Download presentation
1
Frank R. Ebert, MD Union Memorial Hospital Baltimore, Maryland
TOTAL KNEE ARTHROPLASTY Frank R. Ebert, MD Union Memorial Hospital Baltimore, Maryland

2
Total Knee Arthroplasty
Goal Restore mechanical alignment Restore joint line

3
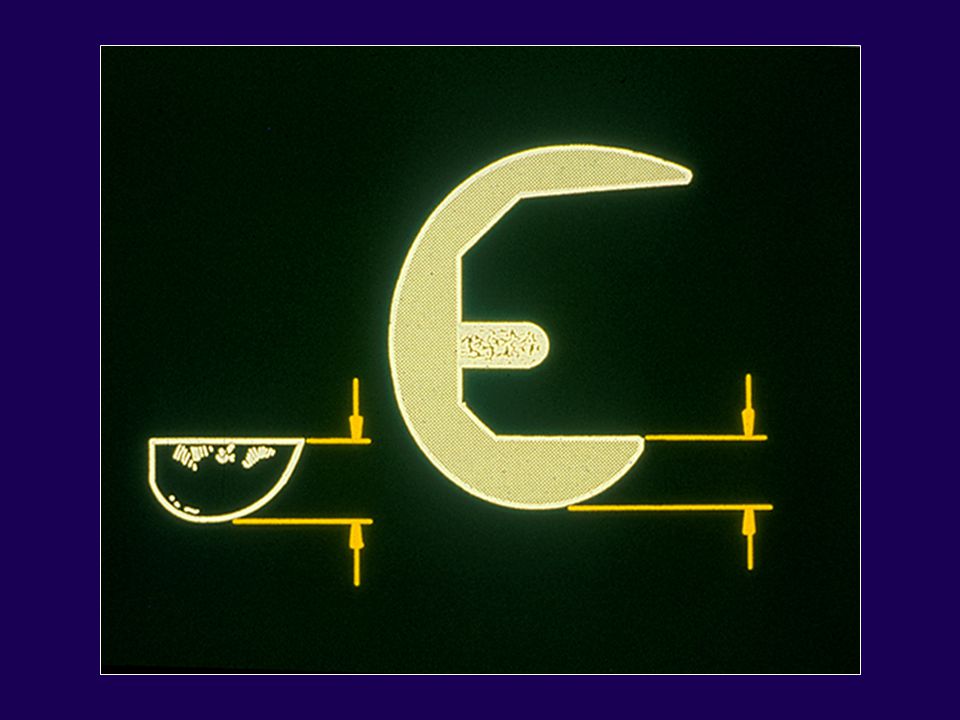
Normal Knee Anatomy Position in single leg stance
Mechanical axis valgus 3º Femoral shaft axis valgus 6º Proximal tibia varus 3º

5
Total Knee Arthroplasty
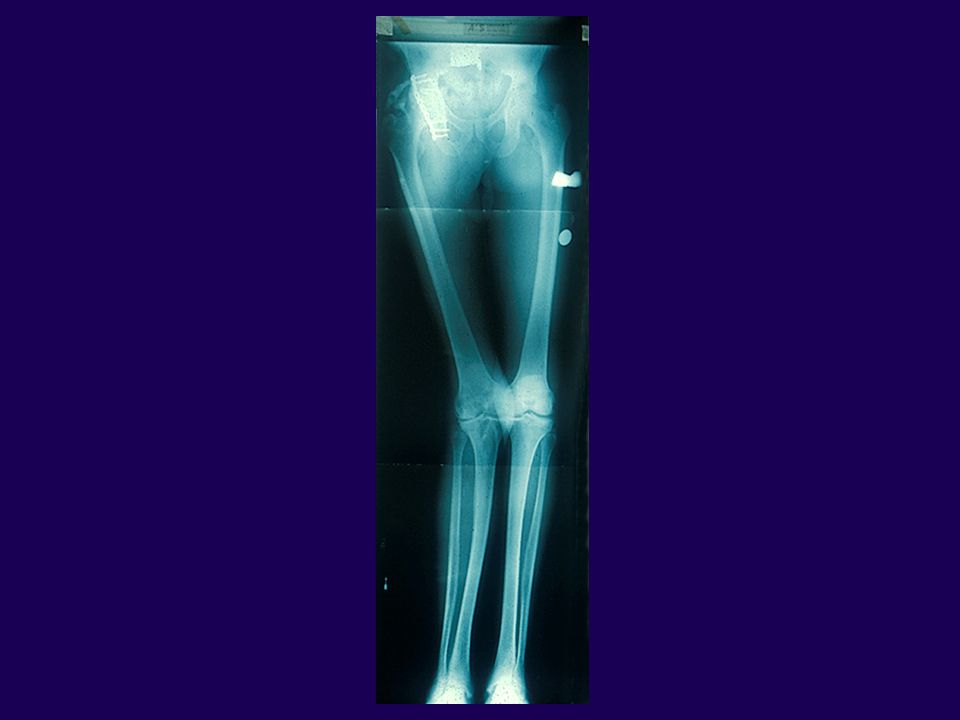
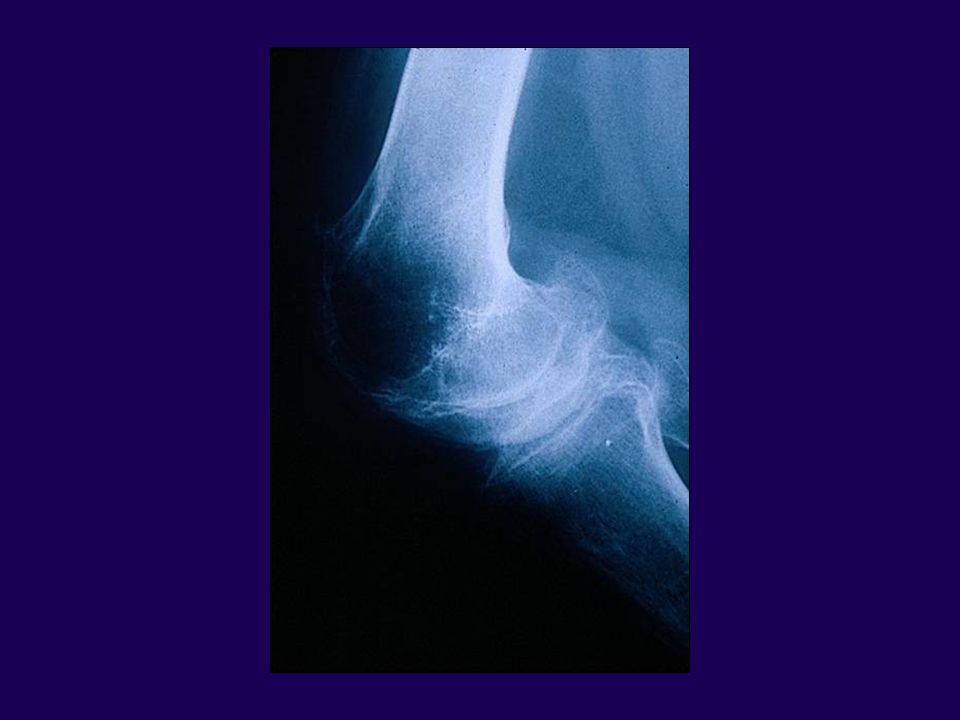
Radiographic Evaluation Standing full length – AP Standing AP Extension/Flexion laterals Tunnel view Sunrise view

7
Total Knee Arthroplasty
Radiographic Evaluation Weight Bearing X-rays Extent of joint space narrowing Ligament stretch out Subluxation of femus on tibia

9
Total Knee Arthroplasty
Radiographic Analysis Anatomic Axis – Femur Line that bisects the medullary canal of the femur Determines the entry point of the femoral medullary guide rod

11
Total Knee Arthroplasty
Radiographic Analysis Mechanical Axis – Femur (MAF) A line from center of femoral head to center of distal femur
 A line from center of femoral head to center of distal femur.")
13
Total Knee Arthroplasty
Radiographic Analysis Anatomic Axis Tibia (AAT) A line that bisects the medullary canal of the tibia Determines the entry point of the guide rod
 A line that bisects the medullary canal of the tibia. Determines the entry point of the guide rod.")
15
Total Knee Arthroplasty
Radiographic Evaluation Mechanical Axis – Tibia (MAT) Line from center of proximal tibia to center of ankle Proximal tibia is cut perpendicular to (MAT)
 Line from center of proximal tibia to center of ankle. Proximal tibia is cut perpendicular to (MAT)")
17
Issues with Surgical Techniques
Traditional Joint Line Orientation Tibial cut perpendicular to the MAT Femoral shaft at a valgus angle 5º to 8º valgus based off the ong standing x-ray

19
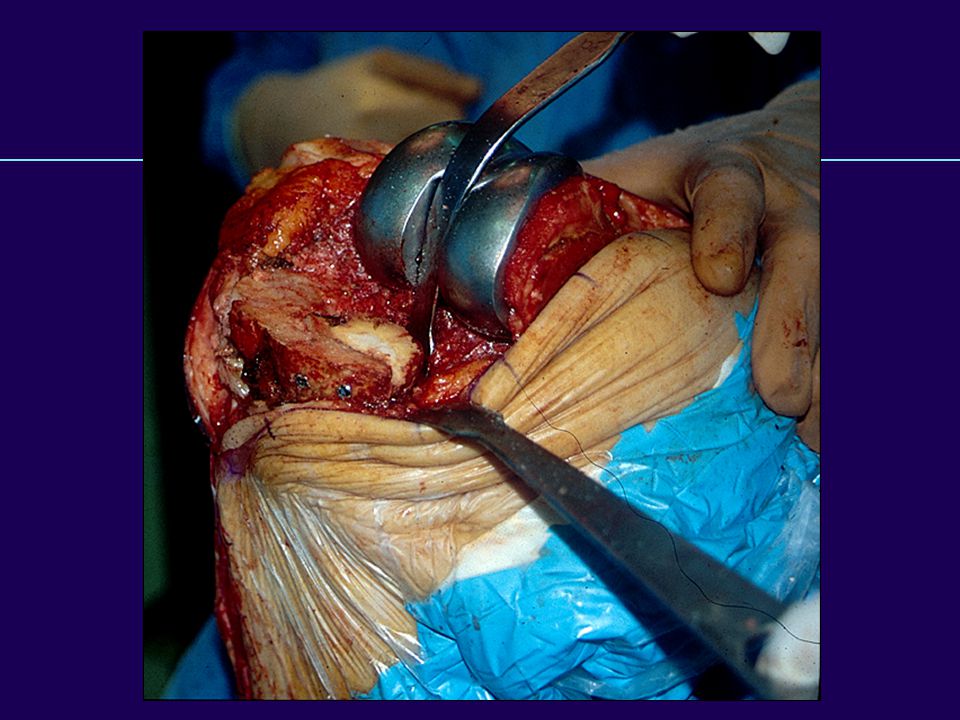
Surgical Technique Incision — straight longitudinal incision
Tissue handling key Avoid flaps Preserve soft tissue flap about the patella

21
Surgical Technique Remember 7cm Rule between incisions

23
Issues with Surgical Techniques
Exposure options — Subvastus / midvastus u Routine knee replacements z Quicker rehab — Medial parapatellar / midline u Difficult total knee — obese patients u Revisions

26
MIS vs MINI TKA Capsulotomy only? Mid vastus? Sub vastus? MIS

27
MIS vs MINI TKA Mid vastus? Sub vastus? Quad sparing? MIS

28
Anatomic Variations of VMO Insertion
Type I-High Insertion Area of Variation Type II-Pole Insertion Type III-Low Insertion

29
Type I- High VMO Insertion
Area of extended retinaculum Muscle Insertion Retinacular Incision

30
Type II-Pole Insertion
Capsular or Retinacular Incision Muscle Insertion

31
Type III-Low VMO Insertion
Area of Extended VM Muscle Insertion

32
Issues with Surgical Techniques
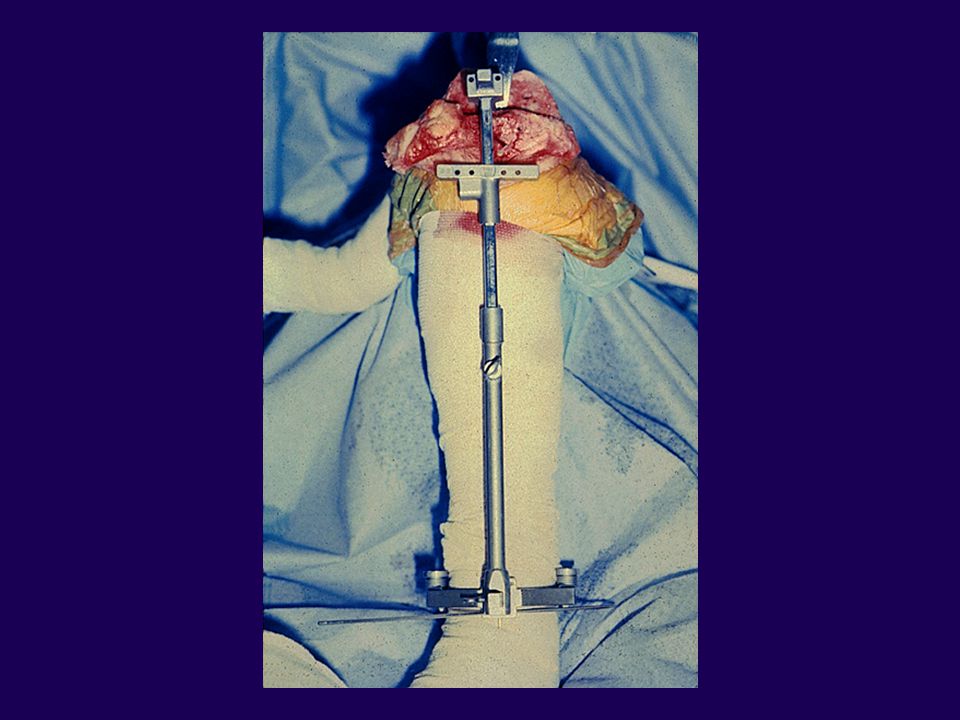
Alignment Extramedullary vs Intramedullary Accuracy vs increased PE risk Femur – Intramedullary z Overdrill opening and insert slowly IM guide z Caution with bilateral Total Knee Arthroplasty Tibia – Extramedullary

34
Issues with Surgical Techniques
Femoral Rotation Landmarks Posterior femoral condyles Epicondyles 5º external rotation to the posterior condyles

38
Issues with Surgical Techniques
Femur Measured resections: equal bone distally and posteriorly Tensioning devices & ligament releases Do not alter bone resection for ligament tightness

40
Issues with Surgical Techniques
Tibial Component Rotation Transmalleolar axis Posterior tibial plateau Tibial tubercle — lies lateral

44
Malalignment Tibial Component Internally Rotated Tubercle Too Lateral

46
Management of Deformity
1. Release the tight side of the deformity 2. Tighten the loose side 3. Accept some residual soft tissue imbalance 4. Combination

48
Surgical Techniques Varus Knee 1. Pes anserinus 2. Joint Capsule
3. Deep Tibial Collateral 4. Semimembranosus 5. Posterior Medial Capsule

52
Varus Knee

53
Varus Knee

54
Varus Knee

55
Varus Knee

56
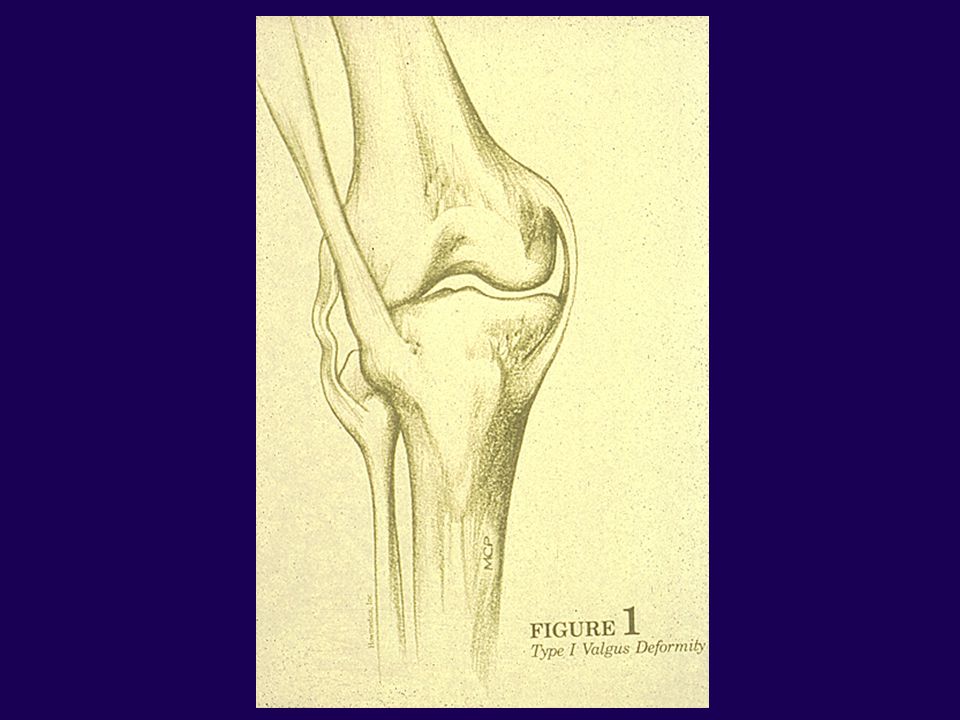
Surgical Techniques Valgus Knee 1. Iliotibial Band 2. Popliteus Tendon
3. Posterior Lateral Capsule 4. Lateral Head of Gastroc 5. Biceps Femoris

60
Surgical Techniques Valgus Knee
Peroneal nerve palsy – valgus / flexion deformity Treatment Release dressings or flex the knee

62
Surgical Techniques: Flexion Contracture 1. Posterior capsule
2. Gastroc origins 3. Posterior cruciate 4. Distal femur

63
Fixed Flexion Deformity in TKA
Complex Combinations: — musculotendinous contracture — ligamentous contracture — capsular contracture — osteophytes of posterior condyle

64
Fixed Flexion Deformity in TKA
Biomechanics — increased quadriceps force for knee stabilization during weight bearing — increased forces transmitted to the patellofemoral joint

65
Fixed Flexion Deformity in TKA
Biomechanics — increased forces are placed on posterior tibial plateau — femoral condyles sink into the tibial plateau — contact between intercondylar notch and tibial eminence form a boney block

66
Fixed Flexion Deformity in TKA
Associated deformity — varus deformity 40% - > 5º range 5 to 30º varus — valgus deformity 30% - > 5º range 5 to 22º valgus Firestone et al COOR ‘92

67
Fixed Flexion Deformity in TKA
Incidence of Problem – Review of 700 TKA & Revision TKA’s — 60% before primary TKA — 21% before revision TKA Tew & Forster JBJS (B) 87
 87.")
68
Fixed Flexion Deformity in TKA
Soft tissue release — Varies with angular deformity Firestone et al COOR ‘92

69
Fixed Flexion Deformity in TKA
Surgical Treatment Soft tissue release Additional bone resection Combination

70
Fixed Flexion Deformity in TKA
Postoperative Correction — the more severe the deformity must consider the pros and cons of additional bone resection and/or soft tissue release Volz COOR ‘89

71
Fixed Flexion Deformity in TKA
Additional bone resection – pros — joint line is positioned slightly more proximal — functionally lengthens the collaterals and posterior capsule forward extension — doesn’t compromise flexion stability Firestone et al COOR ‘92

72
Fixed Flexion Deformity in TKA
Additional bone resection — cons (excessive) Collateral ligament laxity Quadriceps redundancy Hyperextension Bone quality can be compromised McPherson et al ‘94
 Collateral ligament laxity. Quadriceps redundancy. Hyperextension. Bone quality can be compromised. McPherson et al ‘94.")
73
Additional Femoral Resection

75
Fixed Flexion Deformity in TKA
Surgical Treatment for Deformity < 10º FFC Soft tissue release – only necessary — posterior capsule — possibly PCL — posterior osteophytes

76
Fixed Flexion Deformity in TKA
Surgical Treatment for Deformity º FFC — consider distal femoral resection to 5 mm — Posterior capsule — PCL resection posterior osteophytes Firestone et al COOR ‘92

77
Fixed Flexion Deformity in TKA
Surgical Treatment for Deformity º FFC — distal femoral resection 3 to 5 mm — posterior capsule — PCL resection posterior osteophytes Firestone et al COOR ‘92

78
Fixed Flexion Deformity in TKA
Surgical Treatment for Deformity > 30º FFC — consider pre-op casting ≠ — distal femoral resection 5 mm — proximal tibial resection — PCL resection — posterior osteophytes Firestone et al COOR ‘92 et al J of Arthro ‘99

79
Fixed Flexion Deformity in TKA
Peroneal Nerve Palsy Vascular Insufficiency Anterior Pressure Ulcers Manipulation

83
Fixed Flexion Deformity in TKA
No formula is exact for treatment of the problem Consider a balance between soft tissue release vs bone resection

84
Issues with Surgical Techniques
Stiff Knee Remove osteophytes Insall Turn Down Osteotomize the tibial tubercle Rectus snip

89
Issues with Surgical Techniques
Stiff Knee Epicondylar osteotomy for large flexion / contracture Lateral release to evert the patella

93
Issues with Surgical Techniques
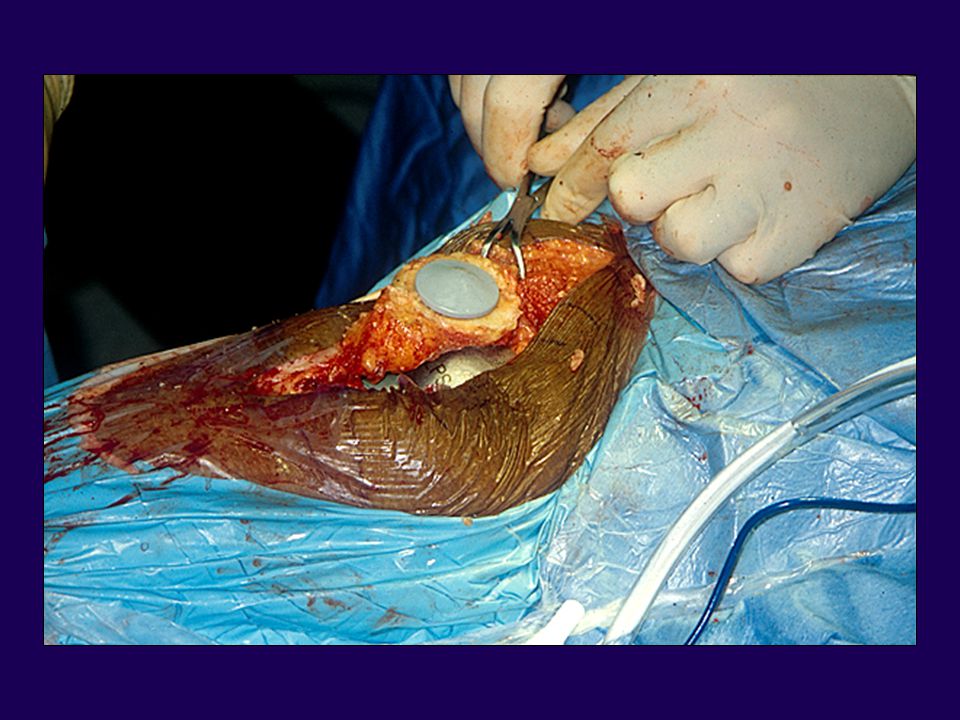
Patellar resurfacing Recommended for all RA patients Without resurfacing 4% to 6% incidence of anterior knee pain With resurfacing increased incidence of fracture

95
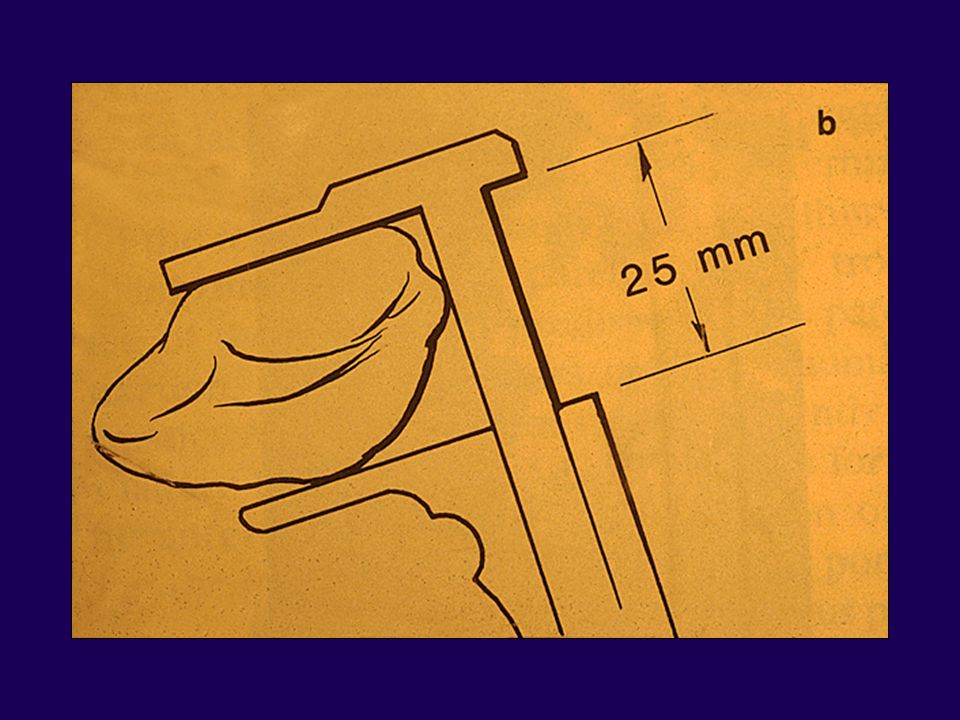
Issues with Surgical Techniques
Patellar resurfacing Thickness shouldn’t exceed 25 mm For every 1 mm thicker reduces flexion by 3º

99
Issues with Surgical Techniques
Patellar Baja Proximal tibial osteotomy Tibial tubercle shift Prior fracture

100
Issues with Surgical Techniques
Patellar Baja Don’t raise joint line Consider lowering joint line — Distal femoral alignment Trim anterior tibial poly to avoid impingement of patella

101
Issues with Surgical Techniques
Patellar Clunk Syndrome — Seen at 35º-40º knee flexion — Treatment is arthroscopic or open resection

102
Issues with Surgical Techniques Sagittal Plane Balancing
Situation Problem Solution Cut Tight Symmetrical – cut more in extension gap proximal tibia Cut Tight in flexion Cut Tight Asymmetrical – Release PCL; in extension gap Posterior capsule Cut Loose Consider PCL in flexion substituting prosthesis – Resection distal femur AVOID recurvatum

103
Issues with Surgical Techniques Sagittal Plane Balancing
Situation Problem Solution Cut Good Asymmetrical – Resection additional in extension gap tibia Cut Tight in flexion – May need to release PCL – Ensure posterior slope of tibia Cut Good Asymmetrical – Need femoral in extension gap augmentation Cut Loose – Adjust to larger in flexion femoral component

104
Complications in Total Knee Arthroplasty
Periprosthetic Fractures Infected Total Knee Arthroplasty

105
After Total Knee Arthroplasty
Supracondylar Fractures of the Femur After Total Knee Arthroplasty

106
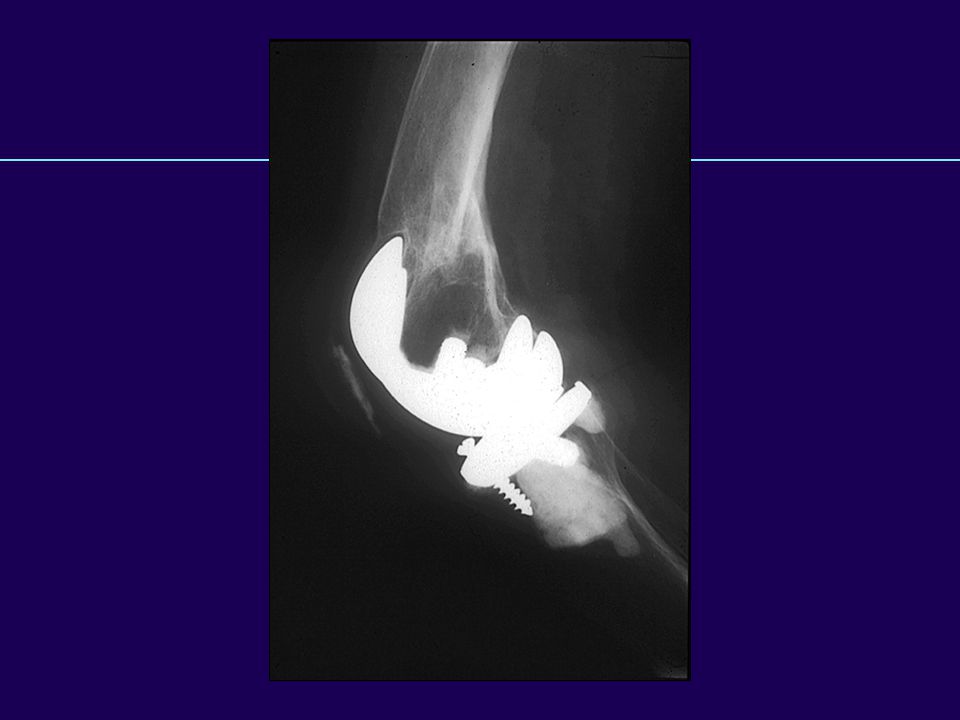
Supracondylar Fractures After TKR
Notching of the femoral cortex Osteoporosis Prolonged steroid use Preexisting neurologic disorders

108
Supracondylar Fractures After TKR
OSTEOPOROSIS Bogoch, et al, CORR 1986

110
Supracondylar Fractures After TKR
Major trauma is not required to produce fractures in many TKA patients Alignment not correlated with fracture Weight not a significant factor

111
Fractures After TKA Neer Classification of Supracondylar Fractures
Type I - Minimal displacement Type IIA - Medial displacement of condyles Type IIB - Lateral displacement of condyles Type III - Supracondylar and shaft fractures

112
Supracondylar Fractures After TKR
TREATMENT Type 1 – Nondisplaced

113
Supracondylar Fractures After TKR
Type 1 fractures 83% success rate Chen, et al, 1994

115
Supracondylar Fractures After TKR
Type 2 fractures 69% success rate Chen, et al, 1994

116
Supracondylar Fractures After TKR
Non Operative Method Casting Traction followed by rest

117
Supracondylar Fractures After TKR
Type 2 fractures 67% success rate Chen, et al, 1994

118
Supracondylar Fractures After TKR
Operative Method Plates / Screw fixation Intramedullary rods Rush pins External fixation Primary arthrodesis Revision arthroplasty

119
Supracondylar Fractures After TKR
Type 2 Considerations Patients’ ability to tolerate traction Ability of bone to hold screws Ability of the surgeon

122
Intercondylar Distances of Commonly Used Femoral Prostheses
Intercondylar Distance (Smallest Size) (mm) Manufacturer Model Biomet, (Warsaw, IN) AGC Universal 18 DePuy, (Warsaw, IN) AMK 20 Dow Corning Wright, (Arlington, TN) Whitesides modular 20 Howmedica, (Rutherford, NJ) PCA 18.5 Intermedics, (Austin, TX) Natural 14 Johnson and Johnson, (New Brunswick, NJ) Press-fit condylar 20 Insall-Burstein* (posterior stabilized) Kirschner, (Timonium, MD) Performance 14 Zimmer, (Warsaw, IN) Insall-Burstein I* 16 Insall-Burstein II (posterior stabilized* or constrained condylar†) Miller-Galante I Small / small + ‡ Regular / regular Large / large Large Miller-Galante II 13
 (mm) Manufacturer. Model. Biomet, (Warsaw, IN) AGC 18 Universal 18. DePuy, (Warsaw, IN) AMK 20. Dow Corning Wright, (Arlington, TN) Whitesides modular 20 Howmedica, (Rutherford, NJ) PCA 18.5 Intermedics, (Austin, TX) Natural 14 Johnson and Johnson, (New Brunswick, NJ) Press-fit condylar 20 Insall-Burstein* 15 (posterior stabilized) Kirschner, (Timonium, MD) Performance 14 Zimmer, (Warsaw, IN) Insall-Burstein I* 16 Insall-Burstein II 15 (posterior stabilized* or constrained condylar†) Miller-Galante I Small / small + ‡ 11 Regular / regular Large / large + 15 Large Miller-Galante II 13.")
124
Supracondylar Fractures After TKR
No one form of treatment gives uniformly good results

125
Infection in Total Knee Arthroplasty

126
Complications in Arthroplasty
Infection – Risk Factors Skin ulcerations / necrosis Rheumatoid Arthritis Previous hip/knee operation Recurrent UTI Oral corticosteroids

127
Complications in Arthroplasty
Infection – Risk Factors Chronic renal insufficiency Diabetes Neoplasm requiring chemo Tooth extraction

128
Complications in Arthroplasty
Infection – Clinical Course Pain #1 Swelling Fever Wound breakdown drainage Windsor et al JBJS; 1990

129
Early < 3 months Lab Value Infections About TKR
Mayo Series Mean 7,500 Differential 67 PMN’s Sed rate 71 mm/hr Arthrocentesis

130
Late > 3 months Symptoms: 52 patients
Infections About TKR Late > 3 months Symptoms: 52 patients Pain 96% swelling 77% Debride 27% Active drainage 27% Sed rate 63 mm/hr WBC Windsor et al JBJS; 1990

131
Complications in Arthroplasty
Infection – Surgical Techniques Avoid skin bridges Avoid creation of skin flaps Hemostasis Prolonged operating time

133
Complications in Arthroplasty
Infection – Work-Up Wound History Physical Exam Serial Radiographs Lab/sed rate/CRP Bone scan / Indium scan

135
Complications in Arthroplasty
Infection Arthrocentesis Cell count Diff > 25,000 pmn Protein – high Glucose – low

136
Complications in Arthroplasty
Infection Host Response Glycocalyx Gristina JBJS; 1983

138
Micro Organisms

139
Organisms Isolated from 71 Patients With Infected Knee Replacement
Percent Staphylococcus 64 S. aureus, penicillin sensitive S. aureus, penicillin resistant 28 S. epidermis 22 Gram negative 12 Pseudomonas 7 Escherichia coli 5 Anærobic 6 Other 17

140
Complications in Arthroplasty
Treatment Options Antibiotic suppression Aggressive wound debridement

141
Complications in Arthroplasty
Treatment Options Antibiotic suppression Indicated in med compromised Organism - gram+ strep staphepi

142
Complications in Arthroplasty
Treatment Options Resection arthroplasty 2 Stage re-implant Arthrodesis Amputation

143
Complications in Arthroplasty
Treatment Options Debridement with antibiotic suppression therapy Strep/staphepi -- best Avoid repeated attempts Frozen tissue section Suction drains

144
Complications in Arthroplasty
Two-Stage Reimplantation Most successful treatment Procedure of choice

145
Complications in Arthroplasty
Two-Stage Reimplantation Procedure Remove components, cement, I&D Fabricate and place spacer 6 weeks of antibiotics Reimplantation

146
Complications in Arthroplasty
Two-Stage Reimplantation Stage I create antibiotic spacer impregnated with antibiotics wound closure

148
Complications in Arthroplasty
Two-Stage Reimplantation Spacer Antibiotic Regimen Tobramycin 2.4 gm/3.6 gm per gms of PMMA Vancomycin > gm to 1 gm per gms of PMMA

149
Complications in Arthroplasty
Intra-operative Frozen Section < 5 PMN’s per HPF – no infection > 10 PMN’s per HPF – infection Mirra; JBJS

150
Complications in Arthroplasty
Results — Gm positive Windsor et al 92 % JBJS 1990 Insall et al 97% JBJS 1983

151
Complications in Arthroplasty
Resection Arthroplasty Removal all components Remove all cement Effective in medically compromised patient

152
Complications in Arthroplasty
Arthrodesis Indications Extensor mechanism disruption Resistant bacteria Inadequate bonestock Inadequate soft tissues Young patient

153
Advantages Definitive treatment Little chance of recurrence
Arthrodesis Advantages Definitive treatment Little chance of recurrence

154
Disadvantages Difficulty with transfers / small spaces
Arthrodesis Disadvantages Difficulty with transfers / small spaces Increase energy requirements

155
Algorithm TKA Clinical Sepsis (GRAM + Organism) < 3 wks > 3 wks
Infections About TKR Algorithm (GRAM + Organism) TKA Clinical Sepsis < 3 wks > 3 wks Debridement Antibiotics (6 wks) 2-Stage Replant
 TKA Clinical Sepsis. < 3 wks. > 3 wks. Debridement Antibiotics (6 wks) 2-Stage Replant.")
156
Debridement Antibiotics
Infections About TKR Algorithm Debridement Antibiotics 2-stage Replant No Success No Success Success Success Arthrodesis 2-stage Replant Resection Arthroplasty

157
Thank You





























































 Medial condyle (8 left) Intercondylar fossa (7 left)>")


 Joint>")

