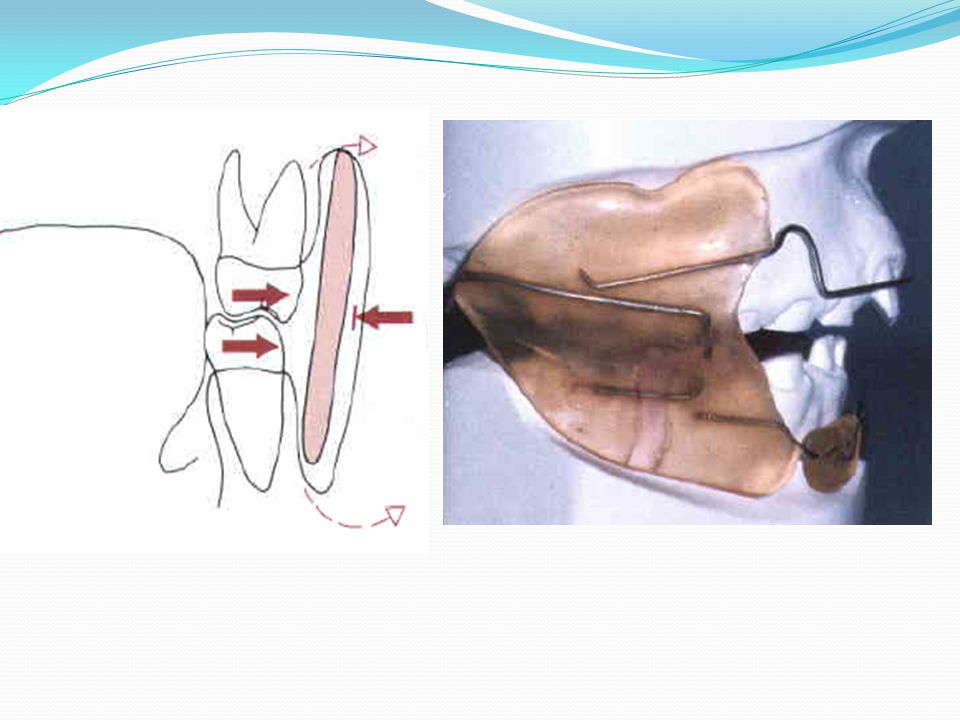
1.Activator The activator is also used to advance the mandible
Incorporate anterior and posterior bite block A labial bow The lingual shields usually extend deeper along the mandibular alveolus than other functional appliances, Displacing spring that engages the maxillary first molar s o that the appliance requires a Closed and advanced mandibular posture to retain the appliance in place.

37
2.Bionator The bionator is borne on the teeth and advances mandible.
A buccal wire to maintain the lips off the teeth Bite blocks between the posterior teeth A tongue shield Major palatal connector to stabilize the posterior segments Limited in bulk and relatively easy for the patient to accommodate

40
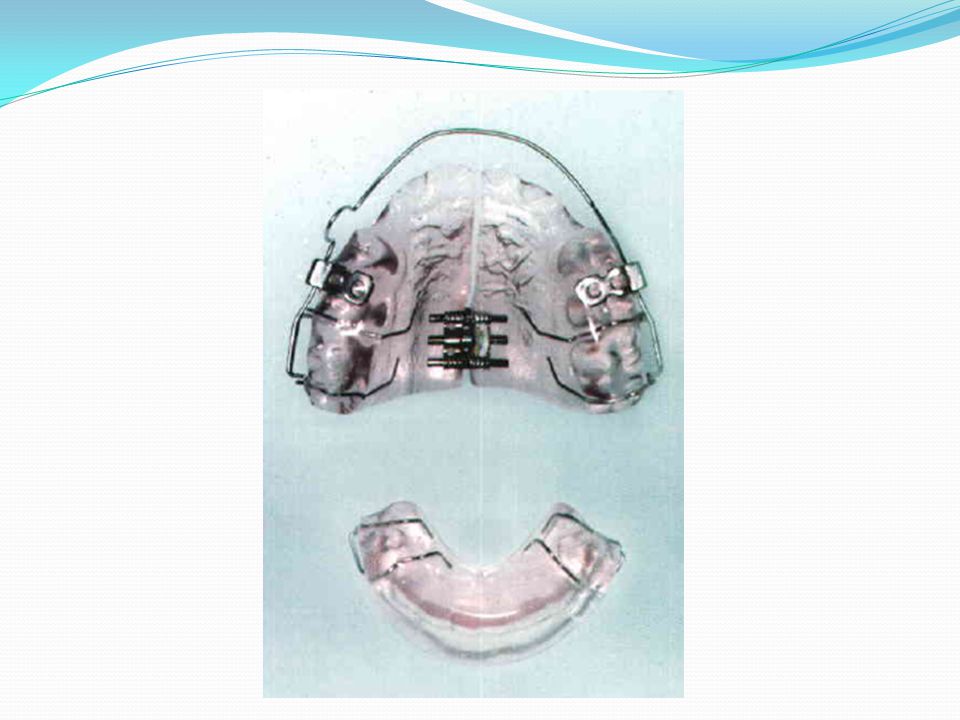
3.Twin block

42
4.Herbst

44
Tissue-Borne Appliances

45
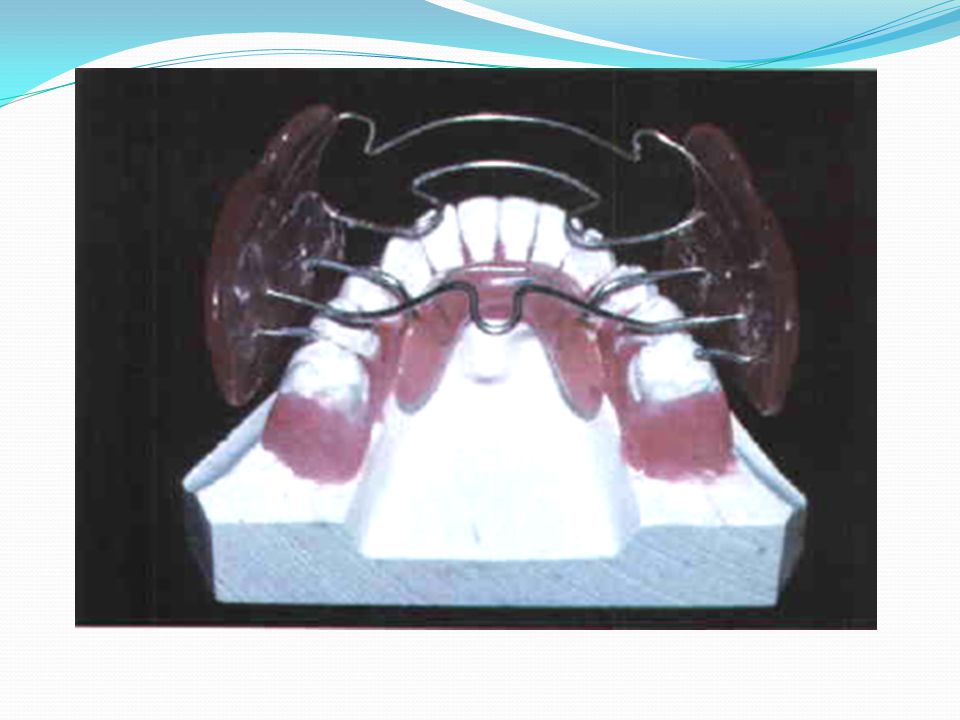
Frankel The Frankel II appliance advances the mandible and fosters expansion of the arches with the buccal shields .The lower lip pad also moves the lower lip facially. The appliance is largely tissue borne This appliance is more bulky than the activator and bionator and potentially uses more soft tissue irritation. The appliance incorporate more wire and is more susceptible to distortion.lt has wire as a major palatal connector and as stops for the maxillary molars and incisors.

49
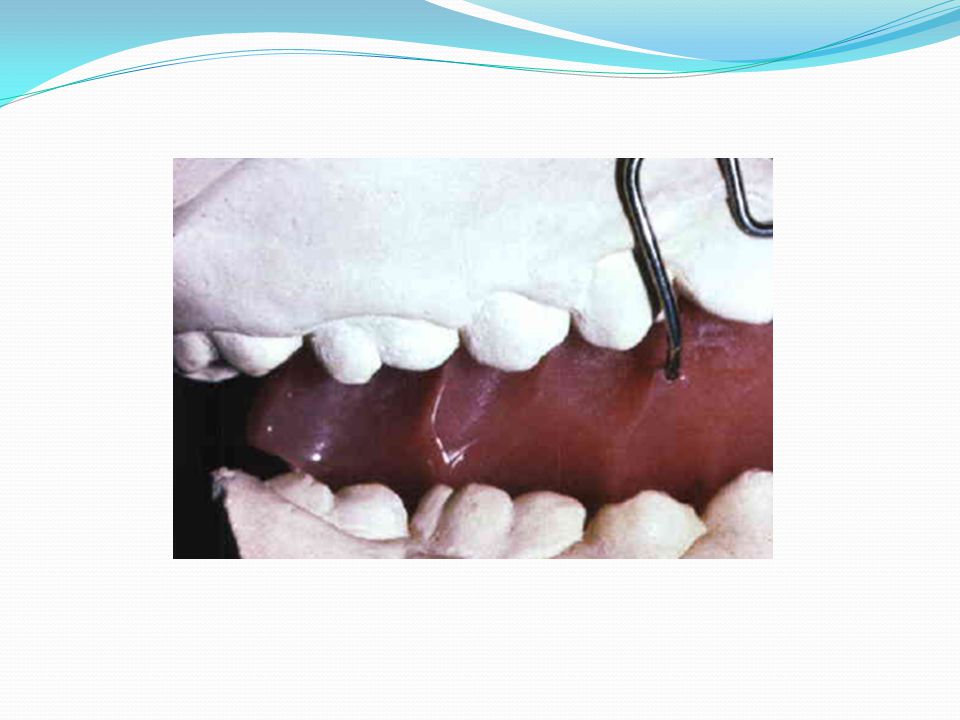
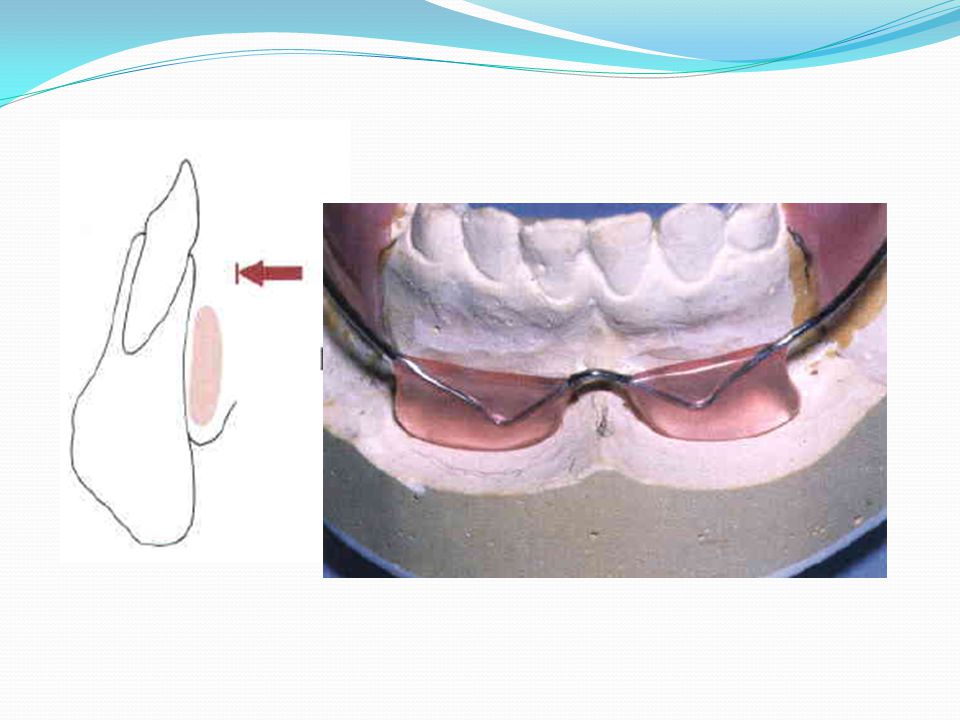
A buccal shield holds the cheek a way from the dentition and (B) facilitates posterior dental expansion b y disrupting the tongue-cheek equilibrium. The shield is placed away from the teeth in areas where arch expansion is desired). The lip pad holds the lower lip (or upper lip with a Frankel ll appliance)a way from the teeth and forces he lip to stretch to form a lip seal The pad must be carefully positioned a t the base o f the vestibule to avoid soft tissue irritation.
. The lip pad holds the lower lip (or upper lip with a Frankel ll appliance)a way from the teeth and forces he lip to stretch to form a lip seal. The pad must be carefully positioned a t the base o f the vestibule to avoid soft tissue irritation.")
52
Active tooth borne Expansion screws or springs
During functional appliance treatment, every millimeter of incisor tipping (camouflage) is a millimeter of potential skeletal correction that has been lost.
 is a millimeter of potential skeletal correction that has been lost.")
53
Headgear tubes can be incorporated into any tooth borne functional appliance so that additional distal and vertical force can be applied with a face bow and head cap Bionator Activator Buccal wire to maintain he lips off the teeth and can incorporate bite blocks between the posterior teeth and a tongue shield as this one does.

54
Hybrid functional Asymmetric patients

Similar presentations























>")







. All rights reserved. No part of this product may be reproduced or transmitted.>")



