Download presentation
Presentation is loading. Please wait.

1
Agents to Treat Gastric Acidity and Gastroesophageal Reflux Disease (GERD)
Presented by Abby Roth

2
Overview Introduction Symptoms Causes Peptic Ulcer Disease H. pylori
NSAIDs GERD Treatments

3
Gastric acidity and GERD affects people of all ages, races, and gender
Who is Affected? Gastric acidity and GERD affects people of all ages, races, and gender

4
Symptoms Heartburn Acid Indigestion Regurgitation Nausea

5
Symptoms Continued Hoarseness Sore Throat Chest Pain Bad Breath
Dry Cough Asthma*

6
Symptoms in Children Vomiting Coughing Breathing Problems

7
Acid-Peptic Disorders
Peptic Ulcer Disease Occurs when there is an imbalance between the mucosal defense factors and the acid and pepsin.

8
Helicobacter pylori Infection
Causes 80% of peptic ulcers Survives the acid environment by attaching to the sugar molecules that line the stomach wall Uses the mucus layer as protection

9
H. pylori Produce large amounts of urease Urease 3 NH3 + CO2 H20 Urea

10
H. pylori Secret proteins and toxins that interact with the stomach’s epithelial cells Leads to inflammation and damage

11
NSAIDs Aspirin, Ibuprofen, Naproxen
Can have an affect at very low doses Suppresses cylooxygenase-1 Decrease production of prostaglandins

12
What is GERD? Condition where the stomach acid/content is pushed back or “refluxed” into the esophagus Affects 10 million Americans Approximately 7% have daily symptoms Link

13
GERD vs. NERD Patients suffering symptoms are placed in two groups
Non-erosive reflux disease, or NERD Erosive esophagitis Erosive esophagitis is characterized by swelling and Inflammation Barrett’s Esophagus Precursor to Esophageal Cancer

14
Causes of GERD Abnormalities with the Lower Esophageal Sphincter, or LES Stomach Abnormalities Hiatal hernia Link

15
Causes Medications NSAIDs
Calcium Channel Blockers (high blood pressure, angina)
")
16
Medications Anticholinergics (urinary tract disorders)
Beta Adrenergic Agonists (asthma) Dopamine (Parkinson’s disease)
 Dopamine (Parkinson’s disease)")
17
Causes Food and Drinks Carbonated beverages Chocolate Alcohol
Citrus Fruits Coffee or Tea Fatty foods Containing tomatoes Mint Spicy Food

18
Causes Smoking Damages mucus membranes
Impairs muscle reflexes in the throat Increases acid secretion Reduces LES function and salivation

19
Causes Obesity Laying down after a large meal Eating close to bed time
Exercise

20
Release of Gastric Acid

21
Release of Gastric acid
Histamine stimulates acid release by interacting with the histamine receptor, H2 Acetylcholine activates the cholinergic receptors Gastrin is released when food is present in the stomach

22
Treatments Antacids Alginates Sucralfate Proton Pump Inhibitors
Histamine H2-Recptor Antagonists Prokinetics New Treatments

23
Antacids Quick but short term Buffer gastric acid, increasing the pH
Neutralize acid by the following reaction Al(OH)3 + 3 HCl AlCl3 + 3 H2O
3 + 3 HCl AlCl3 + 3 H2O.")
24
Antacids Maalox Al(OH)3 (aluminum hydroxide), Mg(OH)2 (magnesium hydroxide)
3 (aluminum hydroxide), Mg(OH)2 (magnesium hydroxide)")
25
Antacids Tums CaCO3 (calcium carbonate)
")
26
Antacids Pepto-Bismol C7H5BiO4 (bismuth subsalicylate)
")
27
Antacids Alka-Seltzer NaHCO3 (sodium bicarbonate)
")
28
Alginates Alginates Usually combined with an antacid
Forms protective barrier on top of gastric contents Gaviscon Sodium Alginate, Sodium Bicarbonate, and Calcium Carbonate Link

29
Alginates Polysaccharide found in the cell walls of brown algae
Sodium alginate is the sodium salt of alginic acid

30
Alginic Acid

31
Sucralfate Reacts with stomach acid to from a cross linked viscous polymer that acts as an acid buffer Can bind to proteins on the surface of an ulcer to prevent further acid damage Has been shown to aid in healing by promoting epidermal growth factors and prostaglandins

32
Sucralfate (Carafate)
")
33
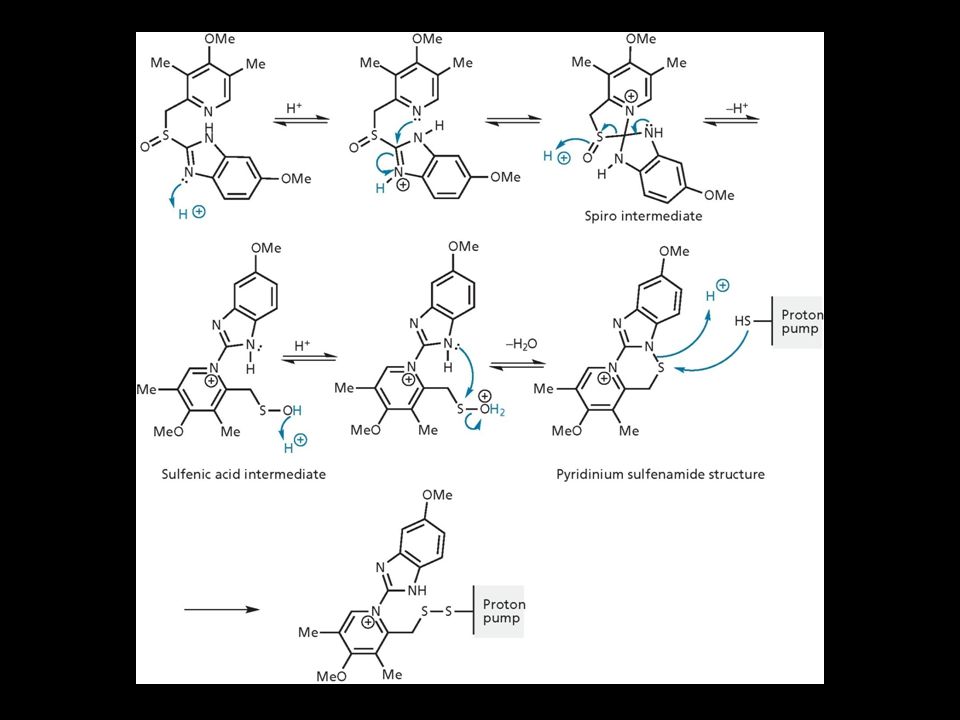
Proton Pump Inhibitors
Proton pump inhibitors (PPIs) Inhibits the gastric acid pump, H+/K+ ATPase Are prodrugs
 Inhibits the gastric acid pump, H+/K+ ATPase. Are prodrugs.")
34
PPIs Diffuse into the parietal cells of the stomach and accumulates
Activated by proton-catalyzed formation of sulfenic acid This prevents the drug from diffusing out Activated form then irreversibly binds at the sulfhydryl groups of the cysteins of the H+/K+ ATPase Link

35
Cysteine

37
PPIs Rabeprazol (Acipex)
")
38
Lansoprazole (Prevacid)
PPIs Lansoprazole (Prevacid)
")
39
Esomeprazole (Nexium)
PPIs Esomeprazole (Nexium)
")
40
PPIs Omeprazole (Prilosec) Omeprazole/sodium bicarbonate (Zegerid)
 Omeprazole/sodium bicarbonate (Zegerid)")
41
Pantoprazole (Protonix)
PPIs Pantoprazole (Protonix)
")
42
Treatments Histamine H2-recptor antagonists (H2RAs)
The hormone, histamine stimulates the release of acid by interacting with the histamine receptor, or H2 receptor. Inhibit acid secretion by competitively and reversibly blocking parietal cell H2-receptors Less potent then PPI’s

43
Agonist vs. Antagonist An agonist is a drug that produces the same response at a receptor as the natural messenger An antagonist is a drug which binds to a receptor without activating it, prevent an agonist or natural messenger from binding

44
Histamine

46
H2RAs Cimetidine (Tagamet)
")
47
H2RAs Nizatidine (Axid)
")
48
Ranitidine HCl (Zantac)
Other H2RAs Famotidine (Pepcid) Ranitidine HCl (Zantac)
 Ranitidine HCl (Zantac)")
49
Treatments Prokinetics Increase LES function
Release stomach contents by Activating serotonin receptors Acting on dopaminergic receptors

50
Metoclopramide (Reglan, Degan)
Prokinetics Metoclopramide (Reglan, Degan)
")
51
Domperidone (Motilium, Costi)
Prokinetics Domperidone (Motilium, Costi)
")
52
Prokinetics Cisapride (Prepulsid, Propulsid)
")
53
Prokinetics Rarely used because of severe side effects Fatigue Tremors
Parkinsonism Tardive Dyskinesia Severe cardiac events

54
New Treatments Cholecystokinin2 receptor antagonists (CCK2)
Potassium competitive acid blockers (P-CABs)
")
55
Treatments Cholecystokinin2 receptor antagonists (CCK2)
Block the CCK2 receptors inhibiting acid secretion Still in clinical trials Best use in combination with PPI’s

56
CCK2 Itriglumide

57
CCK2 Z-360

58
Treatments Potassium competitive acid blockers (P-CABs)
Target H+/K+ ATPase Ionically binds to the proton pump Specific for the K+ binding region and prevents acid secretion Binds reversibly Still in clinical trials

59
P-CABs Revaprazan

60
P-CABs Soraprazan

61
Treatment for H. pylori Amoxicillin + clarithromycin + proton pump inhibitor Metronidazole + clarithromycin + proton pump inhibitor Bismuth subsalicylate + metronidazole + tetracycline + proton pump inhibitor

62
Assigned Reading Vesper, J.B. et all, Gastroesophageal Reflux Diesease, Is there More to the Story?, ChemMedChem (2008), 3,
, 3,")
63
Homework Questions What is an antagonist and how do the H2RAs (histamine receptor antagonists) act as one? Explain the precise biological mechanism whereby prokinetics achieve their effect, including the receptors they act upon. Are they agonists or antagonists? Of which chemical messenger? What is a prodrug? What causes the PPI’s to become an active drug? Bacteria in the upper GI tract may play a role in GERD. Explain.

64
References Bak, Young-Tae. Management Strategies for Gastroesophageal Reflux Disease. Journal of Gastroenterology and Hepatology (2004), 19, S49-S53. Horn, J. Understanding the Pharmacodynamic and Pharmacokinetic Differences between proton pump inhibitors- focus on pKa and metabolism. AP&T (2006), 2, Pettit, M. Treatment of Gastroesophageal Reflux Disease. Pharm World Sci (2005) 27, Vakil, N., New Pharmacological Agents for the Treatment of Gastroesophageal Reflux Disease. AP&T (2006), 19, Vesper, J.B. et all, Gastroesophageal Reflux Diesease, Is there More to the Story?, ChemMedChem (2008), 3, Goodman and Gilman pg Patrick pg
, 19, S49-S53. Horn, J. Understanding the Pharmacodynamic and Pharmacokinetic Differences between proton pump inhibitors- focus on pKa and metabolism. AP&T (2006), 2, Pettit, M. Treatment of Gastroesophageal Reflux Disease. Pharm World Sci (2005) 27, Vakil, N., New Pharmacological Agents for the Treatment of Gastroesophageal Reflux Disease. AP&T (2006), 19, Vesper, J.B. et all, Gastroesophageal Reflux Diesease, Is there More to the Story , ChemMedChem (2008), 3, Goodman and Gilman pg Patrick pg")
Similar presentations
















 2004 Elsevier Inc. All rights reserved. Drugs for Peptic Ulcer Disease Chapter 73.>")



>")