Download presentation
Presentation is loading. Please wait.

1
Catheter-Associated Bloodstream Infections
Loreen A. Herwaldt, MD

2
4JCE Catheter-Associated Bloodstream Infection Rate
This material was prepared for use by a UIHC Committee investigating ways to reduce morbidity & mortality

3
SICU Catheter-Associated Bloodstream Infection Rate
This material was prepared for use by a UIHC Committee investigating ways to reduce morbidity & mortality

4
MICU CVC-Associated BSI
This material was prepared for use by a UIHC Committee investigating ways to reduce morbidity & mortality

5
Central Venous Catheters
A CVC is an intravenous catheter whose tip ends in the central venous system. CVC’s are commonly inserted through the jugular, subclavian, femoral, cephalic, & basilic veins. Indications Administer IV fluids, medications, blood products Total parenteral nutrition (TPN) Hemodynamic monitoring
 Hemodynamic monitoring.")
6
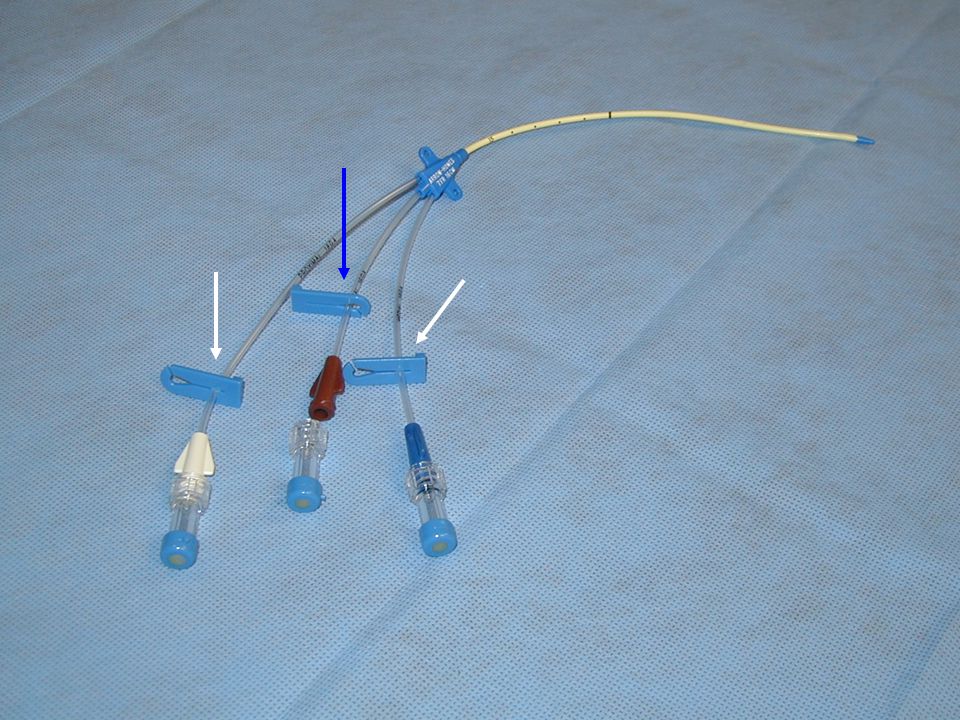
Types of Central Venous Catheters
Long-term (>4-6 weeks): totally implantable port, tunneled catheters Intermediate (>2 weeks, but <6 weeks): peripherally inserted central catheter (PICC) Short-term (<2weeks): non-tunneled central catheter (e.g., triple lumen catheter) Short-term, non-tunneled CVC Account for 90% of CA-BSI
: totally implantable port, tunneled catheters. Intermediate (>2 weeks, but <6 weeks): peripherally inserted central catheter (PICC) Short-term (<2weeks): non-tunneled central catheter (e.g., triple lumen catheter) Short-term, non-tunneled CVC Account for 90% of CA-BSI.")
8
CVC-associated Bloodstream Infections
200,000 (80,000 ICU) CVC-associated BSI in the hospital per year. 10-20% attributable mortality w/ CVC infections in the ICU. Costs of $3,700-$28,000 per line infection and total of $2.3 billion per year in US.
 CVC-associated BSI in the hospital per year % attributable mortality w/ CVC infections in the ICU. Costs of $3,700-$28,000 per line infection and total of $2.3 billion per year in US.")
9
Median Catheter-associated BSI Rates by ICU Type in US
Am J Infect Control 2001; 29:

10
Sources of Catheter-associated Bloodstream Infections
CONTAMINATION OF DEVICE PRIOR TO INSERTION Extrinsic >>Manufacturer SKIN ORGANISMS Endogenous Flora HCW hands Contam Disinfectant Invading Wound CONTAMINATION OF CATHETER HUB Extrinsic (HCW) Endogenous (Skin) CONTAMINATED INFUSATE Fluid Medication Extrinsic Manufacturer Vein HEMATOGENOUS From Distant Local Infection Fibrin Sheath, Thrombus Skin
 Endogenous (Skin) CONTAMINATED. INFUSATE. Fluid. Medication. Extrinsic. Manufacturer. Vein. HEMATOGENOUS. From Distant Local Infection. Fibrin Sheath, Thrombus. Skin.")
11
Prevention of Catheter-Associated Bloodstream Infections:
Central venous catheter insertion

12
Reducing Risk of CVC Infections
Do not routinely replace CVC without indication (NEJM 1992;327:1062-8). Remove CVC as soon as possible. Strict adherence hand hygiene & aseptic technique during CVC insertion. Use subclavian vein first, IJ second, and femoral vein last (if possible). Replace lines placed under emergency circumstances within 24 hours.
. Remove CVC as soon as possible. Strict adherence hand hygiene & aseptic technique during CVC insertion. Use subclavian vein first, IJ second, and femoral vein last (if possible). Replace lines placed under emergency circumstances within 24 hours.")
13
Reducing Risk of CVC Infections
Always use maximum sterile barrier precautions Sterile gloves and gown Nonsterile masks and hats Large sterile drapes that cover wide area Prep site with chlorhexidine gluconate (CHG) Prep with side to side scrub for 30 seconds Let dry for 30 seconds
 Prep with side to side scrub for 30 seconds. Let dry for 30 seconds.")
14
Prevention of Central Venous Catheter-Related Infection by Using Maximal Sterile Barrier Precautions During Insertion Control MSB N 167 176 % Colonization 7.2% 2.3%* Colonization per 1000 catheter days 1.0 0.3* Sepsis per 1000 catheter days 0.5 0.08* *p<0.05 vs. control Raad et al, Infect Control Hosp Epidemiol 1994;15:

15
Prevention of Catheter-Associated Bloodstream Infections:
Central venous catheter care

16
Reducing Risk of CVC Infections
Insertion site should be dressed immediately after placing catheter. Do not use topical antibiotic ointment or creams at insertion site. Transparent dressing should be changed weekly, OR Dressing should be changed if becomes damp with fluids of any type, soiled, or is non-occlusive.

17
Site Care for CVCs Change dressing when wet, soiled or bloody
Change transparent dressings q 7 days Change gauze dressings q 2 days

18
Site Care for CVCs Perform hand hygiene. Assemble supplies.
Using clean gloves, remove old dressing down to the insertion site. Pull the dressing toward the insertion site of the catheter (this helps prevent pulling out the line). Remove the remainder of the dressing by pulling off the dressing toward the insertion site
. Remove the remainder of the dressing by pulling off the dressing toward the insertion site.")
19
Site Care for CVCs Observe site for erythema, exudate or other signs of infection; notify MD if present. Examine sutures anchoring line to ensure they are intact. Put on sterile gloves & palpate the area for tenderness, swelling or fluctuance.

20
Site Care for CVCs Clean area around site with CHG in side to side motion Allow CHG to dry for 30 seconds. Do not fan or blow on the site. Apply appropriate dressing. Securely anchor catheter to skin. Record date, time and initials on tape or dressing.

21
Maintaining IV Sets Change: IV tubing q 96 hours, except
Blood tubing q 24 hours Lipid tubing q 24 hours Propofol tubing q 12 hours IV fluids q 96 hours or when meds outdate Transducers, stopcocks, flush devices, and flush solutions q 96 hours

22
Reducing Risk of CVC Infections
Cleanse outside of hubs with alcohol before each use – allow to air dry. Use TPN only when appropriate & administer through dedicated port.

23
Reducing Risk of CVC Infections
Guidewire exchanges of CVC

24
A Controlled Trial of Scheduled Replacement of Central Venous and Pulmonary-Artery Catheters Cobb et al (NEJM 1992;327:1062-8) Randomized pts. to one of four study Groups: Routine CVC change Q 3 day by GWX Routine CVC change Q 3 day to new site CVC change by GWX only when CVC change indicated CVC change to new site only when CVC change indicated.

25
A Controlled Trial of Scheduled Replacement of Central Venous and Pulmonary-Artery Catheters Cobb et al (NEJM 1992;327:1062-8) No difference in infection rate in pts. undergoing scheduled change vs. those undergoing line change when indicated. Higher rate CR-BSI in patients undergoing GWX (p=0.06). High rate of mechanical complications in patients undergoing new stick (p=0.005).
. High rate of mechanical complications in patients undergoing new stick (p=0.005).")
26
Guidewire Exchange Routine GWX of lines as prophylaxis against CVC infection not supported by literature. Acceptable when line infection not suspected. Do not use guidewire techniques to replace CVC for which there is strong suspicion of CVC-associated infection. Tunneled CVC should never be changed over a guidewire. Ok for line malfunction, new port for TPN, need to change type of line if no fever, elevated WBC or other clinical evidence of line infection Potential indications for GWX when infection suspected History of difficult line placement No site for a new puncture (burns, venous thrombosis, etc.) High or catastrophic risk of pneumothorax (e.g.. pneumonectomy patient on contralateral side from surgery) Anticoagulation (guidewire exchange still not risk free)
 High or catastrophic risk of pneumothorax (e.g.. pneumonectomy patient on contralateral side from surgery) Anticoagulation (guidewire exchange still not risk free)")
27
Recommended Procedure for Guidewire Exchange of CVC
Wide skin prep as with all CVC placements. Double glove and use MSB technique. Once old line removed, remove outer gloves prior to handling new line. Use new sterile caps on ports & new IV tubing. When prepping, hold catheter with one hand, which is now contaminated (like Foley placement). Prep with other hand, starting with skin and then working up the line. Place prepped line either on to chest or on to a sterile barrier opened for this purpose, but not onto the bed (contaminating prep). CAUTION: do not cut if patient is unstable or this is the only access!
. Prep with other hand, starting with skin and then working up the line. Place prepped line either on to chest or on to a sterile barrier opened for this purpose, but not onto the bed (contaminating prep). CAUTION: do not cut if patient is unstable or this is the only access!")
28
Blood Cultures and Central Venous Catheter Infections
Diagnosis of catheter-associated bloodstream infection depends on a positive blood cx Contamination of cultures can result in unnecessary use of antibiotics and possible CVC removal

29
Blood Cultures and Central Venous Catheter Infections
Peripheral sites are preferable to CVC hubs for obtaining blood cx. Antiseptic should be applied to both skin or catheter hub, and blood cx bottle/ tube (air dry – no blowing or fanning). Drawing less than the correct amount (8-10 mls) into a blood cx bottle reduces culture sensitivity.
. Drawing less than the correct amount (8-10 mls) into a blood cx bottle reduces culture sensitivity.")
Similar presentations










 related blood stream infections occur in the United States each year, with a mortality of 12% to 25%>")





>")


