Download presentation
Presentation is loading. Please wait.

1
the Myelodysplastic Syndromes: what they are, what they mean and what are we doing about it Anthony Woods, MD September 30, 2006

2
outline what is myelodysplasia? diagnosis & classification treatment strategies specialty clinics

3
What is…? clonal disorder affecting hematopoietic maturation, characterized by ineffective hematopoiesis and bone marrow failure with resultant cytopenias, often culminating in florid acute leukemia huh?

4
historically reports of cytopenic disorders began appearing in the early 20 th century 1942: odo-leukemia odo = threshold (Chevalier et al) 1949: preleukemic anemia (Hamilton-Paterson) 1953: expanded definition to include all blood lines clonal myeloid hemopathy (Block et al)
 1949: preleukemic anemia (Hamilton-Paterson) 1953: expanded definition to include all blood lines clonal myeloid hemopathy (Block et al)")
5
historically other terms used over the last 50 years: –herald state of leukemia –refractory anemia –sideroachrestic anemia –idiopathic refractory sideroblastic anemia –pancytopenia with hyperplastic marrow –oligoblastic leukemia

6
soapbox no surprise that there is confusion and ignorance about this disorder: historical coupling of MDS to acute myeloid leukemia there is a relationship has hindered consideration of MDS as a distinct entity –biased investigational and therapeutic efforts towards the leukemia

7
historically Paris, 1975: hemopoietic dysplasia –subsequently shortened to myelodysplasia 1982: French-American-British classification scheme (FAB) 1999-2002: World Health Organization classification scheme
 : World Health Organization classification scheme")
8
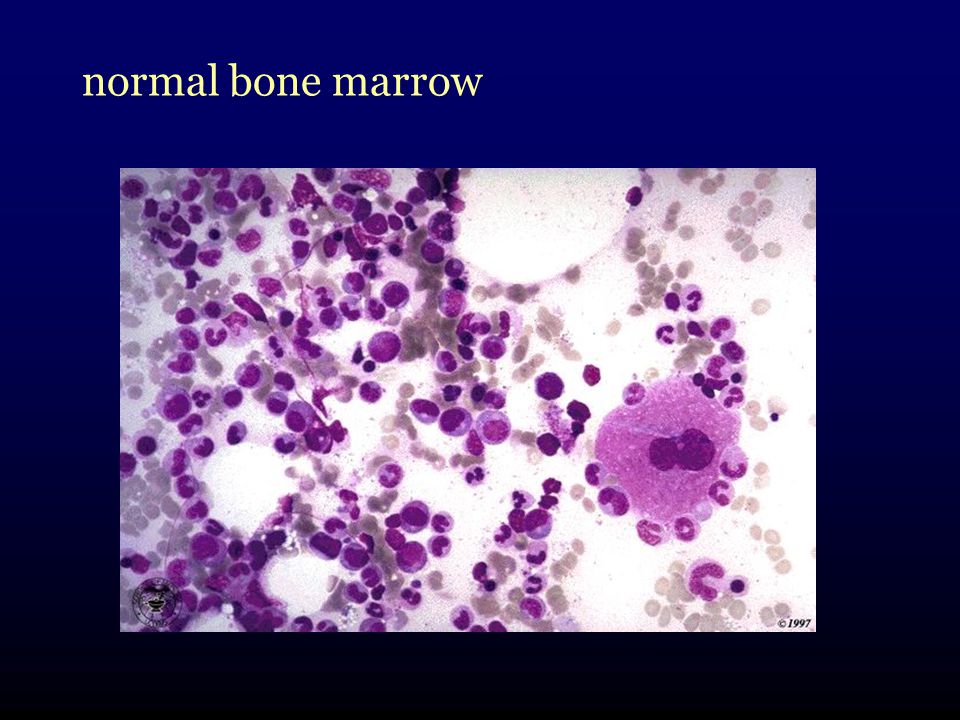
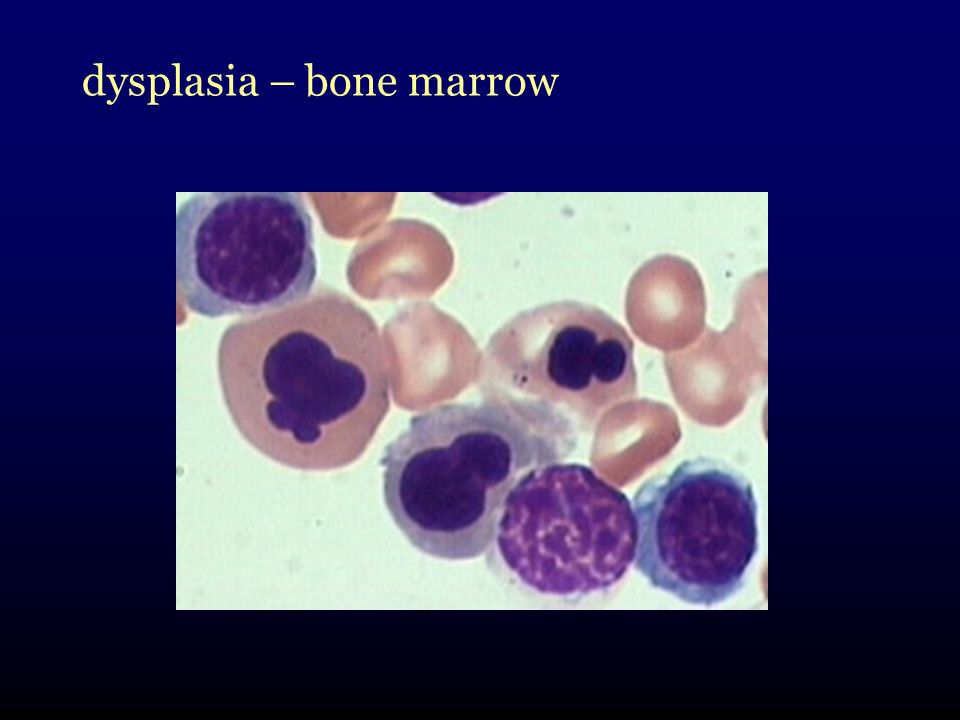
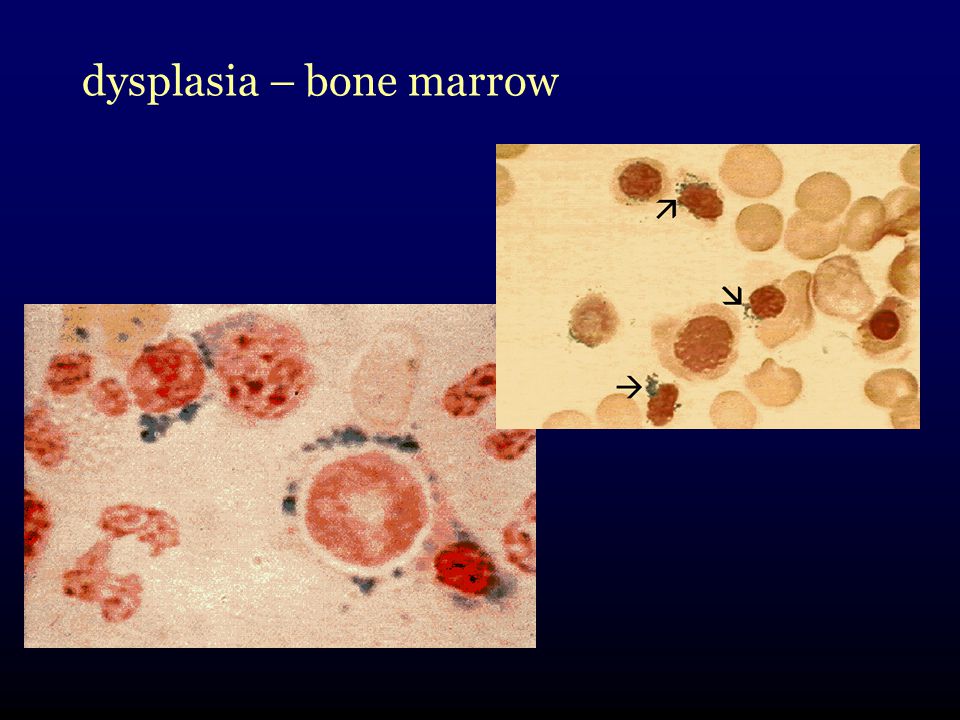
What is myelodysplasia? disordered production of one or more cell lines dysplasia abnormal growth and differentiation of hematopoietic precursors abnormal appearance under the microscope

9
normal blood

10
dysplastic features - blood

11
normal

12
dysplastic features - blood

13
normal bone marrow

15
dysplasia – bone marrow

19
what goes wrong with marrow cells? multistep process sequence of successive DNA mutations in an early blood cell precursor cell evolution of this cell into a clone –self-reproducing abnormal cell –growth advantage over normal marrow cells

20
what goes wrong with marrow cells? complex multistep process: DNA mutations in an early blood cell precursor cell emergence as an abnormal clone –self-reproducing, abnormal cell –growth advantage over normal marrow cells BUT at the same time incapable of producing normal blood cells

21
what goes wrong with marrow cells? expansion of the abnormal clone results in ineffective hematopoiesis –marrow looks full –no useful blood cell production actually occurring –suppression and inhibition of normal marrow growth weeds growing in the garden Dr. R. Wells

22
what goes wrong with marrow cells? worse, over time the clone becomes more and more unstable ~ 25% of persons with MDS develop acute myeloid leukemia

23
what goes wrong with marrow cells? C. Willman, ASH Education Program, 2000 MDS AML

24
causes may follow exposures to bone marrow toxins –chemotherapy –radiation –organic compounds some follow inherited tendencies Fanconi anemia, disorders of DNA repair > 80% have no identifiable exposure or cause

25
in whom and how often can affect people of any age –including children more common in advancing age –North America: mid-late 60s –China: 50 10000-15000 new diagnoses per year in USA –Canada 10% ?

26
in whom and how often MDS Foundation estimates that in people older than 70 there are 15 - 50 new diagnoses / 100,000 persons per year extrapolating USA estimates, perhaps 3000 - 6000 Canadians have an MDS diagnosis at any given time

27
diagnosis requires suspicion typically 2 settings where MDS should be suspected: 1.signs or symptoms of a blood disorder –fatigue, exercise intolerance, pale –serious or recurrent infections –inappropriate bleeding and bruising

28
diagnosis 2.unexpected finding in blood suggesting MDS: –low blood count of any kind > 80% have anemia ± others 30 – 45% have low platelets –macrocytosis (large red cells) –high monocyte count –abnormal appearing blood cells
 –high monocyte count –abnormal appearing blood cells")
29
diagnosis required evaluation: complete history and examination complete blood counts and diff iron, B12 and folate levels bone marrow aspirate & biopsy –chromosome analysis: cytogenetics serum erythropoietin levels –prior to transfusions

30
diagnosis tests that are useful in some clinical circumstances –HLA tissue typing (if BMT a consideration) –HIV testing –other specific tests PNH other HLA determinations
 –HIV testing –other specific tests PNH other HLA determinations")
31
diagnosis no perfect diagnostic test no absolute diagnostic criteria combination of findings: –appearance of dysplasia in blood and marrow –abnormal cytogenetic testing

32
complications related to low blood counts fatigue, decreased exercise tolerance serious, recurrent infection bleeding the latter two are responsible for the majority of severe and life-threatening complications of MDS

33
complications approximately 25% of patients undergo a transformation to acute myeloid leukemia arbitrary distinction of having 20% blast cells in bone marrow represents an increase in the aggressiveness of their MDS associated with a worse prognosis

34
complications suspected if: drop in baseline blood counts higher blast cell numbers showing up in blood higher transfusion requirements non-specific symptoms –weight loss

35
classification 2 classification systems still in use FAB System newer WHO classification

36
FAB classification many clinicians still primarily use this system framework upon which newer classifications are built FAB grouping gives prognostic information: all tables from Steensma et al, May Clin Proc, 2006

37
FAB classification

38
WHO Classification meant to refine the FAB system: incorporated new information –cytogenetics added subcategories for recognized specific sub-entities – 5q - syndrome also takes into account changes in AML diagnostic criteria –20% vs 30%

39
WHO Classification

40
International Prognostic Scoring System need for a better system to predict prognosis in certain patient groups IPSS: a tool specifically designed for prognostic purposes arose out of a 1997 international workshop on MDS Risk Analysis analyzed factors in 816 patients

41
IPSS calculation

42
therapy many potential therapies available to & tried in MDS patients most show some benefit most benefits are –small –only in a minority subset of patients hard to know who should receive them and what to expect

43
transfusion and general supportive measures most persons with MDS require transfusion support at some time during their course most people do not tolerate hemoglobin < 80 g/L –at least 80 or for comfort/symptoms –CMV negative products in potential BMT recipients

44
therapy platelet transfusion is individualized based on baseline counts and bleeding symptoms –alloimmunization to platelets –local blood bank guidelines adjunctive agents can be used –tranexamic acid

45
therapy management of iron overload –Dr. Wells

46
therapy prompt attention given to infectious symptoms primary care physicians should be aware of increased importance of infections in persons with MDS trials of growth factors with infections –inpatient setting –selected outpatients

47
therapy growth factors: erythropoietin and G-CSF rationale is to encourage hematopoiesis responses are variable expensive, not readily obtainable to everyone –3 rd party insurance –sneak past renal guidelines

48
therapy EPO compounds (Eprex) have generally shown response rates of 15-20% better responses seen in: –RCMD-RS –low EPO levels –lighter transfusion needs responses generally last 1-2 years doses: 40-60,000 units SC weekly newer compounds appear equally effective –darbepoietin (Aranesp)
 have generally shown response rates of 15-20% better responses seen in: –RCMD-RS –low EPO levels –lighter transfusion needs responses generally last 1-2 years doses: 40-60,000 units SC weekly newer compounds appear equally effective –darbepoietin (Aranesp)")
49
therapy response rates may increase up to twofold if recombinant granulocyte colony stimulating factor (G-CSF) is added generally done in a stepwise fashion doses of 1 µcg/kg day typical starting point similar difficulties in obtaining drug
 is added generally done in a stepwise fashion doses of 1 µcg/kg day typical starting point similar difficulties in obtaining drug")
50
therapy chemotherapy high-risk MDS patients with high blast counts or those who have transformed are candidates for treatment with traditional chemotherapy regimens similar to AML therapy

51
therapy epigenetic therapy DNA transcription (and normal cell growth and development) in MDS can be altered by factors not directly related to DNA sequences –chemical alterations of DNA itself –chemical changes in support proteins histones
 in MDS can be altered by factors not directly related to DNA sequences –chemical alterations of DNA itself –chemical changes in support proteins histones")
52
therapy demethylation agents: allow transcription of key tumor suppressor genes histone deacetylation agents: alter binding of DNA to histones and increase accessibility of DNA to transcription factors

53
therapy 5-azacytidine methyltransferase inhibitor delays progression of MDS improvements in blood counts in ~ 20% patients improvements in quality of life neutropenia observed as side effect (!)
")
54
therapy 5-aza-2-deoxycytabine (decitabine) similar mechanism less neutropenia & similar response rates –perhaps substantially better in some European studies availability and difficulties with awkward approved dosing schedules have been obstacles
 similar mechanism less neutropenia & similar response rates –perhaps substantially better in some European studies availability and difficulties with awkward approved dosing schedules have been obstacles")
55
therapy immune suppression antithymocyte globulin, cyclosporine –responses of 20-30% in trials –pts with relatively hypoplastic marrows appear to be better candidates immunomodulatory therapy thalidomide and lenalidomide

56
therapy thalidomide has shown promise, but has an unfavorable toxicity profile in MDS have had > 33% drop-out rates in studies

57
therapy lenalidomide (Revlimid): exciting! large improvements seen in transfusion requirements –best in 5q- patients, but also in other karyotypes –normalization of cytogenetics appears much less toxic –reversible neutropenia and thrombocytopenia availability!

58
therapy vitamins: high-dose B complex danazol: thrombocytopenia monoclonal antibodies splenectomy all may have roles in individual patients

59
therapy stem cell transplantation –Dr. L. Savoie definite role in select patients –higher-risk disease –younger patients

60
therapy: general algorithm BMT transplant candidate: young good performance status high risk MDS suitable donor YESconsider BMT NO Low risk MDS: clinical trials growth factors biological agents immune therapy High risk MDS: clinical trials leukemia-style therapy biological agents

61
The Role of the Specialty Clinic: 1. provide guidance for primary caregivers 2. maximize supportive care 3.optimize individualized management 5. dissemination of current state of knowledge 4. clinical trials & 5. data collection:

Similar presentations

















 Masood Anwar. Bone marrow failure syndromes can be defined as a group of diseases in which occurs failure on the part of bone marrow to produce.>")




