Download presentation
Presentation is loading. Please wait.

1
Eddie L. Patton, M.D., M.S. Cecile L. Phan, M.D., F.R.C.P.C. Yadollah Harati, M.D., F.A.C.P.

2
History 71 year old man with a 30 year history of progressive extremity numbness, weakness and wasting and received a diagnosis of Charcot Marie Tooth disease Several years after onset of numbness he developed balance problems to the point that by the time of his presentation he could not stand without holding on to something He developed a tremor in his hands starting in the mid 1980s and was referred to our movement disorders clinic by his brother, a physician, for possible DBS

3
History PMH- Renal calculi PSH- Lithotripsy, hernia repair Allergies- NKDA Med- primidone, hydrochlorothiazide FH- He has four siblings and two children with no neurological problems No family history of CMT

4
Examination Tone- Decreased in his extremities Atrophy- Severe atrophy of the intrinsic muscles of the hand, legs (anterior and posterior department), and forearms (extensor and flexor compartments) Reflexes- Areflexic throughout Gait- Very unsteady, wide based, with bilateral foot drop. He was unable to stand without support

5
Examination Sensory Exam Vibration- absent at the toes and ankles, significantly reduced at the knees Joint position- Absent at the toes and ankles bilaterally Pin prick- symmetrical reduction in stocking and glove pattern up to mid shins and mid forearm Coordination- Dysmetria bilaterally to finger to nose and heel to shin

6
Motor Exam RightLeft Deltoids5- Biceps55 Triceps55 Wrist Extension4+ Wrist Flexion5- Digit Extension11 Digit Flexion22 Interossei11 Illiopsoas55 Knee flexors/extensors55 Tibialis anterior00 Gastrocnemius/soleus00 Toe flexion00 Toe extension00

7
Exam and further questions…

8
EMG/NCS Motor Nerve Conductions- right median, ulnar, peroneal, tibilal and femoral nerves were all non-conductable Spinal accessory and axillary- severe delayed distal latencies and severe reduction in distal amplitudes Sensory Nerve Conductions- absent median, ulnar and sural nerve conductions on the right EMG- diffuse moderate denervation proximally and distally with moderate amount of spontaneous activity

9
EMG/NCS Summary Severe diffuse motor and sensory demyelinating polyneuropathy, distal greater than proximal, with moderate amount of axonal loss.

10
Work-up Complete CMT genetic evaluation- normal MAG IgM antibody- 191 (N) CSF analysis WBC-4 Glucose- 57 Protein- 364 Increased IgG synthesis rate and IgG index Decided at this point to perform a nerve biopsy
 CSF analysis WBC-4 Glucose- 57 Protein- 364 Increased IgG synthesis rate and IgG index Decided at this point to perform a nerve biopsy")
11
Median Antebrachial Nerve

12
Nerve Biopsy H&E- Moderatly severe decreased density of myelinated fibers

13
Nerve Biopsy Trichrome: Myelin digestive chamber Semi-thin: Many small thinly myelinated fibers

14
Nerve Biopsy Teased: Note variation in myelin thickness

15
Nerve Biopsy Moderately severe depopulation of myelinated nerve fibers. 17% of teased fibers display evidence of dymelination/remyelination. Majority of fibers on semi-thin are small and thinly myelinated, without clusters. There were no onion bulbs noted. Findings suggest a chronic, moderately severe demyelinating neuropathy

16
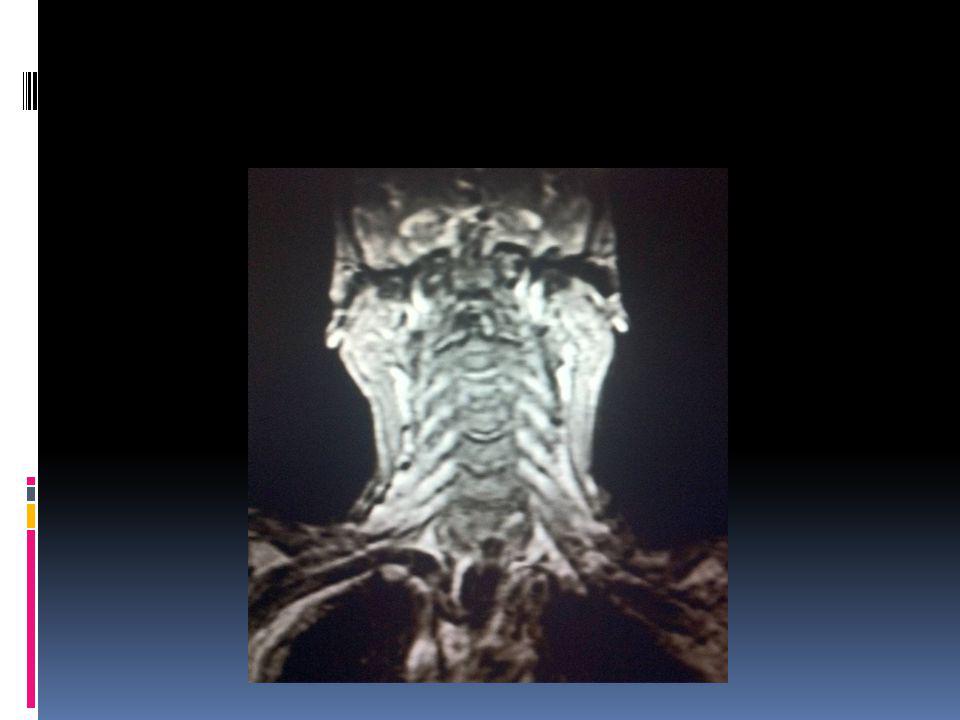
Imaging MRI Brain- No acute abnormalities MRI- cervical spine- enlargement of his cervical spine nerve roots

19
At this point we concluded this was not CMT based on Negative family history Absent onion bulbs on nerve biopsy Marked elevated CSF protein Negative genetic CMT evaluation

20
Diagnosis Undiagnosed Untreated Chronic Inflammatory Demyelinating Polyneuropathy

21
Treatment Initial course of IV Methylprednisolone at 1000 mg daily for 5 days Weekly IVMP 1000 mg boosters for 4 weeks Good response He was then switched to IVIG Initial 5 day course followed by weekly boosters

22
Nerve root involvement in CIDP One of the first papers written about this was by Crino, Grossman and Rostami, Magnetic Resonance Imaging of the Cauda Equina in Chronic Inflammatory Demyelinating Polyneuropathy Annals of Neurology 1993 33 y/o man with 5 week history of progressive weakness and unsteady gait, CSF protein 305,WBC 5 Nerve conduction studies and sural nerve biopsy consistent with demyelinating polyneuropathy

23
Crino et al MRI of his lumbar/sacrum- Enhancement of the cauda equina Enhancement suggests inflammation and compromise of BB barrier Authors suggest that MRI could prove to be useful adjunctive study when suspecting CIDP

24
Nerve root hypertrophy in CIDP Tazawa et al, Spinal Nerve Root Hypertrophy on MRI: Clinical Significance in the Diagnosis of Chronic Inflammatory Demyelinating Polyradiculoneuropathy Internal Medicine 14 patients with CIDP and 10 controls (6 healthy and 4 other neurological condition) Electrophysiological studies done in medial and tibial nerves in side most effected Compared this with MRI findings (STIR images) of cervical and lumbar nerve roots
 Electrophysiological studies done in medial and tibial nerves in side most effected Compared this with MRI findings (STIR images) of cervical and lumbar nerve roots")
25
Tazawa et al Note marked hypertrophy in cervical nerve roots

26
Tazama et al Conclusion Patients with CIDP showed significantly enlargement of cervical and lumbar spinal roots on MRI compared to control Cervical spine- 6.0-6.8 mm (normal < 5 mm) Lumbar spine- 7.3-10.4 mm Hypertrophic nerve root changes correlate with electrophysiological indices F-wave conduction velocity of median and tibial nerves have a negative correlation to corresponding nerve roots
 Lumbar spine mm Hypertrophic nerve root changes correlate with electrophysiological indices F-wave conduction velocity of median and tibial nerves have a negative correlation to corresponding nerve roots")
27
Please tell us how you are responding to treatment…

Similar presentations




 Group of autoimmune conditions involving demyelination and acute axonal degeneration.>")







 Prickly numbness.>")







