Download presentation
Presentation is loading. Please wait.

1
Antibody Identification
Renee Wilkins, PhD, MLS(ASCP)cm CLS 325/435 School of Health Related Professions University of Mississippi Medical Center
cm. CLS 325/435. School of Health Related Professions. University of Mississippi Medical Center.")
2
The Basics….. As you recall,
Antibody Screens use 2 or 3 Screening Cells to “detect” if antibodies are present in the serum If antibodies are detected, they must be identified… present Not present

3
Why do we need to identify?
Antibody identification is needed for transfusion purposes and is an important component of compatibility testing It will identify any unexpected antibodies in the patient’s serum If a person with an antibody is exposed to donor cells with the corresponding antigen, serious side effects can occur

4
Key Concepts In blood banking, we test “knowns” with “unknowns”
When detecting and/or identifying antibodies, we test patient serum (unknown) with reagent RBCs (known) Known: Unknown: Reagent RBCs + patient serum Reagent antisera + patient RBCs
 with reagent RBCs (known) Known: Unknown: Reagent RBCs + patient serum. Reagent antisera + patient RBCs.")
5
Reagent RBCs Screening Cells and Panel Cells are the same with minor differences: Screening cells Antibody detection Sets of 2 or 3 vials Panel cells Antibody identification At least 10 vials per set

6
Antibody Panel vs. Screen
An antibody panel is just an extended version of an antibody screen The screen only uses 2-3 cells:

7
Antibody Panel An antibody panel usually includes at least 10 panel cells:

8
Panel Group O red blood cells

9
Panel Each of the panel cells has been antigen typed (shown on antigram) + refers to the presence of the antigen 0 refers to the absence of the antigen Example: Panel Cell #10 has 9 antigens present: c, e, f, M, s, Leb, k, Fya, and Jka

10
Patient RBCs + Patient serum
Panel An autocontrol should also be run with ALL panels Autocontrol Patient RBCs Patient serum

11
Panel The same phases used in an antibody screen are used in a panel
IS 37° AHG

12
2 drops of the patients serum
Antibody ID Testing A tube is labeled for each of the panel cells plus one tube for AC: 1 2 3 4 5 6 7 8 9 10 11 AC 1 drop of each panel cell + 2 drops of the patients serum

13
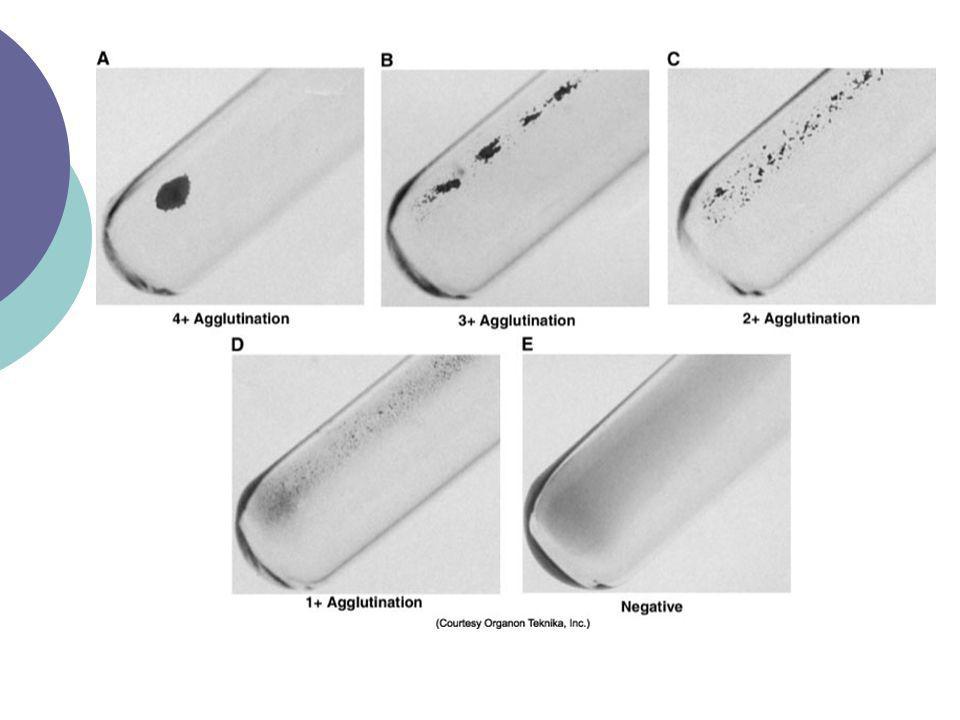
IS Phase Perform immediate spin (IS) and grade agglutination; inspect for hemolysis Record the results in the appropriate space as shown: 2+ Last tube

14
(LISS) 37°C Phase 2 drops of LISS are added, mixed and incubated for minutes Centrifuge and check for agglutination Record results

17
(LISS) 37°C Phase 2+ 2+ 2+ 2+
 37°C Phase")
18
IAT Phase (or AHG) Indirect Antiglobulin Test (IAT) – we’re testing whether or not possible antibodies in patient’s serum will react with RBCs in vitro To do this we use the Anti-Human Globulin reagent (AHG) Polyspecific Anti-IgG Anti-complement
 – we’re testing whether or not possible antibodies in patient’s serum will react with RBCs in vitro. To do this we use the Anti-Human Globulin reagent (AHG) Polyspecific. Anti-IgG. Anti-complement.")
19
AHG Phase Wash cells 3 times with saline (manual or automated)
Add 2 drops of AHG and gently mix Centrifuge Read Record reactions

20
AHG Phase 2+ 2+ 2+ 2+

21
….add “check” cells to any negative AHG !
And don’t forget…. ….add “check” cells to any negative AHG !

22
All cells are negative at AHG, so add “Check” Cells
IS LISS 37° AHG CC 2+ All cells are negative at AHG, so add “Check” Cells

23
You have agglutination…now what?
CC 2+ 2+ 2+ 2+ ??

24
Interpreting Antibody Panels
There are a few basic steps to follow when interpreting panels “Ruling out” means crossing out antigens that did not react Circle the antigens that are not crossed out Consider antibody’s usual reactivity Look for a matching pattern

25
Always remember: An antibody will only react with cells that have the corresponding antigen; antibodies will not react with cells that do not have the antigen

26
Here’s an example:

27
1. Ruling Out 2+ 2+ 2+ 2+ Cross out antigens that show NO REACTION in any phase; do NOT cross out heterozygous antigens that show dosage.

28
2. Circle antigens not crossed out
2+ 2+ 2+ 2+

29
3. Consider antibody’s usual reactivity
2+ 2+ 2+ 2+ Lea is normally a Cold-Reacting antibody (IgM), so it makes sense that we see the reaction in the IS phase of testing; The E antigen will usually react at warmer temperatures
, so it makes sense that we see the reaction in the IS phase of testing; The E antigen will usually react at warmer temperatures.")
30
4. Look for a matching pattern
E doesn’t match and it’s a warmer rx Ab 2+ 2+ 2+ 2+ …Yes, there is a matching pattern!

31
Interpretation anti-Lea

32
Guidelines Again, it’s important to look at: Autocontrol Phases
Negative - alloantibody Positive – autoantibody or DTR (i.e.,alloantibodies) Phases IS – cold (IgM) 37° - cold (some have higher thermal range) or warm reacting AHG – warm (IgG)…significant!! Reaction strength 1 consistent strength – one antibody Different strengths – multiple antibodies or dosage DTR – delayed transfusion reaction (donor cells are sensitized with patient’s antibody)
 Phases. IS – cold (IgM) 37° - cold (some have higher thermal range) or warm reacting. AHG – warm (IgG)…significant!! Reaction strength. 1 consistent strength – one antibody. Different strengths – multiple antibodies or dosage. DTR – delayed transfusion reaction (donor cells are sensitized with patient’s antibody)")
33
About reaction strengths……
Strength of reaction may be due to “dosage” If panel cells are homozygous, a strong reaction may be seen If panel cells are heterozygous, reaction may be weak or even non-reactive Panel cells that are heterozygous should not be crossed out because antibody may be too weak to react (see first example)
")
34
Guidelines (continued)
Matching the pattern Single antibodies usually shows a pattern that matches one of the antigens (see previous panel example) Multiple antibodies are more difficult to match because they often show mixed reaction strengths
 Multiple antibodies are more difficult to match because they often show mixed reaction strengths.")
35
Rule of three The rule of three must be met to confirm the presence of the antibody A p-value ≤ 0.05 must be observed This gives a 95% confidence interval How is it demonstrated? Patient serum MUST be: Positive with 3 cells with the antigen Negative with 3 cells without the antigen

36
Our previous example fulfills the “rule of three”
2+ 3 Positive cells 2+ 2+ 3 Negative cells 2+ Panel Cells 1, 4, and 7 are positive for the antigen and gave a reaction at immediate spin Panel Cells 8, 10, and 11 are negative for the antigen and did not give a reaction at immediate spin

37
What if the “rule of three” is not fulfilled?
If there are not enough cells in the panel to fulfill the rule, then additional cells from another panel could be used Most labs carry different lot numbers of panel cells

38
Phenotyping In addition to the rule of three, antigen typing the patient red cells can also confirm an antibody How is this done? Only perform this if the patient has NOT been recently transfused (donor cells could react) If reagent antisera (of the suspected antibody) is added to the patient RBCs, a negative reaction should result…Why?
 If reagent antisera (of the suspected antibody) is added to the patient RBCs, a negative reaction should result…Why")
39
Remember Landsteiner’s Rule
Individuals DO NOT make allo-antibodies against antigens they have

40
Multiple antibodies Multiple antibodies may be more of a challenge than a single antibody Why? Reaction strengths can vary Matching the pattern is difficult

41
So what is a tech to do? Several procedures can be performed to identify multiple antibodies Selected Cells Neutralization Chemical treatment Proteolytic enzymes Sulfhydryl reagents ZZAP

42
Selected Cells Selected cells are chosen from other panel or screening cells to confirm or eliminate the antibody The cells are “selected” from other panels because of their characteristics The number of selected cells needed depends on how may antibodies are identified

43
Selected Cells Every cell should be positive for each of the antibodies and negative for the remaining antibodies For example: Let’s say you ran a panel and identified 3 different antibodies: anti-S, anti-Jka, and anti-P1 Selected cells could help…

44
Selected Cells Selected cells S Jka P1 IS LISS 37° AHG #1 + 2+ #5 3+
2+ #5 3+ #8 These are panel cells that are being used, I just didn’t include the rest of the antigram because it is not necessary. These results show that instead of 3 antibodies, there are actually 2: anti-S and anti-Jka

45
Neutralization Some antibodies may be neutralized as a way of confirmation Commercial “substances” bind to the antibodies in the patient serum, causing them to show no reaction when tested with the corresponding antigen (in panel)
")
46
Neutralization Manufacturer’s directions should be followed and a dilutional control should always be used The control contains saline and serum (no substance) and should remain positive A control shows that a loss of reactivity is due to the neutralization and not to the dilution of the antibody strength when the substance is added
 and should remain positive. A control shows that a loss of reactivity is due to the neutralization and not to the dilution of the antibody strength when the substance is added.")
47
Neutralization Common substances
P1 substance (sometimes derived from hydatid cyst fluid) Lea and Leb substance (soluble antigen found in plasma and saliva) I substance can be found in breast milk Sda substance derived from human or guinea pig urine **you should be aware that many of these substances neutralize COLD antibodies; Cold antibodies can sometimes mask more clinically significant antibodies (IgG), an important reason to use neutralization techniques
 Lea and Leb substance (soluble antigen found in plasma and saliva) I substance can be found in breast milk. Sda substance derived from human or guinea pig urine. **you should be aware that many of these substances neutralize COLD antibodies; Cold antibodies can sometimes mask more clinically significant antibodies (IgG), an important reason to use neutralization techniques.")
48
Enzymes (proteolytic)
Can be used to enhance or destroy certain blood group antigens Several enzymes exist: Ficin (figs) Bromelin (pineapple) Papain (papaya) In addition, enzyme procedures may be One-step Two-step
 Bromelin (pineapple) Papain (papaya) In addition, enzyme procedures may be. One-step. Two-step.")
49
Enzymes Enzymes remove the sialic acid from the RBC membrane, thus “destroying” it and allowing other antigens to be “enhanced” Antigens destroyed: M, N, S, s, Duffy Antigens enhanced: Rh, Kidd, Lewis, I, and P

50
Enzyme techniques One-stage Two-stage
Enzyme is added directly to the serum/cell mixture Two-stage Panel cells are pre-treated with enzyme, incubated and washed Patient serum is added to panel cells and tested

51
Enzyme techniques If there is no agglutination after treatment, then it is assumed the enzymes destroyed the antigen

52
Enzyme treatment Duffy antigens destroyed Kell antigens not affected
Enzyme treament Anti-K Perfect match for anti-Fya Duffy antigens destroyed Kell antigens not affected

53
Sulfhydryl Reagents Cleave the disulfide bonds of IgM molecules and help differentiate between IgM and IgG antibodies Good to use when you have both IgG and IgM antibodies (warm/cold) Dithiothreitol (DTT) is a thiol and will denature Kell antigens 2-mercaptoethanol (2-ME)
 Dithiothreitol (DTT) is a thiol and will denature Kell antigens. 2-mercaptoethanol (2-ME)")
54
ZZAP A combination of proteolytic enzymes and DTT
Denatures Kell, M, N, S, Duffy and other less frequent blood group antigens Does not denature the Kx antigen Good for adsorption techniques “frees” autoantibody off patient’s cell, so that autoantibody can then be adsorbed onto another RBC

55
Autoantibodies…. Warm & Cold Reacting

56
Autoantibodies Autoantibodies can be cold or warm reacting
A positive autocontrol or DAT may indicate that an auto-antibody is present Sometimes the autocontrol may be positive, but the antibody screening may be negative, meaning something is coating the RBC

57
Getting a positive DAT We have focused a lot on the IAT used in antibody screening and ID, but what about the DAT? The direct antiglobulin test (DAT) tests for the in vivo coating of RBCs with antibody (in the body) AHG is added to washed patient red cells to determine this
 tests for the in vivo coating of RBCs with antibody (in the body) AHG is added to washed patient red cells to determine this.")
58
What can the DAT tell us? Although not always performed in routine pretransfusion testing, a positive DAT can offer valuable information If the patient has been transfused, the patient may have an alloantibody coating the transfused cells If the patient has NOT been transfused, the patient may have an autoantibody coating their own cells

59
Identifying autoantibodies
Auto-antibodies can sometimes “mask” clinically significant allo-antibodies, so it’s important to differentiate between auto- and allo-antibodies

60
Cold autoantibodies React at room temperature with most (if not all) of the panel cells and give a positive autocontrol The DAT is usually positive with anti-C3 AHG (detects complement) Could be due to Mycoplasma pneumoniae, infectious mono, or cold agglutinin disease
 Could be due to Mycoplasma pneumoniae, infectious mono, or cold agglutinin disease.")
61
Cold autoantibodies Mini-cold panels can be used to help identify cold autoantibodies Since anti-I is a common autoantibody, cord blood cells (no I antigen) are usually included Group O individual with cold autoanti-I Group A individual with cold autoanti-IH Anti-IH is reacting weakly with the cord cells (some H antigen present)
 are usually included. Group O individual with cold autoanti-I. Group A individual with cold autoanti-IH. Anti-IH is reacting weakly with the cord cells (some H antigen present)")
62
Avoiding reactivity Cold autoantibodies can be a nuisance at times. Here are a few ways to avoid a reaction: Use anti-IgG AHG instead of polyspecific. Most cold antibodies react with polyspecific AHG and anti-C AHG because they fix complement Skipping the IS phase avoids the attachment of cold autoantibodies to the red cells Use 22% BSA instead of LISS

63
Other techniques If the antibodies remain, then prewarmed techniques can be performed: Red cells, serum, and saline are incubated at 37° before being combined Autoadsorption is another technique in which the autoantibody is removed from the patients serum using their own red cells The serum can be used to identify any underlying alloantibodies

64
Warm autoantibodies More common that cold autoantibodies
Positive DAT due to IgG antibodies coating the red cell Again, the majority of panel or screening cells will be positive The Rh system (e antigen) seems to be the main target although others occur
 seems to be the main target although others occur.")
65
Warm autoantibodies Cause warm autoimmune hemolytic anemia (WAIHA)…H&H How do you get a warm autoantibody? Idiopathic Known disorder (SLE, RA, leukemias, UC, pregnancy, infectious diseases, etc) Medications Several techniques are used when warm autoantibodies are suspected…
 Medications. Several techniques are used when warm autoantibodies are suspected…")
66
Elution (whenever DAT is positive)
Elution techniques “free” antibodies from the sensitized red cells so that the antibodies can be identified Y Elution Y Y Y Y Sensitized RBC Y Y Y Y Y Positive DAT Frees antibody Antibody ID

67
Elution The eluate is a term used for the removed antibodies
Testing the eluate is useful in investigations of positive DATs HDN Transfusion reactions Autoimmune disease The red cells can also be used after elution for RBC phenotyping if needed When tested with panel cells, the eluate usually remains reactive with all cells if a warm autoantibody is present

68
Elution Methods Acid elutions (glycine acid)
Most common Lowers pH, causing antibody to dissociate Organic solvents (ether, chloroform) Dissolve bilipid layer of RBC Heat (conformational change) Freeze-Thaw (lyses cells) ABO antibodies
 Dissolve bilipid layer of RBC. Heat (conformational change) Freeze-Thaw (lyses cells) ABO antibodies.")
69
Adsorption Adsorption procedures can be used to investigate underlying alloantibodies ZZAP or chloroquine diphosphate can be used to dissociate IgG antibodies from the RBC (may take several repeats) After the patient RBCs are incubated, the adsorbed serum is tested with panel cells to ID the alloantibody (if present)
 After the patient RBCs are incubated, the adsorbed serum is tested with panel cells to ID the alloantibody (if present)")
70
Adsorption Two types: Autoadsorption
No recent transfusion Autoantibodies are removed using patient RBCs, so alloantibodies can be identified Allogenic (Differential) adsorption If recently transfused Uses other cells with the patients serum
 adsorption. If recently transfused. Uses other cells with the patients serum.")
71
Remove serum and test for alloantibody
2 tubes Wash x3 after incubation Centrifuge after incubating; and transfer serum to 2nd tube of treated cells; incubate and centrifuge again

72
More reagents…. Many of elution tests can damage the antigens on the RBC Choroquine diphosphate (CDP) and glycine acid EDTA reagents can dissociate IgG from the RBC without damaging the antigens Very useful if the RBC needs to be antigen typed
 and glycine acid EDTA reagents can dissociate IgG from the RBC without damaging the antigens. Very useful if the RBC needs to be antigen typed.")
73
Chloroquine diphosphate
Quinilone derivative often used as an antimalarial May not remove autoantibody completely from DAT positive cells Partial removal may be enough to antigen type the cells or to be used for autoadsorption of warm autoantibodies

74
THE END!!

Similar presentations

 and Elution/Eluate Testing>")













>")



