Download presentation
Presentation is loading. Please wait.

1
The Global Tuberculosis Epidemic The Impact on Florida Michael Lauzardo, MD MSc Principal Investigator, Southeastern National Tuberculosis Center Deputy Health Officer for TB – State of Florida Assistant Professor, Div. of Pulmonary and Critical Care Medicine, University of Florida College of Medicine

2
Disclosure I, Dr. Mike Lauzardo, have no financial or commercial interests to disclose to the meeting participants.

3
Case presentation : The case of the wayward professor RC is a 35yo woman from a country of high TB incidence who presented to her PCP 2 years earlier c/o cough RC is a 35yo woman from a country of high TB incidence who presented to her PCP 2 years earlier c/o cough The PCP at that time placed a PPD and ordered a CXR The PCP at that time placed a PPD and ordered a CXR The PPD was 10mm and the CXR was abnormal so she was sent to a pulmonologist The PPD was 10mm and the CXR was abnormal so she was sent to a pulmonologist

4
Case 1: The wayward professor continued The pulmonologist attributed the CXR abnormality to BCG vaccination and the cough to allergies. The pulmonologist attributed the CXR abnormality to BCG vaccination and the cough to allergies. Sputum was not obtained Sputum was not obtained Lost to follow-up for two years Lost to follow-up for two years Came back to her PCP accompanied by her husband MC, A faculty member at a prominent university Came back to her PCP accompanied by her husband MC, A faculty member at a prominent university Active hemoptysis in the waiting room Active hemoptysis in the waiting room

5
Case 1: The chase begins The PCP is very concerned about TB again The PCP is very concerned about TB again A CXR is obtained and arrangements are made to have the pt seen immediately in the ER by a different pulmonologist A CXR is obtained and arrangements are made to have the pt seen immediately in the ER by a different pulmonologist They never show citing the fact that the husband does not think she has TB They never show citing the fact that the husband does not think she has TB The health department is notified The health department is notified

6
CASE 1 The pts husband is called at home and the rationale and need for evaluation is expressed in the carefully with their concerns addressed The pts husband is called at home and the rationale and need for evaluation is expressed in the carefully with their concerns addressed The plan was that the pt may go to the ER of their choosing and will be met by me to discuss the case and obtain sputum The plan was that the pt may go to the ER of their choosing and will be met by me to discuss the case and obtain sputum Patient and husband never went but sent an impostor who came to the er with a chief complaint of I dont have TB Patient and husband never went but sent an impostor who came to the er with a chief complaint of I dont have TB

7
Case 1: Lost to follow-up ( For a little while ) After much deliberation and legal wrangling the HD sent a police officer to the home to locate the family After much deliberation and legal wrangling the HD sent a police officer to the home to locate the family The officer was informed by MC That he sent his wife and kids away so that they would not be subject to the conspiracy The officer was informed by MC That he sent his wife and kids away so that they would not be subject to the conspiracy Threatening phone calls from family Threatening phone calls from family Heard nothing for 6 weeks until a call from another state on the west coast Heard nothing for 6 weeks until a call from another state on the west coast
 After much deliberation and legal wrangling the HD sent a police officer to the home to locate the family After much deliberation and legal wrangling the HD sent a police officer to the home to locate the family The officer was informed by MC That he sent his wife and kids away so that they would not be subject to the conspiracy The officer was informed by MC That he sent his wife and kids away so that they would not be subject to the conspiracy Threatening phone calls from family Threatening phone calls from family Heard nothing for 6 weeks until a call from another state on the west coast Heard nothing for 6 weeks until a call from another state on the west coast")
8
Case 1: The exciting conclusion to our story RC was diagnosed with smear positive cavitary TB after presenting to a local ER with hemoptysis once again RC was diagnosed with smear positive cavitary TB after presenting to a local ER with hemoptysis once again Placed on court-ordered dot and was banned from travel by the judge until therapy cleared her sputum Placed on court-ordered dot and was banned from travel by the judge until therapy cleared her sputum MC felt humiliated by this and immediately brought his children to the hd for evaluationskin tests were more than 25mm MC felt humiliated by this and immediately brought his children to the hd for evaluationskin tests were more than 25mm MC was evaluated with a CXR… MC was evaluated with a CXR…

10
The microbe is nothing… the terrain is everything LOUIS PASTEUR

11
Epidemiology of TB: Migrants and the Foreign Born

12
TB Epidemiology GLOBALUSA Infected cases 1.7 billion (33% population) 10 million (4% population) Case incidence 8-10 million/year ~ 13,000/year Case prevalence 40-50 million 20,000 Deaths 1.9 million/year 1,000 – 2,000/year MDR Up to 15% (DR and Ecuador) < 1%
 10 million (4% population) Case incidence 8-10 million/year ~ 13,000/year Case prevalence million 20,000 Deaths 1.9 million/year 1,000 – 2,000/year MDR Up to 15% (DR and Ecuador) < 1%")
13
A Silent Global Epidemic One-third of the worlds population infected One-third of the worlds population infected Eight million new cases of active disease per year Eight million new cases of active disease per year Two to three million deaths per year Two to three million deaths per year One person is newly infected every second and one person dies every 10 seconds One person is newly infected every second and one person dies every 10 seconds Rising incidence of drug-resistant disease Rising incidence of drug-resistant disease Billions of dollars in lost productivity Billions of dollars in lost productivity

14
9m cases annually >1/3 in populous India and China 10 000 to 99 999 100 000 to 999 999 1 000 000 or more < 1 000 1 000 to 9 999 No Estimate The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. © WHO 2002 Stop TB Department

15
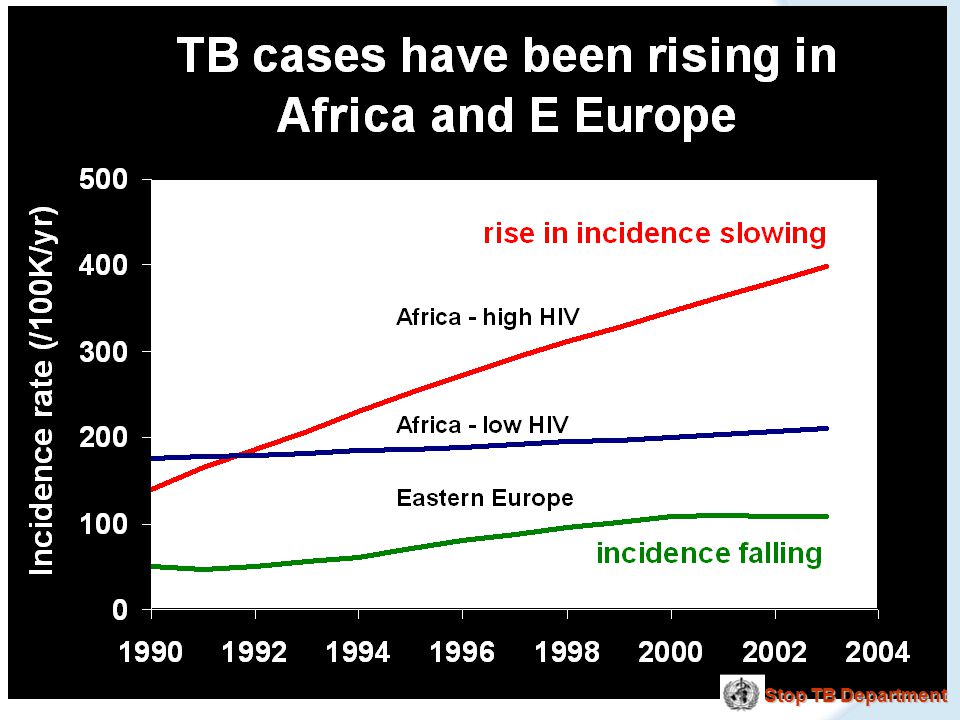
Highest TB rates per capita are in Africa linked to HIV/AIDS 25 to 49 50 to 99 100 to 299 < 10 10 to 24 300 or more No Estimate per 100 000 population The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. © WHO 2002 Stop TB Department

18
Reported TB Cases* United States, 1982–2007 Year No. of Cases *Updated as of April 23, 2008.

19
TB Morbidity United States, 2002–2007 Year No. Rate* 200215,056 5.2 200314,837 5.1 200414,501 4.9 200514,065 4.7 2006 13,754 4.6 2007 13,299 4.4 *Cases per 100,000, updated as of April 23, 2008.

20
Tuberculosis in the U.S. Epidemic Under Control 13,299 cases (4.4/100,000) in 2007 13,299 cases (4.4/100,000) in 2007 Fifteenth year of decline (down 3.3% from 2006) Fifteenth year of decline (down 3.3% from 2006) 98 cases (0.9%) of MDR-TB in 2007 98 cases (0.9%) of MDR-TB in 2007 26 states meet year 2000 elimination target (< 3.5/100,000) 26 states meet year 2000 elimination target (< 3.5/100,000) Completion of therapy exceeds 90% Completion of therapy exceeds 90%
 in ,299 cases (4.4/100,000) in 2007 Fifteenth year of decline (down 3.3% from 2006) Fifteenth year of decline (down 3.3% from 2006) 98 cases (0.9%) of MDR-TB in cases (0.9%) of MDR-TB in states meet year 2000 elimination target (< 3.5/100,000) 26 states meet year 2000 elimination target (< 3.5/100,000) Completion of therapy exceeds 90% Completion of therapy exceeds 90%.")
21
Excess TB Morbidity – U.S. 1985 - 1992 Associated factors Associated factors – Poor infrastructure – HIV epidemic – Immigration – Institutional transmission – MDR-TB JAMA 1994; 272:536

26
TB in Foreign-Born United States 2007 58% of total cases 58% of total cases 20.7 cases/100,000 population 20.7 cases/100,000 population Rate ratio Rate ratio – 9.8 relative to US-born 28 states reported > 50% foreign-born cases 28 states reported > 50% foreign-born cases

27
TB in Foreign-Born Percentage TB cases of foreign origin Andorra Malta Monaco San Marino No data 0% – 4% 5% – 19% 20% – 49% >49%

28
Number of TB Cases in U.S.-Born Versus Foreign-Born Persons, U.S. 1993-2003* # OF CASES

29
Percentage of TB Cases Among Foreign-Born Persons – United States 19932003* 50% 50% 25 – 49 % < 25%

30
Countries of Birth of Foreign-born Persons Reported with TB United States, 2007 Mexico (24%) Philippines (12%) Viet Nam (7%) India (8%) China (5%) Haiti (2%) Rep. Korea (2%) Other Countries (39%)
 Other Countries (39%).")
31
Characteristics of TB Among Migrants

32
Tuberculosis and Fear – ca. 1900 Self-preservation demands radical revision of the definition of personal liberty… The contagion of disease and vice fostered in neglected districts will spread to the prosperous areas. They daily traverse our pathway, entering as servants from contaminated huts, handling our children and every vestige of clothing and linen in our living apartments.

33
Common Misconceptions – ca. 2008 TB rates among the foreign born are high due to illegal immigration TB rates among the foreign born are high due to illegal immigration TB cases among the foreign-born represent failures of overseas screening TB cases among the foreign-born represent failures of overseas screening Most foreign-born persons with TB are poor, unemployed, and uninsured Most foreign-born persons with TB are poor, unemployed, and uninsured Foreign-born persons are less adherent to treatment Foreign-born persons are less adherent to treatment

34
Characteristics Traditionally Associated with US-born TB Homelessness Homelessness Substance abuse Substance abuse Low socioeconomic status Low socioeconomic status Member of a minority group Member of a minority group Healthcare worker Healthcare worker Elderly Elderly

35
Characteristics of Foreign-Born TB Patients- Tarrant County, Texas Immigration status Immigration status – 67 (59%) permanent – 28 (25%) undocumented – 19 (17%) non-immigrant visitors FB TB patients significantly younger than US-born (mean age 38 versus 42 years) FB TB patients significantly younger than US-born (mean age 38 versus 42 years) FB more likely to have primary drug resistance (p <.001) FB more likely to have primary drug resistance (p <.001) Weis et al. AJRCCM 2001, 953-957

36
Epidemiology of TB Among the Foreign-Born – Virginia 840 cases (51.9% of total morbidity 1998-2001) 840 cases (51.9% of total morbidity 1998-2001) – 486 (57.9%) from high burden countries – 462 (55%) arrived within five years – Younger than US-born (mean 38.9 versus 47.2 years) – Common occupations atypical among TB patients 196 cases (58% of morbidity in 2001) 196 cases (58% of morbidity in 2001) – 21 different primary languages – 91 (46.4%) required interpretive services – 129 (65.8%) uninsured Hunninghake, GM et al. AJRCCM 2003 167 (Pt 2).
..")
37
TB Among Foreign-Born Residents, New Jersey 1994-1999 2005 of 4295 cases (47%) foreign-born 2005 of 4295 cases (47%) foreign-born – FB patients resided in more affluent areas than US-born (p <.001) – More likely employed in the two years prior to diagnosis (62% versus 41% p <.001) – South Asian patients more likely to be treated by private MD Davidow, AL et al. Am J Public Health 2003 93:12007-1012.

38
Patterns of TB Transmission New York City 1990-1999 Clustering observed in 48% of strains Clustering observed in 48% of strains Non-Clustering independently associated with Non-Clustering independently associated with – Birth outside the US – Age greater than 60 – Diagnosis after 1993 Among foreign-born persons in New York City, tuberculosis largely due to progression from LTBI Among foreign-born persons in New York City, tuberculosis largely due to progression from LTBI Geng, EG et al. NEJM 2002 346:1453-1458

39
TABLE 1. TUBERCULOSIS IN U.S.-BORN AND FOREIGN-BORN PERSONS BY TIME IN THE UNITED STATES, 2004 * Complete information for date of entry in to the United States was missing for 975 foreign-born patients with tuberculosis. Total n = 14,517. Cain Et al Am J Respir Crit Care Med Vol 175 75-79 2007 Origin Time in the United States (yr) Cases in 2004 n (%) Population Population Case Rate Case Rate U.S. born 6,683 (46) 249,424,0452.7 Foreign born * Total 7,806 (54) 36,245,58221.5 1 1 1,620 (24) 1,338,814121.0 > 1 to 5 1,767 (26) 5,885,67730.0 > 5 3,444 (50) 29,021,09011.9
 Cases in 2004 n (%) Population Population Case Rate Case Rate U.S. born 6,683 (46) 249,424, Foreign born * Total 7,806 (54) 36,245, ,620 (24) 1,338, > 1 to 5 1,767 (26) 5,885, > 5 3,444 (50) 29,021,")
40
Migration to the United States and Florida

41
Estimated Migrants Entering the United States Visitors without visas ~ 30,000,000 Non-immigrant visas 27,907,139 Immigrants and refugees 411,266 Undocumented migrants ~275,000 ± ???? N = ~ 59,000,000 Status adjusters in U.S.: 679,305 Source: U.S. Department of Homeland Security, 2003 (2002 data)
.")
42
Number of Foreign-Born Persons Living in the U.S. Source: Center for Immigration Studies, 2000

43
Florida and Global Migration There are 33 million foreign-born persons living in the United States of whom 2.9 million (8.9%) live in Florida. There are 33 million foreign-born persons living in the United States of whom 2.9 million (8.9%) live in Florida. In 2004 there were over 76.8 million visitors to Florida In 2004 there were over 76.8 million visitors to Florida If Miami-Dade Countys nearly 1.2 million foreign-born residents comprised a city of their own, that city would be among the 10 largest in the nation. If Miami-Dade Countys nearly 1.2 million foreign-born residents comprised a city of their own, that city would be among the 10 largest in the nation. Of the top 100 municipalities with the highest number of foreign-born residents, 31 are in Florida. Of the top 100 municipalities with the highest number of foreign-born residents, 31 are in Florida.
 live in Florida. In 2004 there were over 76.8 million visitors to Florida In 2004 there were over 76.8 million visitors to Florida If Miami-Dade Countys nearly 1.2 million foreign-born residents comprised a city of their own, that city would be among the 10 largest in the nation. If Miami-Dade Countys nearly 1.2 million foreign-born residents comprised a city of their own, that city would be among the 10 largest in the nation. Of the top 100 municipalities with the highest number of foreign-born residents, 31 are in Florida. Of the top 100 municipalities with the highest number of foreign-born residents, 31 are in Florida..")
44
Strategies to Address the Global Epidemic

45
FIND Diagnostics

46
Lessons from the history of TB clinical trials Need to evaluate regimens, not drugs Need to evaluate regimens, not drugs – A drug may act very differently at different points in therapy (e.g., INH, PZA) – A drug may work differently in the setting of different companion drugs (e.g., moxi) May need to evaluate many regimens to find the optimal combination of potency, tolerability, and intermittency May need to evaluate many regimens to find the optimal combination of potency, tolerability, and intermittency – BMRC evaluated ~ 200 regimens to come up with DOTS
 – A drug may work differently in the setting of different companion drugs (e.g., moxi) May need to evaluate many regimens to find the optimal combination of potency, tolerability, and intermittency May need to evaluate many regimens to find the optimal combination of potency, tolerability, and intermittency – BMRC evaluated ~ 200 regimens to come up with DOTS")
47
Prospects for TB drug development Several new drugs have very potent activity in animal model of TB treatment – allowing treatment to be 2-4 months Several new drugs have very potent activity in animal model of TB treatment – allowing treatment to be 2-4 months Several new drugs appear highly active when given 1-2 times/week Several new drugs appear highly active when given 1-2 times/week No published studies yet combining these new drugs No published studies yet combining these new drugs

48
Timetable for new TB drugs Compound/product 200506070809101112131415 Moxi / gati Diarylquinoline TCM207 Otsuka compound Pyrrole LL3858 Nitroimidazole PA-824 Diamine SQ-109 New quinolones II I D II I/II I D II/III II I/II PC III II/III II PC III II/III I III/NDA III I/II III I NDA III II/III NDA III *STOP TB Working Group

49
TBTC Study 27 Proportion sputum culture-negative – moxifloxacin vs. ethambutol (both with HRZ) P=0.02 P=0.003
 P=0.02 P=")
50
Activity of moxifloxacin in combination therapy in a mouse model of TB 2.5 logs Am J Respir Crit Care Med 2004; 164:421-6

51
Tackling TB in the Foreign Born: Overseas Screening

52
Why has impact on TB in the foreign-born been small? Possible explanations Possible explanations – Migration of persons with active TB – Progression from LTBI to active TB following arrival to the US – Transmission of TB within foreign-born communities

53
Tackling TB in the Foreign-Born What will it take? Federal Government Federal Government – Support of global TB control efforts – Changes to US entry procedures State and local public health State and local public health Community practitioners Community practitioners

54
Ending Neglect Challenges Maintain TB control – focus on foreign-born Maintain TB control – focus on foreign-born – Overseas screening and stateside notification Speed TB decline Speed TB decline – Identify and treat latent infection (LTBI) Develop new tools Develop new tools – Tests (LTBI), drugs, vaccine Increase U.S. role in global elimination Increase U.S. role in global elimination Mobilize support and measure progress Mobilize support and measure progress

55
Estimated Migrants Entering the United States Visitors without visas ~ 30,000,000 Non-immigrant visas 27,907,139 Immigrants and refugees 411,266 Undocumented migrants ~275,000 ± ???? N = ~ 59,000,000 Status adjusters in U.S.: 679,305 Source: U.S. Department of Homeland Security, 2003 (2002 data)
.")
56
Objectives of Overseas TB Screening Objectives of Overseas TB Screening Restrict travel/entry of persons with infectious TB Restrict travel/entry of persons with infectious TB – Class A TB (AFB-smear positive) Identify persons with suspect TB requiring follow-up stateside evaluation, and notify receiving jurisdictions of US arrival Identify persons with suspect TB requiring follow-up stateside evaluation, and notify receiving jurisdictions of US arrival
 Identify persons with suspect TB requiring follow-up stateside evaluation, and notify receiving jurisdictions of US arrival Identify persons with suspect TB requiring follow-up stateside evaluation, and notify receiving jurisdictions of US arrival")
57
Current Challenges and Opportunities Quality assurance of overseas TB screening Quality assurance of overseas TB screening Limitations of screening algorithm Limitations of screening algorithm – Sensitivity and specificity – Diagnostic tools – Local resources Timely state-side notification, follow-up, and interventions Timely state-side notification, follow-up, and interventions Expansion of scope and underlying objectives Expansion of scope and underlying objectives

58
Public Health

59
Completing Treatment – Challenges Common obstacles to completing treatment include Common obstacles to completing treatment include – Cultural and linguistic factors – Lifestyle differences – Homelessness – Substance abuse – Patient-related – System-related

60
Technical Instructions for Panel Physicians 2007

62
Technical Instructions for Tuberculosis Screening and Treatment for Panel Physicians To prevent applicants with smear-positive tuberculosis from traveling to the United States, the 1991 system relies on chest radiograph findings and sputum smears among overseas foreign national applicants 15 years of age or older. To prevent applicants with smear-positive tuberculosis from traveling to the United States, the 1991 system relies on chest radiograph findings and sputum smears among overseas foreign national applicants 15 years of age or older. The 1991 system misses applicants with smear-negative but culture-positive tuberculosis, as well as tuberculosis in applicants <15 years of age. The 1991 system misses applicants with smear-negative but culture-positive tuberculosis, as well as tuberculosis in applicants <15 years of age. Moreover, the 1991 requirements do not provide guidance specifying the quality of treatment applicants with tuberculosis should receive prior to travel. Moreover, the 1991 requirements do not provide guidance specifying the quality of treatment applicants with tuberculosis should receive prior to travel.

63
Changes in the 2007 Technical Instructions for Tuberculosis Screening Tuberculin skin tests (TST) for applicants 20 per 100,000. Tuberculin skin tests (TST) for applicants 20 per 100,000. All applicants <15 years of age with TST 5 mm will be required to have a chest radiograph. All applicants <15 years of age with TST 5 mm will be required to have a chest radiograph. Mycobacterial cultures for applicants with chest radiographs suggestive of tuberculosis disease. Mycobacterial cultures for applicants with chest radiographs suggestive of tuberculosis disease. Treatment under a directly observed therapy (DOT) program. Treatment under a directly observed therapy (DOT) program. Completion of treatment prior to immigrating to the United States, according to American Thoracic Society/CDC/Infectious Diseases Society of America guidelines. Completion of treatment prior to immigrating to the United States, according to American Thoracic Society/CDC/Infectious Diseases Society of America guidelines. New TB classifications for all applicants with suspected latent Mycobacterium tuberculosis infection and for contacts for cases of tuberculosis disease. New TB classifications for all applicants with suspected latent Mycobacterium tuberculosis infection and for contacts for cases of tuberculosis disease.
 for applicants 20 per 100,000. All applicants <15 years of age with TST 5 mm will be required to have a chest radiograph. All applicants <15 years of age with TST 5 mm will be required to have a chest radiograph. Mycobacterial cultures for applicants with chest radiographs suggestive of tuberculosis disease. Mycobacterial cultures for applicants with chest radiographs suggestive of tuberculosis disease. Treatment under a directly observed therapy (DOT) program. Treatment under a directly observed therapy (DOT) program. Completion of treatment prior to immigrating to the United States, according to American Thoracic Society/CDC/Infectious Diseases Society of America guidelines. Completion of treatment prior to immigrating to the United States, according to American Thoracic Society/CDC/Infectious Diseases Society of America guidelines. New TB classifications for all applicants with suspected latent Mycobacterium tuberculosis infection and for contacts for cases of tuberculosis disease. New TB classifications for all applicants with suspected latent Mycobacterium tuberculosis infection and for contacts for cases of tuberculosis disease..")
64
Tackling TB in the Foreign-Born What will it take? Federal government Federal government – Support of global TB control efforts – Changes to US entry procedures State and local public health State and local public health – Effective diagnostic and treatment services – Culturally-competent case-management Community practitioners Community practitioners – Efficient diagnosis and treatment – Communication and advocacy

65
Give me your tired, your poor, your huddled masses...

66
Conclusion

Similar presentations

























 201-5414 Tuberculosis surveillance data for Minnesota are available on.>")
